FAQs: Antimicrobial Resistance (AR) Option
General Submission Requirements
NHSN requires a Monthly Reporting Plan for every month that you plan to submit AR data.
- From the NHSN Homepage, select “Reporting Plan” from the left side menu.
- Click Add and select “Monthly Reporting Plan” for the Reporting Plan Type to add a new Monthly Reporting Plan, or click Find to find an existing plan.
- Select the month and year for the AR data submission.
- If editing an existing plan, first scroll down to the bottom of the page and click “Edit”. Then scroll to the “Antimicrobial Use and Resistance Module” section of the plan.
- See example screenshot and details below for guidance in selecting the Locations on Monthly Reporting Plan:
- Select Facility-wide Inpatient (FacWideIN) and check the AR box to submit AR Option data for inpatient locations. Do not list individual inpatient locations in the AR Option plan.
- If applicable, select an allowed outpatient location type (specifically Emergency Department [ED], Pediatric ED, and 24-hour Observation Area) and check the AR box to submit for that specific outpatient location. List the outpatient locations as separate lines in the Monthly Reporting Plan.
- Click Save at the bottom of the screen.

Note: You do not have to check the AU boxes unless you also plan to submit AU Option data.
Please note that the AUR Measure of the CMS Promoting Interoperability Program is attestation-based, so CDC will not share AUR data with CMS, even if it is included in the Monthly Reporting Plan. View the complete list of data required for each CMS Quality Reporting Program [PDF – 1 MB].
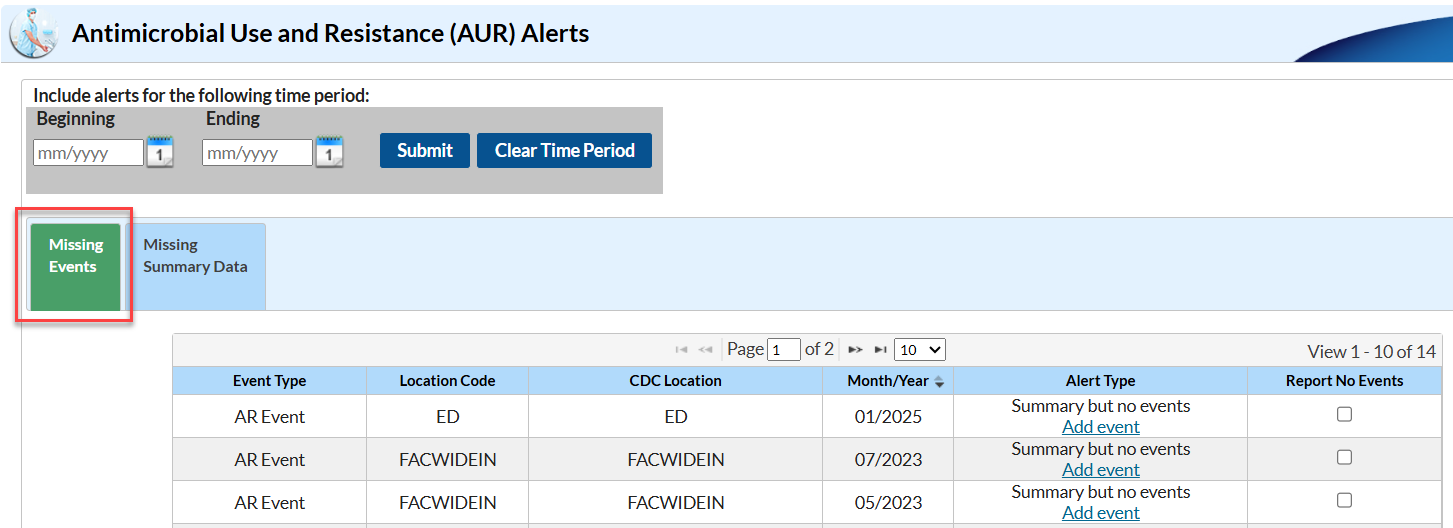
The NHSN Alerts tell you that you haven’t yet submitted data for something listed in your Monthly Reporting Plan. The Missing Event alert specifically tells you that you have reported AR Option summary data for those location/month(s), but you have not yet reported AR Events. Missing AR Event alerts will appear within the AUR alerts section on the Missing Events tab of the alert screen as shown in the screenshot below:
To clear the Missing Event alerts, you will need to submit the AR Event CDA files for the month(s) listed on your alerts screen. If you thought you had already uploaded these data, there is a good chance an error occurred during the original upload process and these specific files failed to import. During the re-submission process, make sure you pay special attention to any errors that may show up on the PDF submission report. Once you have uploaded these data, be sure to generate new datasets.
It would be rare, but not unheard of, to have zero AR Events to report for a given month based on the criteria for determining whether something is an AR Event. For example, any urine specimen in which E. coli was cultured would be eligible to be reported regardless of the susceptibility of that organism to the drugs tested by the lab. However, if there were zero specimens collected with eligible organisms for these months, you can click the “Report No Events” box for the month(s) in question on the Alerts screen. View our guide for more information on how to report no events [PDF – 395 KB].
If you do not yet have AR Event reporting from your vendor software set up, we request that instead of clicking the “Report No Events” box, you remove the AR Option check boxes on your Monthly Reporting Plan for the time being. Clicking the “Report No Events” box, tells NHSN that your facility identified no specimens that met the criteria for an AR Event (in other words, a “true zero”). It would not be appropriate to “Report No Events” because you were not able to report AR Events from your vendor software. See Q5 in the General Submission Requirements section for how to edit the Monthly Reporting Plan.
The Missing Summary Data alert specifically tells you that you have not yet reported AR summary records for those location(s)/month(s) listed in your Monthly Reporting Plan. Missing AR Summary alerts will appear within the AUR alerts section on the Missing Summary tab of the alert screen as shown in the screenshot below:

