Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
General Recommendations on Immunization: Recommendations of the Advisory Committee on Immunization Practices (ACIP)
Please note: An update and an erratum have been published for this report. To view the update, click here. To view the erratum, click here.
The material in this report originated in the National Center for Immunization and Respiratory Diseases, Anne Schuchat, MD, Director.
Corresponding preparer: Andrew Kroger, MD, National Center for Immunization and Respiratory Diseases, 1600 Clifton Rd., MS E-52, Atlanta, GA 30333. Telephone: 404-639-1958; Fax: 404-639-8828; E-mail: aok2@cdc.gov.
Summary
This report is a revision of the General Recommendations on Immunization and updates the 2006 statement by the Advisory Committee on Immunization Practices (ACIP) (CDC. General recommendations on immunization: recommendations of the Advisory Committee on Immunization Practices [ACIP]. MMWR 2006;55[No. RR-15]). The report also includes revised content from previous ACIP recommendations on the following topics: adult vaccination (CDC. Update on adult immunization recommendations of the immunization practices Advisory Committee [ACIP]. MMWR 1991;40[No. RR-12]); the assessment and feedback strategy to increase vaccination rates (CDC. Recommendations of the Advisory Committee on Immunization Practices: programmatic strategies to increase vaccination rates---assessment and feedback of provider-based vaccination coverage information. MMWR 1996;45:219--20); linkage of vaccination services and those of the Supplemental Nutrition Program for Women, Infants, and Children (WIC program) (CDC. Recommendations of the Advisory Committee on Immunization Practices: programmatic strategies to increase vaccination coverage by age 2 years---linkage of vaccination and WIC services. MMWR 1996;45:217--8); adolescent immunization (CDC. Immunization of adolescents: recommendations of the Advisory Committee on Immunization Practices, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American Medical Association. MMWR 1996;45[No. RR-13]); and combination vaccines (CDC. Combination vaccines for childhood immunization: recommendations of the Advisory Committee on Immunization Practices [ACIP], the American Academy of Pediatrics [AAP], and the American Academy of Family Physicians [AAFP]. MMWR 1999;48[No. RR-5]).
Notable revisions to the 2006 recommendations include 1) revisions to the tables of contraindications and precautions to vaccination, as well as a separate table of conditions that are commonly misperceived as contraindications and precautions; 2) reordering of the report content, with vaccine risk-benefit screening, managing adverse reactions, reporting of adverse events, and the vaccine injury compensation program presented immediately after the discussion of contraindications and precautions; 3) stricter criteria for selecting an appropriate storage unit for vaccines; 4) additional guidance for maintaining the cold chain in the event of unavoidable temperature deviations; and 5) updated revisions for vaccination of patients who have received a hematopoietic cell transplant. The most recent ACIP recommendations for each specific vaccine should be consulted for comprehensive details. This report, ACIP recommendations for each vaccine, and additional information about vaccinations are available from CDC at http://www.cdc.gov/vaccines.
Introduction
CDC recommends routine vaccination to prevent 17 vaccine-preventable diseases that occur in infants, children, adolescents, or adults. This report provides information for clinicians and other health-care providers about concerns that commonly arise when vaccinating persons of various ages. Providers and patients encounter numerous issues, such as the timing of each dose, screening for contraindications and precautions, the number of vaccines to be administered, the educational needs of patients and parents, and interpreting and responding to adverse events. Vaccination providers help patients understand the substantial, occasionally conflicting, information about vaccination. These vaccination recommendations are intended for clinicians and other health-care providers who vaccinate patients.
The guidance in this report will help vaccination providers to assess vaccine benefits and risks, use recommended administration and storage practices, understand the most effective strategies for ensuring that vaccination coverage in the population remains high, and communicate the importance of vaccination to reduce the effects of vaccine-preventable disease. These recommendations are intended for use in the United States; vaccine availability, use, and epidemiologic circumstances might differ in other countries and might warrant different recommendations.
Methods
The Advisory Committee on Immunization Practices (ACIP) General Recommendations Work Group (GRWG) revises the General Recommendations on Immunization every 3 to 5 years. Relevant topics are those identified by ACIP as topics that relate to all vaccines, including timing and spacing of doses, vaccine administration, and vaccine storage and handling. New topics often are added when ACIP decides that previous ACIP statements on general issues such as combination vaccines, adolescent vaccination, or adult vaccination should be revised and combined with the General Recommendations on Immunization.
The recommendations in this report are based not only on available scientific evidence but also on expertise that comes directly from a diverse group of health-care providers and public health officials. GRWG includes professionals from academic medicine (pediatrics, family practice, and pharmacy); international (Canada), federal, and state public health professionals; and a member from the nongovernmental Immunization Action Coalition. GRWG, which met monthly beginning June 2007, formed subgroups on the basis of interest in topics such timing and spacing, vaccine administration, and storage and handling. These subgroups also met monthly, conducted literature reviews, and contributed expert opinion on the need for revisions to specific language. In October 2008, GRWG consulted ACIP to determine the best mechanism for approving the resulting document. ACIP concluded that the document could be approved and finalized incrementally, with a final vote on the entire document.
Revisions to the following sections were approved through consensus vote in October 2008 (i.e., were approved as a part of the entire document and not through separate votes on each section): 1) Timing and Spacing of Immunobiologics; 2) Contraindications and Precautions; 3) Preventing and Managing Adverse Reactions; 4) Reporting Vaccine Adverse Events; 5) the National Vaccine Injury Compensation Program; and 6) Vaccine Administration. In February 2009, revisions were made to Storage and Handling of Immunobiologics, and ACIP approved the section. In June 2009, ACIP voted to incorporate the contents of a 1999 ACIP statement on combination vaccines. The statement was revised by GRWG and the ACIP Combination Vaccines Work Group. ACIP also approved minor changes to the section on Special Situations and the section on Vaccination Records. In October 2009, ACIP voted to revise the entire General Recommendations on Immunization, which incorporated ACIP recommendations on adolescent vaccination (1996) and adult vaccination (1991) into the section on Vaccination Programs. Three votes were taken to approve various sections of the document, and one vote was taken to approve the entire document. At this final meeting, ACIP also discussed concerns about the lack of evidence that supports use of antipyretics before or at the time of vaccination for the prevention of fever. Consequently, CDC added information highlighting the lack of evidence for the use of antipyretics to the section on Methods for Alleviating Discomfort and Pain Associated with Vaccination. The last meeting of GRWG was held on December 2, 2009. This meeting served solely to update the work group regarding the discussions and vote of the October 2009 meeting and CDC deliberations on changes to the recommendations on the use of antipyretics.
Timing and Spacing of Immunobiologics
General Principles for Vaccine Scheduling
Optimal response to a vaccine depends on multiple factors, including the type of vaccine, age of the recipient, and immune status of the recipient. Recommendations for the age at which vaccines are administered are influenced by age-specific risks for disease, age-specific risks for complications, age-specific responses to vaccination, and potential interference with the immune response by passively transferred maternal antibodies. Vaccines are recommended for members of the youngest age group at risk for experiencing the disease for which efficacy and safety have been demonstrated.
Certain products, including inactivated vaccines, toxoids, recombinant subunit vaccines, polysaccharide conjugate vaccines, and live vaccines, require ≥2 doses to elicit an adequate antibody response. Tetanus and diphtheria toxoids require booster doses to maintain protective antibody concentrations. Unconjugated polysaccharide vaccines do not induce T-cell memory, and additional doses (although they elicit the same or a lower antibody concentration) might increase the level of protection. Conjugation with a protein carrier improves the effectiveness of polysaccharide vaccines by inducing T-lymphocyte--dependent immunologic function. Many vaccines that stimulate both cell-mediated immunity and neutralizing antibodies (e.g., live, attenuated virus vaccines) usually can induce prolonged immunity, even if antibody titers decline over time (1). Subsequent exposure to such viruses usually results in a rapid anamnestic antibody response without viremia.
Approximately 90%--95% of recipients of a single dose of certain live vaccines administered by injection at the recommended age (i.e., measles, rubella, and yellow fever vaccines) develop protective antibodies, generally within 14 days of the dose. For varicella and mumps vaccines, 80%--85% of vaccinees are protected after a single dose. However, because a limited proportion (5%--15%) of measles, mumps, and rubella (MMR) or varicella vaccinees fail to respond to 1 dose, a second dose is recommended to provide another opportunity to develop immunity (2). Of those who do not respond to the first dose of MMR or varicella vaccine, 97%--99% respond to a second dose (3,4).
The Recommended Immunization Schedules for Persons Aged 0 Through 18 Years and the Recommended Adult Immunization Schedule are revised annually. Physicians and other health-care providers should ensure that they are following the most up-to-date schedules, which are available from CDC at http://www.cdc.gov/vaccines.
Spacing of Multiple Doses of the Same Antigen
Vaccination providers should adhere as closely as possible to recommended vaccination schedules (Table 1). Administration at recommended ages and in accordance with recommended intervals between doses of multidose antigens provide optimal protection.
Administration of doses of a multidose vaccine using intervals that are shorter than recommended might be necessary in certain circumstances, such as impending international travel or when a person is behind schedule on vaccinations but needs rapid protection. In these situations, an accelerated schedule can be implemented using intervals between doses that are shorter than intervals recommended for routine vaccination. The accelerated or minimum intervals and ages for scheduling catch-up vaccinations are available at http://www.cdc.gov/vaccines. Vaccine doses should not be administered at intervals less than these minimum intervals or at an age that is younger than the minimum age.*
Before administering a vaccine dose, providers might need to verify that all previous doses were administered after the minimum age and in accordance with minimum intervals (Table 1). In clinical practice, vaccine doses occasionally are administered at intervals less than the minimum interval or at ages younger than the minimum age. Doses administered too close together or at too young an age can lead to a suboptimal immune response. However, administering a dose a few days earlier the minimum interval or age is unlikely to have a substantially negative effect on the immune response to that dose. Vaccine doses administered ≤4 days before the minimum interval or age are considered valid; however, local or state mandates might supersede this 4-day guideline.† (Day 1 is the day before the day that marks the minimum age or minimum interval for a vaccine.) Because of the unique schedule for rabies vaccine, the 4-day guideline does not apply to this vaccine (5). Doses of any vaccine administered ≥5 days earlier than the minimum interval or age should not be counted as valid doses and should be repeated as age appropriate. The repeat dose should be spaced after the invalid dose by the recommended minimum interval (Table 1). For example, if the first and second doses of Haemophilus influenzae type b (Hib) were administered only 14 days apart, the second dose would be invalid and need to be repeated because the minimum interval from dose 1 to dose 2 is 4 weeks. The repeat dose should be administered ≥4 weeks after the invalid dose (in this case, the second). The repeat dose is counted as the valid second dose.
If the first dose in a series is given ≥5 days before the recommended minimum age, the dose should be repeated on or after the date when the child reaches at least the minimum age. If the vaccine is a live vaccine, ensuring that a minimum interval of 28 days has elapsed from the invalid dose is recommended. For example, if the first dose of varicella vaccine were inadvertently administered at age 10 months, the repeat dose would be administered no earlier than the child's first birthday (the minimum age for the first dose). If the first dose of varicella vaccine were administered at age 11 months and 2 weeks, the repeat dose should be administered no earlier than 4 weeks thereafter, which would occur after the first birthday.
