Intermittent Preventive Treatment of Malaria for Pregnant Women (IPTp)
Why Pregnant Women Are Especially at Risk
Adults who have survived repeated malaria infections throughout their lifetimes may become partially immune to severe or fatal malaria. However, because of the changes in women’s immune systems during pregnancy and the presence of a new organ (the placenta) with new places for parasites to bind, pregnant women lose some of their immunity to malaria infection.
Malaria infection during pregnancy can have adverse effects on both mother and fetus, including maternal anemia, fetal loss, premature delivery, intrauterine growth retardation, and delivery of low birth-weight infants (<2500 g or <5.5 pounds), a risk factor for death.
It is a particular problem for women in their first and second pregnancies and for women who are HIV-positive.
Adverse Effects Vary by Transmission Level
The problems that malaria infection causes differ somewhat by the type of malaria transmission area: stable (high) or unstable (low) transmission.
- In high transmission areas, women have developed immunity that generally prevents severe disease, however, parasite specifically target the placenta, leading in an increased risk during pregnancygained a level of immunity to malaria that wanes somewhat during pregnancy. Malaria infection is more likely to contribute to maternal anemia and delivery of low birth-weight infants (<2500 g or <5.5 pounds). It is a particular problem for women in their first and second pregnancies, for younger women, and for women who are HIV-positive.
- In low transmission areas, women generally have developed no immunity to malaria. Malaria infection is more likely to result in severe malaria disease, maternal anemia, premature delivery, or fetal loss.
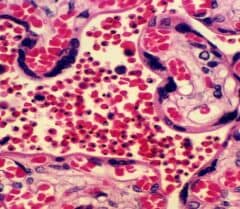
Malaria-infected human placenta examined under the microscope. The intervillous spaces (central area of the picture) are filled with red blood cells, most of which are infected with Plasmodium falciparum malaria parasites. The parasites appear here as black dots. A malaria-infected placenta is unable to carry out normally its main function: to provide nutrients to the fetus.
Recommended Interventions
The currently recommended interventions for pregnant women are
- Use of insecticide-treated bed nets
- Intermittent preventive treatment (IPTp) (for HIV negative women in high transmission areas).
- Effective case management (diagnosis and treatment of illness)
Women should also receive iron/folate supplementation to protect them against anemia, a common occurrence among all pregnant women.
IPTp
IPTp entails administration of a curative dose of an effective antimalarial drug (currently sulfadoxine-pyrimethamine) to all pregnant women without testing whether or not they are infected with the malaria parasite . IPTp should be given at each routine antenatal care visit, starting as early as possible in the second trimester.
Pregnant women are routinely given folic acid supplementation to prevent neural tube defects in their infants. However, high doses of folic acid counteract the effect of sulfadoxine-pyrimethamine. Therefore, it is preferred that women take only the recommended 0.4 mg daily dose of folic acid. In some countries, 5 mg of folic acid are used, and in those countries, it is recommended to withhold folic acid supplementation for two weeks after taking IPTp with sulfadoxine-pyrimethamine to ensure optimal efficacy.

A pregnant woman during an antenatal consultation in Malawi receives sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria (IPTp). The plastic bag on the table holds an insecticide-treated bed net, another method for protecting her against malaria.