To clear the Missing Summary Data alerts, you will need to submit the AR summary records (also known as the “denominator” data) for the month(s) listed on your alerts screen. If you thought you had already uploaded these data, there is a good chance an error occurred during the original upload process and these specific files failed to import or these summary files were not included in your original zip file submission. During the re-submission process, make sure you pay special attention to any errors that may show up on the PDF submission report. Once you have uploaded these data, be sure to generate new datasets.
Specimen Sources
Data Import
Sometimes, when you are uploading many AR files, some files will successfully upload, and others will not. Below is a screenshot of what it looks like when you submit files together and you have some records pass and others fail. Note that both the Error Report and Submit buttons are enabled:

If you click on the Events tab in the Validation Results table, you can see the files that passed and failed validation by looking in the Status column. In this instance, 13 records were submitted. Four passed validation and nine failed. When you click the Submit button, only the four files that successfully passed validation will upload into NHSN. Clicking the submit button generates a PDF report, which shows the file(s) that successfully imported and the file(s) that did not pass validation and did not import (see example screenshot below).

Please view and save the PDF report for your records each time you import data into the AR Option. The above example of the PDF report shows you which files passed validation and which files failed validation. For each file that failed, the reasons for failure are included in the section below the record information. The NHSN Help Desk requires information from the PDF report to assist users with inquiries related to data import errors.
Import Errors
The location in the CDA file must be the exact match of the “Your Code” value, “NHSN HL7 code” and location type of the values in the NHSN Location Manager (see screenshot below). This error message is telling you that the location name used in your CDA file does not match a location currently mapped in your NHSN facility.
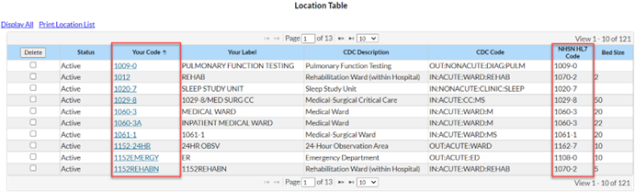
We recommend meeting with your NHSN Facility Administrator to have them export the location list out of NHSN (Facility > Locations > Export Location List) so you can compare what’s in NHSN to what’s in your vendor system. Decide the best way to rectify the differences (update NHSN or update the vendor software) with your Infection Control/Infection Prevention department. Once you’ve matched the locations across both systems, re-export your AR CDA files and import them into NHSN.
Data Deletion
There are two options for correcting AR Summary files:
- Manually delete and re-upload a new file
- Use Succession Management within vendor software
Manual Deletion: To manually delete the record, log into NHSN, select ‘Summary Data’ from the navigation menu on the left side and then select ‘Delete AUR Data’. Use the Summary Data Type drop down menu to select ‘Antimicrobial Resistance Data.’ Select the Location Code (for example, FACWIDEIN, Emergency Department), and use the Month and Year drop down menus to select the month/year you’d like to delete from NHSN. Then click the ‘Delete’ button to delete the record. See the screen shot below for reference.

Succession Management: Your vendor software may be able to automatically update AR summary files in NHSN using succession management. Many vendors have implemented this feature by allowing users to simply export a new version of the file but be sure to work with your vendor to determine if this approach is appropriate for you. Please note that succession management does not allow you to delete a record without overwriting it with a new record for that location/month.
There are two options:
- Manually delete and re-upload a new file.
- Use Succession Management within vendor software to replace the existing file.
Manual Deletion:
- Log into NHSN, select ‘Event’ from the navigation menu on the left side and then select Find.
- Use the Event Type drop down menu to select ‘AR – Antimicrobial Resistance’ and optionally input any other identifying information. Select Find.

3. Locate the AR Event you want to delete on the Event List table. Check the box in the Delete column next to the AR Event. Click the ‘Delete’ button at the top of the column to delete the event. You can select additional check boxes if you’d like to delete more than one event.