Certain vaccines (e.g., adult tetanus and diphtheria toxoids [Td], pediatric diphtheria and tetanus toxoids [DT]; and tetanus toxoid) produce increased rates of local or systemic reactions in certain recipients when administered more frequently than recommended (6,7). Careful record keeping, maintenance of patient histories, use of immunization information systems (IISs), and adherence to recommended schedules can decrease the incidence of such reactions without adversely affecting immunity.
Simultaneous Administration
Simultaneous administration of vaccines is defined as administering more than one vaccine on the same clinic day, at different anatomic sites, and not combined in the same syringe. Experimental evidence and extensive clinical experience provide the scientific basis for administering vaccines simultaneously. Simultaneously administering all vaccines for which a person is eligible at the time of a visit increases the probability that a child, adolescent, or adult will be vaccinated fully by the appropriate age (8). A study conducted during a measles outbreak demonstrated that approximately one third of measles cases among unvaccinated but vaccine-eligible preschool children might have been prevented if MMR had been administered at the same visit when another vaccine was administered (9). Simultaneous administration also is critical when preparing for foreign travel and when a health-care provider is uncertain that a patient will return for additional doses of vaccine.
With some exceptions, simultaneously administering the most widely used live and inactivated vaccines has produced seroconversion rates and rates for adverse reactions similar to those observed when the vaccines are administered separately (10--13). Routine administration of all age-appropriate doses of vaccines simultaneously is recommended for children for whom no specific contraindications exist at the time of the visit. MMR and varicella vaccine can be administered simultaneously. Live, attenuated influenza vaccine (LAIV) does not interfere with the immune response to MMR or varicella vaccines administered at the same visit. No data exist about the immunogenicity of oral Ty21a typhoid vaccine when administered concurrently or within 30 days of live virus vaccines. In the absence of such data, if typhoid vaccination is warranted, administration should not be delayed because of recent administration of live, attenuated virus vaccines (14). Simultaneous administration of pneumococcal polysaccharide vaccine (PPSV) and inactivated influenza vaccine elicits a satisfactory antibody response without increasing the incidence or severity of adverse reactions (15). Simultaneous administration of PPSV and inactivated influenza vaccine is recommended for all persons for whom both vaccines are indicated. Tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) and trivalent inactivated influenza vaccine (TIV) can be administered simultaneously (16). Hepatitis B vaccine administered with yellow fever vaccine is as safe and immunogenic as when these vaccines are administered separately (17). Measles and yellow fever vaccines have been administered safely at the same visit and without reduction of immunogenicity of either of the components (18,19).
Depending on which vaccines are administered during the first year of life, a child might receive up to nine injections at the 12- through 15-month visit (MMR, varicella, Hib, pneumococcal conjugate vaccine [PCV], pediatric diphtheria and tetanus toxoids and acellular pertussis [DTaP], inactivated poliovirus [IPV], hepatitis A, hepatitis B, and influenza vaccines). Although there is no exact limit on the number of injections, with a little flexibility, a provider can ensure that the primary series doses are given without administering too many injections at each visit. To reduce the number of injections at the 12- through 15-month visit, the hepatitis B series and 3 doses of IPV (20) can be administered before the child's first birthday.
There are many other examples of ways the vaccination schedule provides flexibility. The majority of children aged 1 year who have received 2 Hib vaccine doses (polyribosylribitol phosphate-meningococcal outer membrane protein [PRP-OMP]) or 3 Hib vaccine doses (PRP-tetanus [PRP-T]) and 3 previous doses of DTaP and PCV have protection against Hib, diphtheria, pertussis, tetanus, and pneumococcus, which lasts throughout infancy (21,22). The third (PRP-OMP) or fourth (PRP-T) dose of the Hib series and the fourth doses of DTaP and PCV are critical in boosting antibody titer and ensuring continued protection (22--25). The fourth dose of DTaP is recommended at age 15--18 months but may be administered as early as age 12 months if 6 months have elapsed since the third dose and if there is concern that the child might not return by age 18 months (23). For infants at low risk for infection with hepatitis B virus (i.e., mother tested negative for hepatitis B surface antigen [HBsAg] at the time of delivery and is not in a high risk group), the hepatitis B series can be completed at any time for children aged 6--18 months (26). The minimum age for administration of combination vaccines is the oldest minimum age for any of the individual components; the minimum interval between doses is equal to the greatest minimum interval of any of the individual components. With use of the combination Hib-hepatitis B vaccine, the minimum age of administration of the final dose is 12 months because of the minimum age requirement for the last dose of the Hib series (26). Recommended spacing of doses should be maintained (Table 1).
Combination Vaccines
Combination vaccines merge equivalent component vaccines into single products to prevent more than one disease or to protect against multiple strains of infectious agents causing the same disease. Licensed combination vaccines can be used whenever any components of the combination are indicated and its other components are not contraindicated and if licensed by the Food and Drug Administration (FDA) for that dose in the series. Use of combination vaccines can reduce the number of injections patients receive and alleviate concern associated with the number of injections (20,27,28). Studies have demonstrated that parents and providers might be uncomfortable with multiple injections during single visits (29--31). Potential advantages of combination vaccines include 1) improved vaccine coverage rates (32), 2) timely vaccination coverage for children who are behind the schedule (33,34), 3) reduced shipping and stocking costs, 4) reduced costs for extra health-care visits necessitated by deferral of vaccination, and 5) facilitation of additional new vaccines into vaccination programs.
Potential disadvantages of combination vaccines include the following: 1) adverse events that might occur more frequently after administration of a combination vaccine compared with administration of separate antigens at the same visit, such as those that occur with the combination measles, mumps, rubella, and varicella (MMRV) vaccine and combination DTaP-hepatitis B-IPV vaccine (35,36); 2) confusion and uncertainty about selection of vaccine combinations and schedules for subsequent doses, especially when vaccinations are given by multiple providers who might be using different products; 3) reduced immunogenicity of one or more components (37); 4) extra doses of certain antigens in the fixed product (e.g., a provider who uses DTaP-hepatitis B-IPV vaccine will give an extra dose of hepatitis B component); and 5) a shorter shelf-life than the individual component vaccines. The economic impact of the use of combination vaccines is unclear because combination products have the potential for either increased or decreased costs compared with single-antigen component vaccines. The price of a combination vaccine might exceed the total price of separate vaccines containing the same antigens. However, combination vaccines might represent a better overall economic value if the direct and indirect costs of extra injections, delayed or missed vaccinations, and additional handling and storage are taken into consideration (38).
Licensed Combination Vaccines
In this report, a combination vaccine is defined as a product containing components that can be divided equally into independently available routine vaccines. A dash ( - ) between vaccine products indicates that products are supplied in their final form by the manufacturer and do not require mixing or reconstitution by the user. A slash ( / ) indicates that the products must be mixed or reconstituted by the user. Seven combination vaccines for which separate antigens or antigen combinations exist have been licensed by FDA since 1996 in the United States (Table 2) (39--45). In the future, combination vaccines might include increasing numbers of components in different arrays to protect against these and other diseases. (The status of licensure and recommendations for new vaccines is available at http://aapredbook.aappublications.org/news/vaccstatus.shtml.) The use of a combination vaccine generally is preferred over separate injections of the equivalent component vaccines. Considerations should include provider assessment,§ patient preference, and the potential for adverse events. An exception is the first dose of MMRV. Unless the parent or caregiver expresses a preference for MMRV vaccine, MMR and varicella vaccine should be administered for the first dose for children aged 12--47 months (35).
Situations might arise in which one component of a combination vaccine is specifically preferred to another component in that same vaccine. Future research considerations for newly licensed combination vaccines should focus on safety of doses that are not needed because a patient is already vaccinated against the agents, whether the combination vaccine will improve the timeliness of vaccination, and potential reduced costs from disease prevention resulting from timely vaccination.
Combination Vaccines and FDA Licensure
Only combination vaccines licensed by FDA should be used. Vaccination providers should not combine separate vaccines into the same syringe to administer together unless mixing is indicated for the patient's age and is explicitly specified on the FDA-approved product label inserts. Only two combination vaccines (DTaP-IPV/Hib vaccine, marketed as Pentacel, and DTaP/Hib, marketed as TriHibit) contain separate antigen components for which FDA approves mixing by the user. The safety, immunogenicity, and effectiveness of unlicensed combinations are unknown.
Interchangeability of Formulations
FDA generally licenses a combination vaccine based on studies demonstrating that the product's immunogenicity (or efficacy) and safety are comparable or equivalent to monovalent or combination products licensed previously (46). FDA licensure also generally indicates that a combination vaccine may be used interchangeably with monovalent formulations and other combination products with similar component antigens produced by the same manufacturer to continue the vaccination series. For example, DTaP, DTaP/Hib, and future DTaP vaccines that contain similar acellular pertussis antigens from the same manufacturer may be used interchangeably if licensed and indicated for the patient's age (45).
Interchangeability of Combination Vaccines from Different Manufacturers
Licensure of a vaccine by FDA does not necessarily indicate that the vaccine is interchangeable with products from other manufacturers. Such data are ascertained and interpreted more readily for diseases with known correlates of protective immunity (e.g., specific serologic markers). For diseases without such surrogate laboratory markers, prelicensure field vaccine efficacy (phase III) trials or postlicensure surveillance generally are required to determine protection (47). ACIP prefers that doses of vaccine in a series come from the same manufacturer; however, if this is not possible or if the manufacturer of doses given previously is unknown, providers should administer the vaccine that they have available.
Vaccine Supply
Although vaccination providers should stock sufficient quantities of combination and monovalent vaccines needed to vaccinate children, adolescents, and adults against all diseases for which vaccines are recommended (20,28), all available types or brand-name products need not be stocked. Potential advantages of stocking a limited number of vaccines include 1) reducing confusion and potential errors when staff members must handle redundant products and formulations, 2) minimizing waste when less commonly used products expire, 3) decreasing cold storage capacity requirements, and 4) minimizing administrative costs related to accounting, purchasing, and handling.
Extra Doses of Vaccine Antigens
Administering extra antigens contained in a combination vaccine should be avoided in most situations. Using combination vaccines containing certain antigens not indicated at the time of administration to a patient might be justified when 1) the extra antigen is not contraindicated, 2) products that contain only the needed antigens are not readily available, and 3) potential benefits to the patient outweigh the potential risk for adverse events associated with the extra antigens. An extra dose of many live-virus vaccines and Hib or hepatitis B vaccine has not been found to be harmful (48). However, the risk for an adverse event might increase when extra doses are administered at an earlier time than the recommended interval for certain vaccines (e.g., tetanus toxoid vaccines and PPSV) (16,24,49).
A vaccination provider might not have vaccines available that contain only the antigens needed as indicated by a child's vaccination history. Alternatively, although the indicated vaccines might be available, the provider might prefer to use a combination vaccine to reduce the required number of injections. In such cases, the benefits and risks of administering the combination vaccine with an unneeded antigen should be carefully considered and discussed with the patient or parent.
