What to know
- There are millions of fungal species, but only a few hundred can make people sick.
- Fungal infections range from mild to life-threatening.
- People with weakened immune systems are at higher risk for most fungal infections.
- Select from the list below to visit their websites and learn about these fungal diseases.
Fungal diseases

The fungus Aspergillus affects lungs in people with weak immunity. Antifungal resistance is growing.

Blastomycosis is a lung infection caused by a fungus that lives in soil in parts of the U.S.

The emerging fungus, C. auris can cause severe multidrug-resistant illness in hospitalized patients.
Candidiasis occurs when Candida, a yeast that lives in parts of the body, grows out of control.
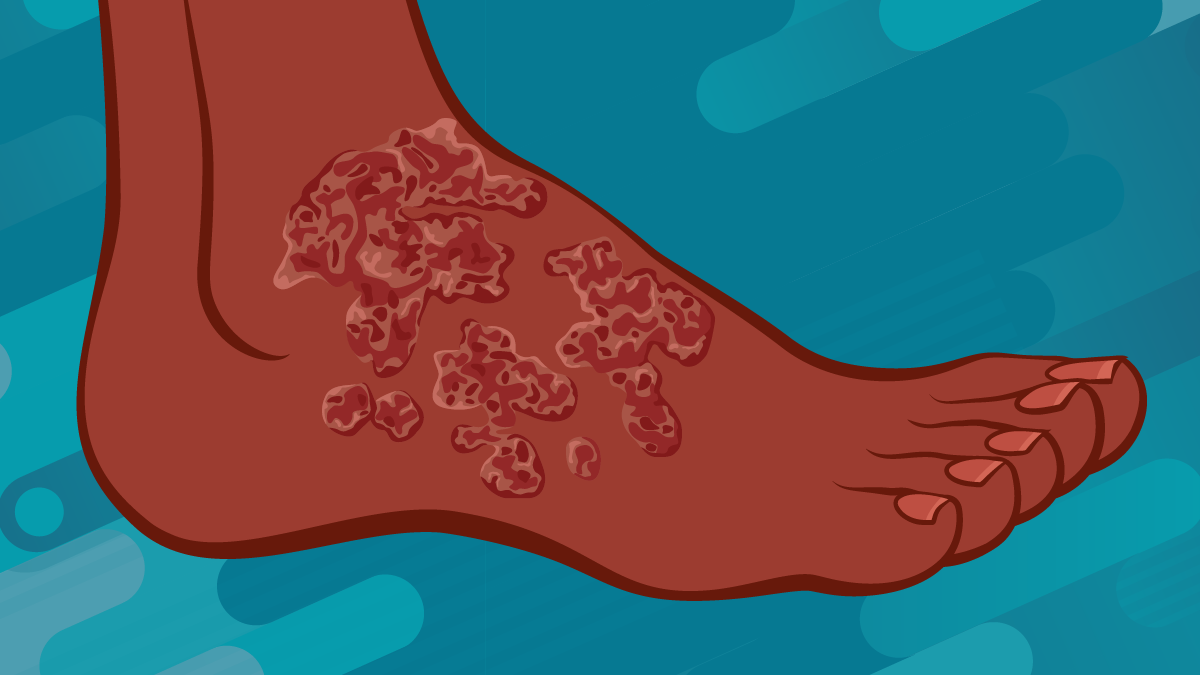
Untreated chromoblastomycosis, a fungal infection, can cause limb swelling and difficulty walking.
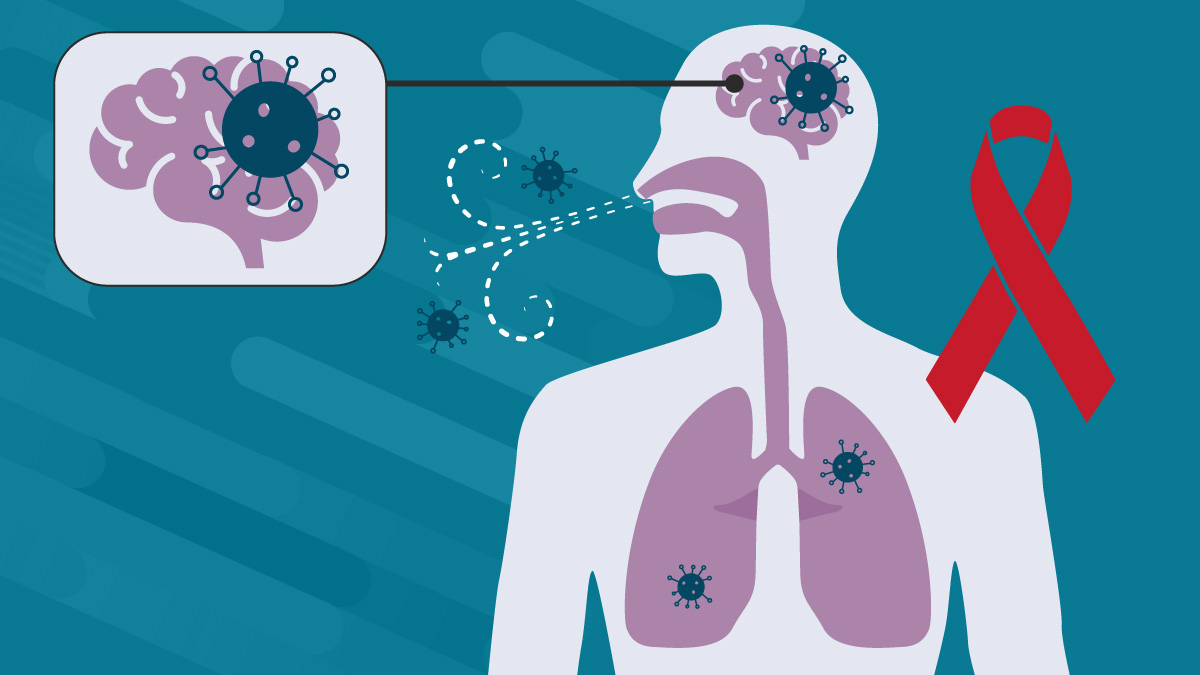
Cryptococcosis usually affects the lungs or brain. People who have HIV/AIDS are at higher risk.
Eye infections caused by fungi are extremely rare, but they can be very serious.

Histoplasma, a fungus in soil, bird, and bat droppings in areas in the U.S., causes lung infections.

Mucormycosis mainly affects the lungs in people with weak immune systems.

Mycetoma is a disease caused by certain types of bacteria and fungi found in soil and water.

Paracoccidioidomycosis is caused by a fungus in Latin America. Many cases are in outdoor workers.

Pneumocystis pneumonia is a serious lung infection that affects people with weakened immune systems.
Ringworm and nail infections are common fungal infections. Ringworm causes a ring-shaped rash.

Sporotrichosis typically causes severe skin infections but can affect other parts of the body.

In Southeast Asia the fungal infection, Talaromycosis can affect people with weak immune systems.

Valley fever (coccidioidomycosis) is a lung infection from a fungus in soil in parts of the U.S.

In the U.S., three types of fungi commonly infect the lungs and can cause pneumonia.

Chromoblastomycosis, mycetoma, paracoccidioidomycosis and sporotrichosis are fungal NTDs.