Succession Management: Your vendor software may be able to automatically update AR Event files in NHSN using succession management. Many vendors have implemented this feature by allowing users to simply export a new version of the file but be sure to work with your vendor to determine if this approach is appropriate for you.
Important Note: Succession management does not allow you to delete a record without overwriting it with a new record for that patient. If you need to simply delete an AR Event that was erroneously submitted, please follow the manual deletion steps above.
Duplicate Rules
Laboratory Testing Results
AR Summary Data
AR Option Analysis
The Antimicrobial Resistance Event Line List report is an organized, detailed list of each record a facility reports into NHSN. You may have to modify the report by filtering by month, pathogen, specimen, or other variable as the default settings may produce a report that is too lengthy to be useful and/or displayed. Users can review the report to verify the data imported successfully and can also be helpful for data validation.
Below is an example AR Event Line List report showing fictitious data and a description of how to read this report:

The Laboratory isolated Stenotrophomonas maltophilia from a patient’s cerebrospinal fluid collected in the MSICU on October 14, 2021. This isolate was resistant to cefiderocol, ceftazidime, chloramphenicol, levofloxacin, and minocycline. The laboratory did not test for sulfamethoxazole with trimethoprim. (Please note that data on this report are fictitious and for example only.)
You can find more information about the AR Event Line List in the Antimicrobial Resistance Event Line List quick reference guide [PDF – 323 KB].
The AR Summary line list is a report summarizing denominator data reported into NHSN for FacWideIN and the individual outpatient locations. For FacWideIN, this includes data on patient days and admissions whereas outpatient encounters are reported for the outpatient locations. By default, this report also includes the “Report No AR Events” variable. Information on how to modify the AR Summary Line List, for example filtering by month or changing the variables displayed, is available in our AR Denominator Line List [PDF – 394 KB] quick reference guide. NHSN has also developed a guide for more information on how to report no AR events [PDF – 394 KB]. Below is an example AR Summary Line List report showing fictitious data and a description of how to read this report:

Please note that data on this report are fictitious and for example only.
This report includes the default variables included in the AR summary line list report. The first line shows that in January 2021 for FacWideIN, there were 5,241 patient days and 264 admissions. The second line shows in July 2021 for EMER, there were 375 patient encounters. The third line shows in July 2021 for FacWideIN, there were 2,350 patient days and 460 admissions reported. In January 2021, the Report No AR Event variable = N, indicating that there are AR Events reported for that calendar month. However, in both rows for July 2021, the Report No AR Event variable = Y, indicating that there were no AR Events to be reported for that calendar month and the facility checked the “Report No Events” boxes for both FacWideIN and EMER.
The facility-wide antibiogram table displays the calculated percent susceptible (%S) for each organism-antimicrobial combination for the time period of interest. Users can modify the antibiogram table to further customize this output. Additional information on the antibiogram is available in the antibiogram quick reference guide [PDF – 1MB].
Below is an example of a facility-wide antibiogram showing fictitious data and a description of how to read it:

Please note that data on this report are fictitious and for example only.
The column headers list the organism category and specific pathogen while the rows represent each antimicrobial test, sorted by drug class. In this example, there were 40 isolates identified as Acinetobacter species. Since there were more than 30 isolates reported, NHSN generates the susceptibility percentages. The first row in that column shows 9% of the Acinetobacter spp. isolates tested were susceptible to amikacin (AMK).
There were only 6 isolates identified as Acinetobacter baumannii or Acinetobacter calcoaceticus-baumannii complex. Because there were less than 30 isolates reported, the susceptibility information is withheld and represented with “.” in the cell. Additionally, specific organism/drug combinations for which there were less than 30 isolates tested will also show as “.”.
Cells shaded in grey represent non-valid organism/drug combinations. When reviewing the antibiogram, keep in mind that some organisms may be grouped with others in their genus (for example, Acinetobacter spp.) and also be separated in a column of their own (Acinetobacter calcoaceticus-baumannii complex). For the full drug name, see the List of Antimicrobial Agents Eligible for AUR Module [XLS – 482 KB] spreadsheet, which is found in the Supporting Materials section of the AUR Module webpage.
Yes, if you customize an antibiogram report and plan to run the same analysis again, you can save your modifications as a template for future use. Once you’ve made your modifications, follow the steps below to save them as a custom report template:
- Click Save on the bottom right-hand side of the modifications screen.
- Change the report name and title on the “Specify a name for your Analysis Report” pop-up screen.
- Click Save to save your modified report as a custom analysis report.

Your report will save to the “Custom Reports” folder under your Antimicrobial Resistance Data folder.
Please note that your modifications will be saved as a template. The custom report will not save the results. Specifically, if new data are uploaded and new data sets are generated, the custom antibiogram output would include the new data (assuming they meet the modification criteria).
To make modifications to your custom report, click the report and select the “Modify Report” option.

NHSN automatically calculates AR Event onset categorization based on the number of hospital days between the date the patient is admitted to the facility and the specimen collection date. Facility admission date is considered Day 1.
- ≤ 3 days = community-onset (CO)
- ≥ 4 days = healthcare facility-onset (HO)
The table and graphic below indicate the onset of an AR Event collected on specific hospital days.
| Specimen collected on hospital day: | AR Event onset: |
|---|---|
| ED encounter | CO |
| Day 1 (admission) | CO |
| Day 2 | CO |
| Day 3 | CO |
| Day 4 | HO |
| Day 5+ | HO |

Please note: any specimen collected in an outpatient location will be categorized as community-onset (CO).