When inactivated (i.e., killed), or particularly subunit vaccines (which are often adsorbed to aluminum-salt adjuvants), are administered, the reactogenicity of the vaccine must be considered in balancing the benefits and risks of extra doses. Because clinical experience suggests low reactogenicity, an extra dose of Hib or hepatitis B vaccine may be administered as part of a combination vaccine to complete a vaccination series for another component of the combination. Administration of extra doses of tetanus toxoid vaccines earlier than the recommended intervals can increase the risk for hypersensitivity reactions (16,24,50). Examples of such vaccines include DTaP, DTaP/Hib, DT (for children), Td (for adolescents and adults), and Tdap. Extra doses of tetanus-toxoid--containing vaccines might be appropriate for certain patients, including for children who previously received DT or Td vaccine and need protection from pertussis (in DTaP or Tdap) or for immigrants with uncertain vaccination histories.
Conjugate Vaccine Carrier Proteins
Certain carrier proteins in existing conjugated Hib vaccines also are used as components of other vaccines (e.g., pneumococcal and meningococcal vaccines) (51). Protein conjugates used in Hib conjugate vaccines produced in the United States include an outer membrane protein complex from Neisseria meningitidis (in PRP-OMP), and tetanus toxoid (in PRP-T). Simultaneous administration of quadrivalent meningococcal conjugate vaccine (MCV4), PCV, and Tdap, all of which contain diphtheria toxoid, is not associated with reduced immunogenicity or an increase in local adverse events (24,51).
Nonsimultaneous Administration
There is no evidence that inactivated vaccines interfere with the immune response to other inactivated vaccines or to live vaccines. Any inactivated vaccine can be administered either simultaneously or at any time before or after a different inactivated vaccine or live vaccine (Table 3).
Limited data are available regarding interference between live vaccines used in the United States. The immune response to one live-virus vaccine might be impaired if administered within 28 days (i.e., 4 weeks) of another live-virus vaccine (52,53). In a study conducted in two U.S. health maintenance organizations, the risk for varicella vaccine failure (i.e., varicella disease in a vaccinated person) among persons who received varicella vaccine within 28 days of MMR vaccination was threefold higher than among persons who received varicella vaccine >28 days after MMR vaccination (54). Another study determined that the response to yellow fever vaccine is not affected by monovalent measles vaccine administered 1--27 days earlier (18). The effect of nonsimultaneous administration of rubella, mumps, varicella, and yellow fever vaccines is unknown.
To minimize the potential risk for interference, injectable or nasally administered live vaccines not administered on the same day should be administered ≥4 weeks apart (Table 3). If injectable or nasally administered live vaccines are separated by <4 weeks, the second vaccine administered should not be counted as a valid dose and should be repeated. The repeat dose should be administered ≥4 weeks after the last invalid dose. Oral vaccines (Ty21a typhoid vaccine and rotavirus) can be administered simultaneously or at any interval before or after other live vaccines (injectable or intranasal) if indicated.
Spacing of Vaccines and Antibody-Containing Products
Live Vaccines
Ty21a typhoid, yellow fever, LAIV, zoster, and rotavirus vaccines may be administered at any time before, concurrent with, or after administration of any immune globulin, hyperimmune globulin, or intravenous immune globulin (IGIV) (55). Blood (e.g., whole blood, packed red blood cells, and plasma) and other antibody-containing blood products (e.g., immune globulin, hyperimmune globulin, and IGIV) can inhibit the immune response to measles and rubella vaccines for ≥3 months. The effect of blood and immune globulin preparations on the response to mumps and varicella vaccines is unknown; however, commercial immune globulin preparations contain antibodies to these viruses. Blood products available in the United States are unlikely to contain a substantial amount of antibody to yellow fever vaccine virus. The length of time that interference with injectable live-virus vaccine (other than yellow fever) can persist after the antibody-containing product is a function of the amount of antigen-specific antibody contained in the product (56--58). Therefore, after an antibody-containing product is received, live vaccines (other than yellow fever, oral Ty21a typhoid, LAIV, zoster, and rotavirus) should be delayed until the passive antibody has degraded (Table 4). If a dose of injectable live-virus vaccine (other than yellow fever and zoster) is administered after an antibody-containing product but at an interval shorter than recommended in this report, the vaccine dose should be repeated unless serologic testing is feasible and indicates a response to the vaccine. The repeat dose or serologic testing should be performed after the interval indicated for the antibody-containing product (Table 5).
Although passively acquired antibodies can interfere with the response to rubella vaccine, the low dose of anti-Rho(D) globulin administered to postpartum women has not been demonstrated to reduce the response to the RA27/3 strain rubella vaccine (59). Because of the importance of rubella and varicella immunity among women of child-bearing age (4,60), the postpartum vaccination of women without evidence of immunity to rubella or varicella with MMR, varicella, or MMRV vaccines should not be delayed because of receipt of anti-Rho(D) globulin or any other blood product during the last trimester of pregnancy or at delivery. These women should be vaccinated immediately after giving birth and, if possible, tested ≥3 months later to ensure immunity to rubella and, if appropriate, to measles (2).
Interference might occur if administration of an antibody-containing product becomes necessary after administration of MMR or varicella vaccines. Usually, vaccine virus replication and stimulation of immunity occurs 1--2 weeks after vaccination. If the interval between administration of any of these vaccines and subsequent administration of an antibody-containing product is <14 days, vaccination should be repeated after the recommended interval (Tables 4 and 5) unless serologic testing indicates a protective antibody response.
A humanized mouse monoclonal antibody product (palivizumab) is available as prophylaxis for serious lower respiratory tract disease from respiratory syncytial virus among infants and young children. This product contains only antibody to respiratory syncytial virus and does not interfere with the immune response to licensed live or inactivated vaccines.
Inactivated Vaccines
Antibody-containing products interact less with inactivated vaccines, toxoids, recombinant subunit, and polysaccharide vaccines than with live vaccines (61). Therefore, administering inactivated vaccines and toxoids either simultaneously with or at any interval before or after receipt of an antibody-containing product should not substantially impair development of a protective antibody response (Table 4). The vaccine or toxoid and antibody preparation should be administered at different sites using the standard recommended dose. Increasing the vaccine dose volume or number of vaccinations is not indicated or recommended.
Interchangeability of Single-Component Vaccines from Different Manufacturers
Certain vaccines that provide protection from the same diseases are available from different manufacturers, and these vaccines usually are not identical in antigen content or in amount or method of formulation. Manufacturers use different production processes, and their products might contain different concentrations of antigen per dose or a different stabilizer or preservative.
Available data indicate that infants who receive sequential doses of different Hib conjugate, hepatitis B, and hepatitis A vaccines produce a satisfactory antibody response after a complete primary series (62--65). All brands of Hib conjugate, hepatitis B,¶ hepatitis A, rotavirus,** and quadrivalent meningococcal conjugate vaccines are interchangeable within their respective series. If different brands of a particular vaccine require a different number of doses for series completion (e.g., Hib and rotavirus vaccines) and a provider mixes brands, the higher number of doses is recommended for series completion (e.g., 3 doses of either rotavirus or Hib vaccines).
Limited data are available about the safety, immunogenicity, and efficacy of using acellular pertussis (e.g., DTaP) vaccines from different manufacturers for successive doses of the pertussis series. Data from one study indicate that for the first 3 doses of the DTaP series, 1--2 doses of Tripedia (Sanofi Pasteur) followed by Infanrix (GlaxoSmithKline) for the remaining dose (or doses) is comparable to 3 doses of Tripedia with regard to immunogenicity, as measured by antibodies to diphtheria, tetanus, and pertussis toxoids, and filamentous hemagglutinin (66). However, in the absence of a clear serologic correlate of protection for pertussis, the relevance of these immunogenicity data for protection against pertussis is unknown. When feasible, the same brand of DTaP vaccine should be used for all doses of the vaccination series. If vaccination providers do not know or have available the type of DTaP vaccine previously administered to a child, any DTaP vaccine may be used to continue or complete the series. For a child who needs 2 doses of influenza vaccine (TIV or LAIV), it is preferable to use the same type of vaccine for both doses. However, if the child is eligible for either TIV or LAIV, and the type of vaccine used for the first dose is not available, either vaccine can be used for the second dose. For vaccines in general, vaccination should not be deferred because the brand used for previous doses is not available or is unknown (23,67).
Lapsed Vaccination Schedule
Vaccination providers should administer vaccines as close to the recommended intervals as possible. However, intervals between doses that are longer than recommended typically do not reduce final antibody concentrations, although protection might not be attained until the recommended number of doses has been administered. With exception of oral typhoid vaccine, an interruption in the vaccination schedule does not require restarting the entire series of a vaccine or toxoid or addition of extra doses.
Unknown or Uncertain Vaccination Status
Vaccination providers frequently encounter persons who do not have adequate documentation of vaccinations. With the exception of influenza vaccine and PPSV, providers should only accept written, dated records as evidence of vaccination; self-reported doses of influenza vaccine and PPSV are acceptable (49,68). Although vaccinations should not be postponed if records cannot be found, an attempt to locate missing records should be made by contacting previous health-care providers, reviewing state or local IISs, and searching for a personally held record. If records cannot be located within a reasonable time, these persons should be considered susceptible and started on the age-appropriate vaccination schedule. Serologic testing for immunity is an alternative to vaccination for certain antigens (e.g., measles, rubella, hepatitis A, and tetanus). However, commercial serologic testing might not always be sufficiently sensitive or standardized for detection of vaccine-induced immunity (with the exception of hepatitis B vaccination at 1--2 months after the final dose), and research laboratory testing might not be readily available.
Contraindications and Precautions
Contraindications and precautions to vaccination are conditions under which vaccines should not or likely should not be administered. Because the majority of contraindications and precautions are temporary, vaccinations often can be administered later if one or more exist. A contraindication is a condition in a recipient that increases the risk for a serious adverse reaction. A vaccine should not be administered when a contraindication is present; for example, MMR vaccine should not be administered to severely immunocompromised persons. In contrast, certain conditions are commonly misperceived as contraindications (i.e., are not valid reasons to defer vaccination).
National standards for pediatric vaccination practices have been established and include descriptions of valid contraindications and precautions to vaccination. Persons who administer vaccines should screen patients for contraindications and precautions to the vaccine before each dose of vaccine is administered (Table 6). Screening is facilitated by consistent use of screening questionnaires, which are available from certain state vaccination programs and other sources (e.g., the Immunization Action Coalition, http://www.immunize.org).
The only contraindication applicable to all vaccines is a history of a severe allergic reaction (i.e., anaphylaxis) after a previous dose of vaccine or to a vaccine component (unless the recipient has been desensitized; see Special Situations section). In addition, severely immunocompromised persons generally should not receive live vaccines. Children who experienced encephalopathy within 7 days after administration of a previous dose of diphtheria and tetanus toxoids and whole-cell pertussis vaccine (DTP), DTaP, or Tdap not attributable to another identifiable cause should not receive additional doses of a vaccine that contains pertussis. Because of the theoretical risk to the fetus, women known to be pregnant generally should not receive live, attenuated virus vaccines (see Special Situations section).
A precaution is a condition in a recipient that might increase the risk for a serious adverse reaction or that might compromise the ability of the vaccine to produce immunity (e.g., administering measles vaccine to a person with passive immunity to measles from a blood transfusion or administering influenza vaccine to someone with a history of Guillain-Barré syndrome within 6 weeks of a previous influenza vaccination). A person might experience a more severe reaction to the vaccine than would have otherwise been expected; however, the risk for this happening is less than the risk expected with a contraindication. In general, vaccinations should be deferred when a precaution is present. However, a vaccination might be indicated in the presence of a precaution if the benefit of protection from the vaccine outweighs the risk for an adverse reaction. For example a dose of DTaP should be considered for a person in a community with a pertussis outbreak even if that person previously developed Guillain-Barré syndrome after a dose.
The presence of a moderate or severe acute illness with or without a fever is a precaution to administration of all vaccines (Table 6). A personal or family history of seizures is a precaution for MMRV vaccination. A recent study found an increased risk for febrile seizures in children who receive MMRV compared with MMR and varicella vaccine (35).
Clinicians or other health-care providers might misperceive certain conditions or circumstances as valid contraindications or precautions to vaccination when they actually do not preclude vaccination (Table 7). These misperceptions result in missed opportunities to administer recommended vaccines (69). Among the most common conditions mistakenly considered to be contraindications are diarrhea, minor upper respiratory tract illnesses (including otitis media) with or without fever, mild to moderate local reactions to a previous dose of vaccine, current antimicrobial therapy, and being in the convalescent phase of an acute illness.
The decision to administer or delay vaccination because of a current or recent acute illness depends on the severity of symptoms and etiology of the condition. The safety and efficacy of vaccinating persons who have mild illnesses have been documented (70--73). Vaccination should not be delayed because of the presence of mild respiratory tract illness or other acute illness with or without fever. Vaccination should be deferred for persons with a moderate or severe acute illness. This precaution avoids causing diagnostic confusion between manifestations of the underlying illness and possible adverse effects of vaccination or superimposing adverse effects of the vaccine on the underlying illness. After screening them for contraindications, persons with moderate or severe acute illness should be vaccinated as soon as the acute illness has improved. Studies indicate that failure to vaccinate children with minor illnesses can impede vaccination efforts (74--76). Among persons whose compliance with medical care cannot be ensured, use of every opportunity to administer appropriate vaccines is critical.
Routine physical examinations and procedures (e.g., measuring temperatures) are not prerequisites for vaccinating persons who appear to be healthy. The provider should ask the parent or guardian if the child is ill. If the child has a moderate or severe illness, the vaccination should be postponed.
Preventing and Managing Adverse Reactions
Benefit and Risk Communication
Parents, guardians, legal representatives, and adolescent and adult patients should be informed about the benefits of and risks from vaccines in language that is culturally sensitive and at an appropriate educational level. Opportunity for questions should be provided before each vaccination. Discussion of the benefits of and risks from vaccination is sound medical practice and is required by law.
The National Childhood Vaccine Injury Act of 1986†† requires that vaccine information materials be developed for each vaccine covered by the act. These materials, known as vaccine information statements (VISs), must be provided by all public and private vaccination providers each time a vaccine is administered. Copies of VISs are available from state health authorities responsible for vaccination and from CDC (http://www.cdc.gov/vaccines). Translations of VISs into languages other than English are available from certain state vaccination programs and from the Immunization Action Coalition website (http://www.immunize.org). The act does not require that a signature be obtained; however, documentation of consent might be recommended or required by certain state or local health authorities or school authorities.
Certain parents or patients question the need for or safety of vaccinations and want to discuss the risks from and benefits of certain vaccines. Some refuse certain vaccines or reject all vaccinations for personal or religious reasons. Having a basic understanding of how patients and parents of patients view vaccine risk and developing effective approaches to address vaccine safety concerns are imperative for vaccination providers.
Each person understands and reacts to vaccine information on the basis of different factors, including previous experience, education, personal values, method of data presentation, perceptions of the risk for disease and perceived ability to control these risks, and risk preference. Increasingly, decisions about vaccination are based on inaccurate information about risk provided by the media and certain websites. Websites and other sources of vaccine information might be inaccurate or incomplete. Health-care providers can be a pivotal source of science-based credible information by discussing with parents and patients the risks from and benefits of vaccines, which helps patients make informed decisions.
When a parent or patient initiates a discussion about a perceived vaccine adverse reaction, the health-care provider should discuss the specific concerns and provide factual information, using appropriate language. Effective, empathetic vaccine risk communication is essential in responding to misinformation and concerns, with health-care providers recognizing that risk assessment and decision-making can be difficult and confusing. Certain vaccines might be acceptable to a parent who is resistant to other vaccines. This partial acceptance can be used to facilitate additional communication. Their concerns can be addressed using the VIS and offering other resource materials (e.g., vaccination information from CDC: http://www.cdc.gov/vaccines).
The American Academy of Pediatrics (AAP) does not recommend that providers exclude from their practice patients whose parents or guardians question or refuse vaccination. A limited number of providers might exclude patients on this basis; however, an effective public health strategy is to identify common ground and discuss measures that need to be followed if the decision is to defer vaccination. Health-care providers should reinforce key points about each vaccine, including safety, and emphasize risks for disease among unvaccinated children. Parents should be advised of state laws regarding entry to schools or child-care facilities, which might require that unvaccinated children be excluded from the facility during outbreaks. These discussions should be documented in the patient's medical record, including the refusal to receive certain vaccines (i.e., informed refusal).
Preventing Adverse Reactions
Vaccines are intended to produce active immunity to specific antigens. An adverse reaction is an undesirable side effect that occurs after a vaccination. Vaccine adverse reactions are classified as 1) local, 2) systemic, or 3) allergic (additional information available at http://www.fda.gov). Local reactions (e.g., redness) are usually the least severe and most frequent. Systemic reactions (e.g., fever) occur less frequently than local reactions, and severe allergic reactions (e.g., anaphylaxis) are the least frequent reactions. Severe adverse reactions are rare.
Syncope (vasovagal or vasodepressor reaction) can occur after vaccination and is most common among adolescents and young adults. In 2005, the Vaccine Adverse Event Reporting System (VAERS) began detecting a trend of increasing syncope reports that coincided with the licensure of three vaccines for adolescents: human papillomavirus (HPV), MCV4, and Tdap (77). Of particular concern among adolescents has been the risk for serious secondary injuries, including skull fracture and cerebral hemorrhage. Of 463 VAERS reports of syncope during January 1, 2005, to July 31, 2007, a total of 41 listed syncope with secondary injury with information on the timing after vaccination, and the majority of these syncope reports (76%) occurred among adolescents. Among all age groups, 80% of reported syncope episodes occur within 15 minutes of vaccine administration (additional information available at http://www.cdc.gov/vaccinesafety/concern/syncope.htm). Providers should take appropriate measures to prevent injuries if a patient becomes weak or dizzy or loses consciousness. Adolescents and adults should be seated or lying down during vaccination. Vaccine providers, particularly when vaccinating adolescents, should consider observing patients (with patients seated or lying down) for 15 minutes after vaccination to decrease the risk for injury should they faint (77). If syncope develops, patients should be observed until the symptoms resolve.
Managing Acute Vaccine Reactions
Although anaphylactic reactions are rare after vaccination, their immediate onset and life-threatening nature require that all personnel and facilities providing vaccinations have procedures in place for anaphylaxis management. All vaccination providers should be familiar with the office emergency plan and be currently certified in cardiopulmonary resuscitation. Epinephrine and equipment for maintaining an airway should be available for immediate use.
Anaphylaxis usually begins within minutes of vaccine administration (78--80). Rapid recognition and initiation of treatment are required to prevent possible progression to cardiovascular collapse. If flushing, facial edema, urticaria, itching, swelling of the mouth or throat, wheezing, dyspnea, or other signs or symptoms of anaphylaxis occur, the patient should be placed in a recumbent position with the legs elevated if possible (81,82). Administration of epinephrine is the management of choice. Additional drugs also might be indicated (Table 8) (83). Maintenance of the airway and oxygen administration might be necessary. After the patient is stabilized, arrangements should be made for immediate transfer to an emergency facility for additional evaluation and treatment.
Reporting Adverse Events After Vaccination
Modern vaccines are safe and effective; however, adverse events have been reported after administration of all vaccines (84). More complete information about adverse reactions to a specific vaccine is available in the package insert for each vaccine and from CDC at http://www.cdc.gov/vaccines/vac-gen/side-effects.htm. An adverse event is an untoward event that occurs after a vaccination that might be caused by the vaccine product or vaccination process. These events range from common, minor, local reactions to rare, severe, allergic reactions (e.g., anaphylaxis). Establishing evidence for cause and effect on the basis of case reports and case series alone is usually not possible because health problems that have a temporal association with vaccination do not necessarily indicate causality.
Many adverse events require more detailed epidemiologic studies to compare the incidence of the event among vaccinees to the incidence among unvaccinated persons. Reporting adverse events, including serious events, to VAERS is a key mechanism for identifying potential vaccine safety concerns. Potential causal associations between reported adverse events after vaccination can be assessed through epidemiologic or clinical studies.
The National Childhood Vaccine Injury Act requires health-care providers and vaccine manufacturers to report to VAERS specific adverse events that occur after vaccination. The reporting requirements are different for manufacturers and health-care providers. Manufacturers are required to report all adverse events that occur after vaccination to VAERS, whereas health-care providers are required to report events that appear in the reportable events table on the VAERS website at http://vaers.hhs.gov/reportable.htm.
In addition to the mandated reporting of events listed on the reportable events table, health-care providers should report to VAERS all events listed in product inserts as contraindications, as well as all clinically significant adverse events, even if they are uncertain that the adverse event is related causally to vaccination. Persons other than health-care providers also can report adverse events to VAERS.
There are three ways to report to VAERS:
- Submit the report online via a secure website at https://vaers.hhs.gov/esub/step1,
- Fax a completed VAERS form to 877-721-0366, or
- Mail a completed VAERS form: VAERS, P.O. Box 1100, Rockville, MD 20849-1100.
A VAERS form can be downloaded from the VAERS website at http://vaers.hhs.gov/resources/vaers_form.pdf. VAERS forms also can be requested by e-mail (info@vaers.org), telephone (800-822-7967), or fax (877-721-0366).
National Vaccine Injury Compensation Program
The National Vaccine Injury Compensation Program, established by the National Childhood Vaccine Injury Act of 1986, is a no-fault system in which persons thought to have experienced an injury or to have died as a result of administration of a covered vaccine can seek compensation. The program became operational on October 1, 1988, and is intended as an alternative to civil litigation under the traditional tort system in that negligence need not be proven. Claims arising from covered vaccines must first be adjudicated through the program before civil litigation can be pursued.
The program relies on the Vaccine Injury Table, which lists the vaccines covered by the program and the injuries (including death), disabilities, illnesses, and conditions for which compensation might be awarded. The table defines the time during which the first symptom or substantial aggravation of an injury must appear after vaccination to be eligible. Successful claimants receive a legal presumption of causation if a condition listed in the table is proven, thus avoiding the need to prove actual causation in an individual case. Claimants also can prevail for conditions not listed in the reportable events table if they prove causation for covered vaccines. Additional information is available from the Health Resources and Services Administration (HRSA) (http://www.hrsa.gov/vaccinecompensation, telephone: 800-338-2382). Persons who would like to file a claim for vaccine injury should contact the U.S. Court of Federal Claims (717 Madison Place, N.W., Washington, DC 20005; telephone: 202-357-6400).
Vaccine Administration
Infection Control and Sterile Technique
General Precautions
Persons administering vaccinations should follow appropriate precautions to minimize risk for spread of disease. Hands should be cleansed with an alcohol-based waterless antiseptic hand rub or washed with soap and water before preparing the vaccine and between each patient contact (85). Occupational Safety and Health Administration (OSHA) regulations do not require gloves to be worn when administering vaccinations, unless persons administering vaccinations are likely to come into contact with potentially infectious body fluids or have open lesions on their hands. If gloves are worn, they should be changed between patients.
Needles and Syringes
Needles and syringes used for vaccine injections must be sterile and disposable. A separate needle and syringe should be used for each injection. Changing needles between drawing vaccine from a vial and injecting it into a recipient is not necessary unless the needle has been damaged or contaminated. Different vaccines should never be mixed in the same syringe unless specifically licensed for such use, and no attempt should be made to transfer between syringes. Single-dose vials and manufacturer-filled syringes are designed for single-dose administration and should be discarded if vaccine has been withdrawn or reconstituted and subsequently not used within the time frame specified by the manufacturer. This typically is no longer than the same clinic day (typically recommended as a maximum for inactivated vaccines).
Sometimes providers prefill syringes themselves. ACIP discourages the routine practice of prefilling syringes because of the potential for administration errors and vaccine wastage. Because the majority of vaccines have a similar appearance after being drawn into a syringe, prefilling might result in administration errors. In certain circumstances in which a single vaccine type is being used (e.g., in preparation for a community influenza vaccination campaign), filling a small number of syringes may be considered. Vaccine doses should not be drawn into a syringe until immediately before administration. When syringes are filled, the type of vaccine, lot number, and date of filling must be labeled on each syringe, and the doses should be administered as soon as possible after filling. Unused syringes filled by the end user (i.e., not filled by the manufacturer) should be discarded at the end of the vaccination session. In addition to administration errors, prefilling of syringes is a concern because FDA does not license administration syringes for vaccine storage. Unused syringes that are prefilled by the manufacturer and activated (i.e., syringe cap removed or needle attached) should be discarded at the end of the clinic day. When in doubt about the appropriate handling of a vaccine, vaccination providers should contact the manufacturer.
Bloodborne diseases (e.g., hepatitis B, hepatitis C, and human immunodeficiency virus [HIV]) are occupational hazards for clinicians and other health-care providers. The Needlestick Safety and Prevention Act was enacted in 2000 to reduce the incidence of needle-stick injury and the consequent risk for bloodborne diseases acquired from patients. The act directed OSHA to strengthen its existing bloodborne pathogen standards. The revised standards became effective in 2001 (86). These federal regulations require that safety-engineered injection devices (e.g., needle-shielding syringes or needle-free injectors) be used for injectable vaccination in all clinical settings. The regulations also require maintenance of records documenting injuries caused by needles and other medical sharp objects and that nonmanagerial employees be involved in the evaluation and selection of safety-engineered devices before they are procured.
Safety-engineered needles and syringes or needle-free injection devices are preferred and should be encouraged to reduce risk for injury. To prevent inadvertent needle-stick injury or reuse, safety mechanisms should be deployed after use and needles and syringes should be discarded immediately in labeled, puncture-proof containers located in the same room where the vaccine is administered. Used needles should never be recapped.
Needle-shielding or needle-free devices that might satisfy the occupational safety regulations for administering injectable vaccines are available in the United States (87--89). Additional information about implementation and enforcement of these regulations is available from OSHA (http://www.osha.gov).
Route of Administration
Oral Route
Rotavirus and oral typhoid vaccines are the only vaccines administered orally in the United States. Oral typhoid capsules should be administered as directed by the manufacturer. The capsules should not be opened or mixed with any other substance. Rotavirus vaccines are licensed for infants. There are two brands of rotavirus vaccine, and they have different types of applicators. Providers should consult the package insert for details. A dose of rotavirus vaccine need not be repeated if the vaccine is spit up or vomited. The infant should receive the remaining recommended doses of rotavirus vaccine following the routine schedule.
Intranasal Route
LAIV is licensed for healthy nonpregnant persons aged 2--49 years and is the only vaccine administered by the intranasal route. The administration device is a nasal sprayer with a dose-divider clip that allows introduction of one 0.1-mL spray into each naris. The tip should be inserted slightly into the naris before administration. Even if the person coughs or sneezes immediately after administration or the dose is expelled any other way, the vaccine dose need not be repeated. Introduction of low levels of vaccine viruses into the environment likely is unavoidable when administering LAIV; however, no instances have been reported of illness or attenuated vaccine virus infections among inadvertently exposed health-care providers or immunocompromised patients. The risk for acquiring vaccine viruses from the environment is unknown but is likely low; in addition, vaccine viruses are cold-adapted and attenuated and unlikely to cause symptomatic influenza. Severely immunosuppressed persons should not administer LAIV. However, other persons at higher risk for influenza complications can administer LAIV. These include persons with underlying medical conditions placing them at higher risk or who are likely to be at risk, including pregnant women, persons with asthma, and persons aged ≥50 years (68).
Injectable Route
With the exception of bacille Calmette-Guérin (BCG) vaccine and smallpox vaccine, injectable vaccines are administered by the intramuscular or subcutaneous route. The method of administration of injectable vaccines is determined, in part, by the presence of adjuvants in some vaccines. An adjuvant is a vaccine component distinct from the antigen that enhances the immune response to the antigen. Inactivated vaccines containing an adjuvant should be injected into a muscle because administration subcutaneously or intradermally can cause local irritation, induration, skin discoloration, inflammation, and granuloma formation. Routes of administration are recommended by the manufacturer for each immunobiologic (Table 9). Deviation from the recommended route of administration might reduce vaccine efficacy (90,91) or increase the risk for local adverse reactions (92--94).
Intramuscular Injections
Needle Length
Injectable immunobiologics should be administered where local, neural, vascular, or tissue injury is unlikely. Use of longer needles has been associated with less redness or swelling than occurs with shorter needles because of injection into deeper muscle mass (92). Appropriate needle length depends on age and body mass. Injection technique is the most important parameter to ensure efficient intramuscular vaccine delivery.
For all intramuscular injections, the needle should be long enough to reach the muscle mass and prevent vaccine from seeping into subcutaneous tissue, but not so long as to involve underlying nerves, blood vessels, or bone (91,95--97). Vaccinators should be familiar with the anatomy of the area into which they are injecting vaccine. Intramuscular injections are administered at a 90-degree angle to the skin, preferably into the anterolateral aspect of the thigh or the deltoid muscle of the upper arm, depending on the age of the patient (Table 10).
A decision on needle size and site of injection must be made for each person on the basis of the size of the muscle, the thickness of adipose tissue at the injection site, the volume of the material to be administered, injection technique, and the depth below the muscle surface into which the material is to be injected (Figure 1). Aspiration before injection of vaccines or toxoids (i.e., pulling back on the syringe plunger after needle insertion but before injection) is not necessary because no large blood vessels are present at the recommended injection sites, and a process that includes aspiration might be more painful for infants (98).
Infants (Aged <12 Months)
For the majority of infants, the anterolateral aspect of the thigh is the recommended site for injection because it provides a large muscle mass (Figure 2). In certain circumstances (e.g., physical obstruction to other sites and no reasonable indication to defer doses), the gluteal muscle can be used. If the gluteal muscle must be used, care should be taken to define the anatomic landmarks.§§ Injection technique is the most important parameter to ensure efficient intramuscular vaccine delivery. If the subcutaneous and muscle tissue are bunched to minimize the chance of striking bone (95), a 1-inch needle is required to ensure intramuscular administration in infants aged ≥1 month. For the majority of infants, a 1-inch, 22- to 25-gauge needle is sufficient to penetrate the thigh muscle. For neonates (first 28 days of life) and preterm infants, a ⅝-inch needle usually is adequate if the skin is stretched flat between the thumb and forefinger and the needle is inserted at a 90-degree angle to the skin (97).
Toddlers (Aged 12 Months--2 Years)
For toddlers, the anterolateral thigh muscle is preferred, and if used, the needle should be at least 1 inch long. The deltoid muscle can be used if the muscle mass is adequate. A ⅝-inch needle is adequate only for the deltoid muscle and only if the skin is stretched flat between thumb and forefinger and the needle is inserted at a 90-degree angle to the skin.
Children (Aged 3--18 Years)
The deltoid muscle is preferred for children aged 3--18 years (Figure 3); the needle size for deltoid site injections can range from 22 to 25 gauge and from ⅝ to 1 inch on the basis of technique. Knowledge of body mass can be useful for estimating the appropriate needle length (99); however, neither a physical examination nor measurement of body mass is necessary to administer vaccines. Most children in this age range require a ⅝- or 1-inch needle (or intermediate size, if available).
Adults (Aged ≥19 Years)
For adults, the deltoid muscle is recommended for routine intramuscular vaccinations. The anterolateral thigh also can be used. For men and women who weigh <130 lbs (<60 kg), a ⅝-inch needle is sufficient to ensure intramuscular injection in the deltoid muscle if the injection is made at a 90-degree angle and the tissue is not bunched. For men and women who weigh 130--152 lbs (60--70 kg), a 1-inch needle is sufficient. For women who weigh 152--200 lbs (70--90 kg) and men who weigh 152--260 lbs (70--118 kg), a 1- to 11/2 -inch needle is recommended. For women who weigh >200 lbs (>90 kg) or men who weigh >260 lbs (>118 kg), a 11/2-inch needle is recommended (Table 10) (96).
Subcutaneous Injections
Subcutaneous injections are administered at a 45-degree angle, usually into the thigh for infants aged <12 months and in the upper-outer triceps area of persons aged ≥12 months. Subcutaneous injections may be administered into the upper-outer triceps area of an infant if necessary. A ⅝-inch, 23- to 25-gauge needle should be inserted into the subcutaneous tissue (Figures 4 and 5).
Multiple Injections
If multiple vaccines are administered at a single visit, administer each preparation at a different anatomic site. For infants and younger children, if more than two vaccines are injected in a single limb, the thigh is the preferred site because of the greater muscle mass; the injections should be sufficiently separated (i.e., ≥1 inch if possible) so that any local reactions can be differentiated (92,100). For older children and adults, the deltoid muscle can be used for more than one intramuscular injection. If a vaccine and an immune globulin preparation are administered simultaneously (e.g., Td/Tdap and tetanus immune globulin [TIG], hepatitis B and hepatitis B immunoglobulin [HBIG]), separate anatomic sites (i.e., different limbs) should be used for each injection. The location of all injection sites should be documented in the patient's medical record. Health-care practices should consider using a vaccination site map so that all persons administering vaccines routinely use a particular anatomic site for each different vaccine.
Jet Injections
Jet injectors are needle-free devices that pressurize liquid medication, forcing it through a nozzle orifice into a narrow stream capable of penetrating skin to deliver a drug or vaccine into intradermal, subcutaneous, or intramuscular tissues (101,102). Jet injectors prevent needle-stick injuries to health-care providers (86) and can overcome improper, unsterile reuse and other drawbacks of needles and syringes in developing countries (87,103--104). Immune responses generated by jet injectors against both attenuated and inactivated viral and bacterial antigens are usually equivalent to, and occasionally greater than, immune responses induced by needle injection. However, local reactions or injuries are sometimes more frequent on delivery of vaccine by jet injectors compared with needle injection, depending on the inherent irritability of the vaccine and operator technique (102). Jet injectors that use the same nozzle for consecutive injections without intervening sterilization were used in mass vaccination campaigns from the 1950s through the 1990s (102); however, these were found to be unsafe because of the possibility of bloodborne pathogen transmission (105--108) and should not be used. A new generation of jet injectors with disposable cartridges and syringes has been developed since the 1990s. With a new, sterile dose chamber and nozzle for each patient and correct use, these devices do not have the same safety concerns as multiple-use nozzle jet injectors. Several of the newer devices have been approved by FDA for sale in the United States (102).
Methods for Alleviating Discomfort and Pain Associated with Vaccination
Comfort measures, such as distraction (e.g., playing music or pretending to blow away the pain), ingestion of sweet liquids, breastfeeding, cooling of the injection site, and topical analgesia, can help infants or children cope with the discomfort associated with vaccination (109,110). Pretreatment (30--60 minutes before injection) with a 5% topical lidocaine-prilocaine emulsion might decrease the pain of vaccination by causing superficial anesthesia (111,112). Evidence indicates that this cream does not interfere with the immune response to MMR (113). Topical lidocaine-prilocaine emulsion should not be used on infants aged <12 months who are receiving treatment with methemoglobin-inducing agents because of the possible development of methemoglobinemia (114). Use of a topical refrigerant (vapocoolant) spray immediately before vaccination can reduce the short-term pain associated with injections and can be as effective as lidocaine-prilocaine cream (115). Evidence does not support use of antipyretics before or at the time of vaccination; however, they can be used for the treatment of fever and local discomfort that might occur following vaccination. Studies of children with previous febrile seizures have not demonstrated antipyretics to be effective in the prevention of febrile seizures (116).
Nonstandard Vaccination Practices
Recommendations for route, site, and dosage of immunobiologics are derived from data from clinical trials, practical experience, normal periodicity of health-care visits, and theoretical considerations. ACIP discourages variations from the recommended route, site, volume, or number of doses of any vaccine.
Variation from the recommended route and site can result in inadequate protection. In adults (but not in infants) (117), the immunogenicity of hepatitis B is substantially lower when the gluteal rather than the deltoid site is used for administration (90). Hepatitis B administered intradermally might result in a lower seroconversion rate and final titer of hepatitis B surface antibody than when administered by the deltoid intramuscular route (118,119). Hepatitis B administered by any route other than intramuscular, or in adults at any site other than the deltoid or anterolateral thigh, should not be counted as valid and should be repeated. Similarly, doses of rabies vaccine administered in the gluteal site should not be counted as valid doses and should be repeated (120). MCV4 should be administered intramuscularly; however, revaccination is not necessary if a vaccine dose is administered subcutaneously (121). Inactivated influenza vaccine is immunogenic when administered in a lower than standard dose by the intradermal route to healthy adult volunteers (122). However, the immunogenicity for persons aged ≥60 years is inadequate, and varying the recommended route and dose is not recommended.
Live, attenuated injectable vaccines (e.g., MMR, varicella, and yellow fever) and certain inactivated vaccines (e.g., meningococcal polysaccharide) are recommended by the manufacturers to be administered by subcutaneous injection. PPSV and IPV are recommended by the manufacturer to be administered by the subcutaneous or intramuscular route. Response to vaccines recommended by the subcutaneous route are unlikely to be affected if the vaccines are administered by the intramuscular rather than subcutaneous route. Repeating doses of vaccine administered by the intramuscular route when recommended to be by the subcutaneous route is not necessary.
Administering volumes smaller than recommended (e.g., inappropriately divided doses) might result in inadequate protection. Using reduced doses administered at multiple vaccination visits that equal a full dose or using smaller divided doses is not recommended. Any vaccination using less than the standard dose should not be counted, and the person should be revaccinated according to age unless serologic testing indicates that an adequate response has developed. If less than a full recommended dose of a parenteral vaccine is administered because of syringe or needle leakage, the dose should be repeated. Using larger than recommended dosages can be hazardous because of excessive local or systemic concentrations of antigens or other vaccine constituents.
Storage and Handling of Immunobiologics
Failure to adhere to recommended specifications for storage and handling of immunobiologics can reduce or destroy their potency, resulting in inadequate or no immune response in the recipient. Recommendations in the product package inserts, including methods for reconstitution of the vaccine, should be followed carefully. Maintenance of vaccine quality is the shared responsibility of all handlers of vaccines from the time a vaccine is manufactured until administration. All vaccines should be inspected on delivery and monitored during storage to ensure that the recommended storage temperatures are maintained. Vaccines should continue to be stored at recommended temperatures immediately on receipt until use. Inadequate vaccine storage also can result in the loss of thousands of dollars worth of vaccine inventory and the cost of inventory replacement.
Storage Temperature
Vaccines licensed for refrigerator storage should be stored at 35°F--46°F (2°C--8°C). Liquid vaccines containing an aluminum adjuvant permanently lose potency when exposed to freezing temperatures. Live, attenuated virus vaccines that should be frozen lose potency when exposed to higher temperatures because the viruses degrade more quickly at storage temperatures that are warmer than recommended (Table 11).
Storage Units
Refrigerators and freezers used for vaccine storage must maintain the required temperature range year-round, be large enough to hold the year's largest inventory, and be dedicated to storage of vaccines. Vaccine storage units must be carefully selected, used properly, and consistently monitored to ensure that recommended temperatures are maintained. Refrigerators without freezers and stand-alone freezers (either manual defrost or automatic defrost) are usually the most effective at maintaining the precise temperatures required for vaccine storage. Such single-purpose units sold for home use are less expensive alternatives to medical specialty equipment (123) and are preferable to combination units. A combination refrigerator-freezer unit sold for home use might be adequate for storing limited quantities of vaccines if the refrigerator and freezer compartments have separate external doors. Before using the refrigerator for vaccine storage, the temperature should be allowed to stabilize and then be measured in various locations within the refrigerator compartment to document that a consistent temperature can be maintained within the compartment (Table 11) (124). New units might need ≥2 days of operation to establish a stable operating temperature; vaccine should not be stored in the unit until the unit maintains an appropriate and stable storage temperature. Refrigerator temperatures are most reflective of the actual compartment temperature after the door has remained closed and undisturbed for several hours (e.g., overnight). The refrigerator temperature should be set at the midpoint of the recommended range (i.e., 40°F [5°C]) (125,126). A storage unit should be sufficiently sized so that vaccines can be placed away from the walls in the part of the unit best able to maintain the constant, required temperature. Combination units, with separate compartments of smaller size, can only be used to store limited quantities of vaccines. Frequent opening and closing of doors can cause fluctuations in compartment temperature; food, beverages, and clinical specimens should not be stored in vaccine storage units. If it becomes necessary to store clinical specimens in the same unit as vaccines, the clinical specimens should be on a shelf below the vaccine to prevent contamination should the specimen leak.
Temperature Monitoring
Temperature monitoring is a critical component of temperature management. All office and clinical staff members should be aware of vaccine vulnerabilities and storage requirements. Assigning one person in the office the primary responsibility for maintaining and reviewing temperature logs (Figure 6) generally is most effective, with a second person assigned as backup. Temperatures for both the refrigerator and freezer should be documented twice a day and recorded. The backup person should review the log at least once each week. Temperature logs should be maintained for 3 years unless state or local authorities require a longer time. An automated monitoring system that alerts staff when a temperature deviation occurs is optimal. However, even if an automated monitoring system is used, temperatures still should be manually checked and recorded twice each day.
Thermometers should be placed in each compartment near the vaccines. Different types of thermometers can be used, including standard fluid-filled, minimum-maximum, and continuous chart recorder thermometers (Table 12). Standard fluid-filled thermometers are the simplest and least expensive products. Product temperature thermometers are encased in biosafe liquids and generally reflect refrigerator temperature more accurately than standard fluid-filled thermometers. Minimum-maximum thermometers monitor the temperature range. Continuous chart recorder thermometers monitor temperature range and duration. All thermometers used for monitoring vaccine storage temperatures should be calibrated and certified by an appropriate agency (e.g., National Institute of Standards and Technology or the American Society for Testing and Materials). Because all thermometers are calibrated as part of the manufacturing process, this recommendation refers to a second calibration process that occurs after manufacturing but before marketing and is documented with a certificate that comes with the product. Some products (e.g., continuous chart recorder thermometers) usually include a manufacturer-defined schedule for additional recalibration. For many types of thermometers, replacement might be less expensive than recalibration. Thermometers that require batteries need to have the batteries changed; review the documentation that comes with the product for guidance.
Response to Out-of-Range Temperature Reading
An out-of-range temperature reading should prompt immediate action. A plan should be developed ahead of time to address various types of emergencies that might require removal of vaccine from the original storage unit. Transfer of vaccines to a predesignated alternative emergency storage site might be necessary if a temperature problem cannot be resolved immediately (e.g., plugging in an unplugged unit or closing a door that has been left open). Vaccine should be marked "do not use" and moved to the alternate site after verifying that the alternate unit is at the proper temperature. After the vaccine has been moved, determine whether the vaccine is still useable by contacting the state or local health department or manufacturer. Damage to the immunogenicity of a vaccine exposed to temperatures outside of the recommended range might not be apparent visually. As a general rule, vaccines that have been stored at inappropriate temperatures should not be administered. If such vaccines already have been administered, guidance is available from the state health department or CDC. Vaccine exposed to inappropriate temperatures that is inadvertently administered should generally be repeated. Clinicians should consult with state or local health departments in these situations.
Expiration Dates and Windows
All vaccines have an expiration date determined by the manufacturer that must be observed. Providers should record the vaccine expiration dates and lot numbers on a stock or inventory record for each vaccine vial when a shipment is received. When vaccines are removed from storage, clinicians and other health-care providers should note whether an expiration window exists for vaccine stored at room temperature or at an intermediate temperature. For example, single-component varicella vaccine that is stored frozen must be discarded after 72 hours of storage at refrigerator temperature. Vaccine transport between the storage site and the administration clinic is discouraged unless the cold chain is maintained, and vaccine transport by the patient (e.g., transporting zoster vaccine from a pharmacy to a clinic) is particularly discouraged. An expiration window also applies to vaccines that have been reconstituted. For example, after reconstitution, MMR vaccine should be kept at refrigerator temperature and must be administered within 8 hours. Doses of expired vaccines that are administered inadvertently generally should not be counted as valid and should be repeated. Inactivated vaccines should be repeated as soon as possible. Live vaccines should be repeated after a 28-day interval from the invalid dose to reduce the risk for interference from interferon on the subsequent doses. Additional information about expiration dates is available at http://www.cdc.gov/vaccines/recs/storage.
Multidose Vials
Certain vaccines (i.e., quadrivalent meningococcal polysaccharide vaccine [MPSV4], PPSV, TIV, IPV, and yellow fever) are available in multidose vials. Because several doses are withdrawn from the same vial, proper technique must be followed to prevent contamination. For multidose vials that do not require reconstitution, doses that remain after withdrawal of a dose can be administered until the expiration date printed on the vial or vaccine packaging if the vial has been stored correctly and the vaccine is not visibly contaminated, unless otherwise specified by the manufacturer. Multidose vials that require reconstitution must be used within the interval specified by the manufacturer. After reconstitution, the new expiration date should be written on the vial.
Altered Immunocompetence
General Principles
Altered immunocompetence, a term often used synonymously with immunosuppression and immunocompromise, can be classified as primary or secondary. Primary immunodeficiencies generally are inherited and include conditions defined by an absence or quantitative deficiency of cellular or humoral components or both that provide immunity. Examples include congenital immunodeficiency diseases such as X-linked agammaglobulinemia, severe combined immunodeficiency disease, and chronic granulomatous disease. Secondary immunodeficiency generally is acquired and is defined by loss or qualitative deficiency in cellular or humoral immune components that occurs as a result of a disease process or its therapy. Examples of secondary immunodeficiency include HIV infection, hematopoietic malignancies, treatment with radiation, and treatment with immunosuppressive drugs including alkylating agents and antimetabolites. The degree to which immunosuppressive drugs cause clinically significant immunodeficiency generally is dose related and varies by drug. Primary and secondary immunodeficiencies might include a combination of deficits in both cellular and humoral immunity. In this report, the general term altered immunocompetence also is used to include conditions such as asplenia and chronic renal disease, and treatments with therapeutic monoclonal antibodies (specifically, the tumor necrosis factor inhibitors) (127--132) and prolonged administration of high-dose corticosteroids.
Determination of altered immunocompetence is important to the vaccine provider because incidence or severity of some vaccine-preventable diseases is higher in persons with altered immunocompetence; therefore, certain vaccines (e.g., inactivated influenza vaccine and pneumococcal vaccines) are recommended specifically for persons with these diseases (28,68). Vaccines might be less effective during the period of altered immunocompetence. Live vaccines might need to be deferred until immune function has improved. Inactivated vaccines administered during the period of altered immunocompetence might need to be repeated after immune function has improved. In addition, persons with altered immunocompetence might be at increased risk for an adverse reaction after administration of live, attenuated vaccines because of uninhibited replication.
The degree of altered immunocompetence in a patient should be determined by a physician. The challenge for clinicians and other health-care providers is assessing the safety and effectiveness of vaccines for conditions associated with primary or secondary immunodeficiency, especially when new therapeutic modalities are being used and information about the safety and effectiveness of vaccines has not been characterized fully in persons receiving these drugs (Table 13). Laboratory studies can be useful for assessing the effects of a disease or drug on the immune system. Tests useful to assess humoral immunity include immunoglobulin (and immunoglobulin subset) levels and specific antibody levels (e.g., tetanus and diphtheria). Tests that demonstrate the status of cellular immunity include lymphocyte numbers (i.e., a complete blood count with differential), a test that delineates concentrations and proportions of lymphocyte subsets (i.e., B and T lymphocytes, CD4+ T versus CD8+ T lymphocytes), and tests that measure T-cell proliferation in response to specific or nonspecific stimuli (e.g., lymphocyte proliferation assays) (133,134). The ability to characterize a drug or disease condition as affecting cellular or humoral immunity is only the first step; using this information to draw inferences about whether particular vaccines are indicated or whether caution is advised with use of live or inactivated vaccines is more complicated and might require consultation with an infectious disease or immunology specialist.
Altered Immunocompetence as an Indication to Receive a Vaccine
Persons with altered immunocompetence generally are advised to receive TIV and age-appropriate polysaccharide-based vaccines (PCV, PPSV, MCV4, MPSV4, and Hib) on the basis of demonstrated effectiveness or an increased risk for disease if the vaccine is withheld.
Pneumococcal Vaccines
Two types of vaccine against invasive pneumococcal disease are available in the United States: PCV and PPSV. PCV is recommended routinely for all children beginning at age 2 months. PCV is recommended routinely up to age 59 months for healthy children and up to 71 months for children with conditions that place them at high risk for invasive disease from Streptococcus pneumoniae. PPSV is licensed for persons aged ≥2 years and recommended for persons with certain underlying medical conditions (including altered immunocompetence) and for all persons aged ≥65 years. Complete recommendations on use of PCV and PPSV are available in the Recommended Immunization Schedules for Persons Aged 0 Through 18 Years and the Recommended Adult Immunization Schedule (25,49).
Influenza Vaccines
Two types of influenza vaccine are used in the United States: TIV and LAIV. Vaccination with TIV is recommended specifically for persons with altered immunocompetence, including HIV infection. LAIV usually is contraindicated for persons with altered immunocompetence, although healthy persons with anatomic or functional asplenia and household and other close contacts of persons with altered immunocompetence can receive this vaccine (68).
Meningococcal Vaccines
Two types of meningococcal vaccine are licensed in the United States: MCV4 and MPSV4. Persons with asplenia, C3 complement deficiency (51), or persistent complement component deficiency are at increased risk for meningococcal disease and should receive MCV4 or MPSV4. Quadrivalent MCV4 is licensed for persons aged 2--55 years; persons aged ≥56 years should receive MPSV4.
Hib Vaccines
Hib conjugate vaccines are available in single or combined antigen preparations. Hib vaccine is recommended routinely for all children through age 59 months. However, a single dose of Hib vaccine also may be considered for asplenic older children, adolescents, and adults who did not receive the vaccine series in childhood. Clinicians and other health-care providers might consider use of Hib vaccine for persons with HIV infection who did not receive the vaccine during infancy or childhood.
Vaccination of Contacts of Persons with Altered Immunocompetence
Household contacts and other close contacts of persons with altered immunocompetence may receive all age-appropriate vaccines, with the exception of smallpox vaccine. MMR, varicella, and rotavirus vaccines should be administered to susceptible household contacts and other close contacts of immunocompromised patients when indicated. MMR vaccine viruses are not transmitted to contacts, and transmission of varicella vaccine is rare (2,4,135). No specific precautions are needed unless the varicella vaccine recipient has a rash after vaccination, in which case direct contact with susceptible household contacts should be avoided until the rash resolves (4,135). All members of the household should wash their hands after changing the diaper of an infant. This minimizes rotavirus transmission, for an undetermined number of weeks after vaccination, from an infant who received rotavirus vaccine (136). Household and other close contacts of persons with altered immunocompetence should receive annual influenza vaccination. LAIV may be administered to healthy household and other close contacts of persons with altered immunocompetence (68).
Vaccination with Inactivated Vaccines
All inactivated vaccines can be administered safely to persons with altered immunocompetence whether the vaccine is a killed whole-organism or a recombinant, subunit, toxoid, polysaccharide, or polysaccharide protein-conjugate vaccine. If inactivated vaccines are indicated for persons with altered immunocompetence, the usual doses and schedules are recommended. However, the effectiveness of such vaccinations might be suboptimal.
Except for inactivated influenza vaccine, vaccination during chemotherapy or radiation therapy should be avoided if possible because antibody response might be suboptimal. Patients vaccinated within 14 days before starting immunosuppressive therapy or while receiving immunosuppressive therapy should be considered unimmunized and should be revaccinated at least 3 months after therapy is discontinued if immune competence has been restored.
Vaccination with Live, Attenuated Viral and Bacterial Vaccines
Severe complications have followed vaccination with live, attenuated viral and live, attenuated bacterial vaccines among persons with altered immunocompetence (137--145). Persons with most forms of altered immunocompetence should not receive live vaccines (MMR, varicella, MMRV, LAIV, zoster, yellow fever, Ty21a oral typhoid, BCG, and rotavirus).
Children with defects in phagocyte function (e.g., chronic granulomatous disease or myeloperoxidase deficiency) can receive live, attenuated viral vaccines in addition to inactivated vaccines but should not receive live, attenuated bacterial vaccines (e.g., BCG or Ty21a oral typhoid vaccines). Children with deficiencies in complement or with asplenia can receive live, attenuated viral and live, attenuated bacterial vaccines.
Persons with severe cell-mediated immunodeficiency should not receive live, attenuated viral or bacterial vaccines. However, two factors support vaccination of HIV-exposed or HIV-infected infants: 1) the HIV diagnosis might not be established in infants born to HIV-infected mothers before the age of the first rotavirus vaccine dose (only 1.5% to 3% of HIV-exposed infants in the United States will be determined to be HIV-infected), and 2) vaccine strains of rotavirus are considerably attenuated (136,146).
Children with HIV infection are at increased risk for complications from varicella and herpes zoster compared with immunocompetent children (145,147). Limited data among HIV-infected children (specifically CDC class N, A, or B with age-specific CD4+ T-lymphocyte percentages of ≥15%) indicate that varicella vaccine is immunogenic, effective, and safe (4,147). Varicella vaccine should be considered for children who meet these criteria. Eligible children should receive 2 doses of varicella vaccine with a 3-month interval between doses (4,147). Doses separated by <3 months are invalid for persons with altered immunocompetence.
Persons with HIV infection are at increased risk for severe complications if infected with measles. No severe or unusual adverse events have been reported after measles vaccination among HIV-infected persons who did not have evidence of severe immunosuppression (148--151). Therefore, MMR vaccination is recommended for all asymptomatic HIV-infected persons who do not have evidence of severe immunosuppression (age-specific CD4+ T-lymphocyte percentages of ≥15%) and for whom measles vaccination would otherwise be indicated. Similarly, MMR vaccination should be considered for mildly symptomatic HIV-infected persons (pediatric category A1 or A2 or adolescent/adult category A) who do not have evidence of severe immunosuppression (age-specific CD4+ T-lymphocyte percentages ≥15%) for whom measles vaccination would otherwise be indicated (2,146). MMRV (licensed only through age 12 years) should not be administered to children or adolescents with HIV infection (35).
HIV-infected persons who are receiving regular doses of IGIV might not respond to varicella vaccine or MMR vaccine because of the continued presence of passively acquired antibody. However, because of the potential benefit, MMR and varicella vaccines should be considered approximately 14 days before the next scheduled dose of IGIV (if not otherwise contraindicated), although an optimal immune response might not occur depending on the dose and interval since the previous dose of IGIV. Unless serologic testing indicates that specific antibodies have been produced, vaccination should be repeated (if not otherwise contraindicated) after the recommended interval (Table 5). In most cases, this is after the therapy has been discontinued. An additional dose of IGIV should be considered for persons receiving maintenance IGIV therapy who are exposed to measles or varicella ≥3 weeks after administering a standard dose (100--400 mg/kg body weight) of IGIV. Patients with leukemia, lymphoma, or other malignancies whose disease is in remission, who have restored immunocompetence, and whose chemotherapy has been discontinued for at least 3 months can receive live-virus vaccines. Persons with impaired humoral immunity (e.g., hypogammaglobulinemia or dysgammaglobulinemia) may be vaccinated with varicella vaccine (4). However, most persons with these disorders also receive periodic doses of IGIV. Appropriate spacing should be maintained between administration of IGIV and varicella vaccine to prevent an inadequate response to vaccination caused by the presence of neutralizing antibodies from the IGIV. Household members should not receive smallpox vaccine.
Zoster incidence is higher in persons with altered immunocompetence (55). Adults with most types of altered immunocompetence are expected to maintain residual immunity to varicella-zoster virus because of previous infection that protects against primary varicella but provides incomplete protection against zoster. Zoster vaccine is contraindicated in persons with primary or acquired immunodeficiency (e.g., lymphoma, leukemia, tumors involving bone marrow, and patients receiving chemotherapy) and some patients with AIDS (55). ACIP has no recommendation for or against vaccination of persons with HIV infection with CD4+ T-lymphocyte counts >200 cells/µL. Zoster vaccine may be administered to certain persons with altered immunocompetence, such as persons with HIV infection who have CD4+ T-lymphocyte counts >200 cells/µL.
Recipients of Hematopoietic Cell Transplants
A hematopoietic cell transplant (HCT) results in immunosuppression because of the hematopoietic ablative therapy administered before the transplant, drugs used to prevent or treat graft-versus-host disease, and, in some cases, from the underlying disease process necessitating transplantation (152--154). HCT involves ablation of the bone marrow followed by reimplantation of the person's own stem cells or stem cells from a donor. Antibody titers to vaccine-preventable diseases (e.g., tetanus, poliovirus, measles, mumps, rubella, and encapsulated bacteria) decrease 1--4 years after autologous or allogeneic HCT if the recipient is not revaccinated. HCT recipients of all ages are at increased risk for certain vaccine-preventable diseases, including diseases caused by encapsulated bacteria (i.e., pneumococcal, meningococcal, and Hib infections). As a result, HCT recipients should be revaccinated routinely after HCT, regardless of the source of the transplanted stem cells (152--154). Most inactivated vaccines should be initiated 6 months after the HCT (154) Inactivated influenza vaccine should be administered beginning at least 6 months after HCT and annually thereafter for the life of the patient. A dose of inactivated influenza vaccine can be given as early as 4 months after HCT, but a second dose should be considered in this situation (154). A second dose is recommended routinely for all children receiving influenza vaccine for the first time. Sequential administration of 3 doses of pneumococcal conjugate vaccine is recommended, beginning 3--6 months after the transplant, followed by a dose of PPSV (152). A 3-dose regimen of Hib vaccine should be administered beginning 6 months after transplant; at least 1 month should separate the doses (154). MMR vaccine should be administered 24 months after transplant if the HCT recipient is immunocompetent. Because of insufficient experience using varicella vaccine among HCT recipients, physicians should assess the immune status of each recipient on a case-by-case basis and determine the risk for infection before using the vaccine. If a decision is made to vaccinate with varicella vaccine, the vaccine should be administered a minimum of 24 months after transplantation if the HCT recipient is presumed to be immunocompetent (152,153).
Conditions or Drugs that Might Cause Immunodeficiencies
Asplenia and use of corticosteroids or certain drugs have the potential to be immunosuppressive and are presumed to cause some degree of altered immunocompetence.
Anatomic or Functional Asplenia
Persons with anatomic asplenia (e.g., surgical removal or congenital absence of the spleen) or functional asplenia (as occurs in persons with sickle cell disease) are at increased risk for infection by encapsulated bacteria, especially by S. pneumoniae (pneumococcus), N. meningitidis (meningococcus), and Hib (22,49,51). Children aged <5 years with anatomic or functional asplenia should receive an age-appropriate series of PCV. Persons aged ≥2 years should receive 2 doses of PPSV separated by 5 years (20,25,28,49).
Meningococcal vaccine is recommended for persons with anatomic or functional asplenia. A specific MCV4 (Menactra), is approved for persons aged 2--55 years and is the recommended vaccine for this age group unless a contraindication exists. Another MCV4 (Menveo) is approved only for ages 11--55 years. Persons aged ≥56 years should receive MPSV4. The duration of immunity after meningococcal vaccination is not certain; however, on the basis of serologic testing with recently licensed assays, revaccination is recommended for persons at continued high risk. A 3-year interval to the next dose is recommended for children at high risk who receive their first dose at ages 2--6 years. A 5-year interval is recommended for persons at high risk who receive their first dose at age ≥7 years.
No efficacy data are available on which to base a recommendation for use of Hib vaccine for older children and adults with the chronic conditions that are associated with an increased risk for Hib disease. Administering 1 dose of Hib vaccine to these patients who have not previously received Hib vaccine is not contraindicated.
Pneumococcal, meningococcal, and Hib vaccinations should be administered at least 14 days before elective splenectomy, if possible. If the vaccinations are not administered before surgery, they should be administered after the procedure as soon as the patient's condition is stable.
Corticosteroids
The amount of systemically absorbed corticosteroids and the duration of administration needed to suppress the immune system of an otherwise immunocompetent person are not well defined. Corticosteroid therapy usually is not a contraindication to administering live-virus vaccine when administration is 1) short term (i.e., <14 days); 2) a low to moderate dose (<20 mg of prednisone or equivalent per day); 3) long-term, alternate-day treatment with short-acting preparations; 4) maintenance physiologic doses (replacement therapy); or 5) topical (skin or eyes), inhaled, or by intraarticular, bursal, or tendon injection (154). No evidence of more severe reactions to live, attenuated viral vaccines has been reported among persons receiving corticosteroid therapy by aerosol, and such therapy is not a reason to delay vaccination. Although the immunosuppressive effects of steroid treatment vary, the majority of clinicians consider a dose equivalent to either ≥2 mg/kg of body weight or ≥20 mg/day of prednisone or equivalent for persons who weigh >10 kg when administered for ≥14 days as sufficiently immunosuppressive to raise concern about the safety of vaccination with live-virus vaccines (154). Corticosteroids used in greater than physiologic doses also can reduce the immune response to vaccines. Vaccination providers should defer live-virus vaccination for at least 1 month after discontinuation of high-dose systemically absorbed corticosteroid therapy administered for >14 days.
Other Immunosuppressive Drugs
When feasible, clinicians should administer all indicated vaccines to all persons before initiation of chemotherapy, before treatment with other immunosuppressive drugs, and before radiation or splenectomy. Persons receiving chemotherapy or radiation for leukemia and other hematopoietic malignancies, for solid tumors, or after solid organ transplant should be assumed to have altered immunocompetence. Live, attenuated vaccines should not be administered for at least 3 months after such immunosuppressive therapy. Inactivated vaccines administered during chemotherapy should be readministered after immune competence is regained. Children receiving chemotherapy for leukemia, lymphoma, other malignancies, or radiation generally are thought to retain immune memory after treatment, although revaccination with the common childhood vaccines after chemotherapy for acute lymphoblastic leukemia might be indicated (155). In general, revaccination of a person after chemotherapy or radiation therapy is considered unnecessary if the previous vaccination occurred before therapy and not during therapy, with the exception of recipients of HCT, who should be revaccinated as recommended previously. Determination of the level of immune memory and the need for revaccination should be made by the treating physician.
Inactivated vaccines may be administered during low-dose intermittent or maintenance therapy with immunosuppressive drugs. The safety and efficacy of live, attenuated vaccines during such therapy is unknown. Physicians should carefully weigh the risks for and benefits of providing injectable live vaccines to adult patients receiving low-dose therapies for chronic autoimmune disease. The safety and efficacy of live, attenuated vaccines administered concurrently with recombinant human immune mediators and immune modulators are unknown. Evidence that use of therapeutic monoclonal antibody preparations, especially the antitumor necrosis factor agents adalimumab, infliximab, and etanercept, causes reactivation of latent tuberculosis infection and tuberculosis disease and predisposes persons to other opportunistic infections suggests caution in the use of live vaccines in patients receiving these drugs (127--132). Until additional information becomes available, avoidance of live, attenuated vaccines during intermittent or low-dose chemotherapy or other immunosuppressive therapy is prudent, unless the benefit of vaccination outweighs the hypothetical increased risk for an adverse reaction after vaccination.
Special Situations
Concurrent Administration of Antimicrobial Agents and Vaccines
With a few exceptions, use of an antimicrobial agent is not a contraindication to vaccination. Antibacterial agents have no effect on the response to live, attenuated vaccines, except live oral Ty21a typhoid vaccine, and have no effect on inactivated, recombinant subunit, or polysaccharide vaccines or toxoids. Ty21a typhoid vaccine should not be administered to persons receiving antimicrobial agents until 24 hours after the last dose of antimicrobial (14). If feasible, to avoid a possible reduction in vaccine effectiveness, antibacterial drugs should not be started or resumed until 1 week after the last dose of Ty21a.
Antiviral drugs used for treatment or prophylaxis of influenza virus infections have no effect on the response to inactivated influenza vaccine (68). However, live, attenuated influenza vaccine should not be administered until 48 hours after cessation of therapy with antiviral influenza drugs. If feasible, to avoid possible reduction in vaccine effectiveness, antiviral medication should not be administered for 14 days after LAIV administration (68). Antiviral drugs active against herpesviruses (e.g., acyclovir or valacyclovir) might reduce the efficacy of live, attenuated varicella and zoster vaccines (4,55). These drugs should be discontinued at least 24 hours before administration of vaccines containing varicella zoster virus, including zoster vaccine, if possible. Delay use or resumption of antiviral therapy for 14 days after vaccination. No data exist to suggest that commonly used antiviral drugs have an effect on rotavirus vaccine or MMR.
Tuberculosis Screening and Skin Test Reactivity
Measles illness, severe acute or chronic infections, HIV infection, and malnutrition can create a relatively anergic state during which the tuberculin skin test (TST) might have a false-negative reaction (156--158). Although any live, attenuated measles vaccine theoretically can suppress TST reactivity, the degree of suppression is likely less than that occurring from acute infection from wild-type measles virus. Although routine TST screening of all children is no longer recommended, TST screening is sometimes needed (e.g., for well child care, school entrance, or employee health reasons) at the same time as administration of a measles-containing vaccine.
The TST and measles-containing vaccine can be administered at the same visit (preferred option). Simultaneously administering the TST and measles-containing vaccine does not interfere with reading the TST result at 48--72 hours and ensures that the person has received measles vaccine.
If the measles-containing vaccine has been administered recently, TST screening should be delayed for at least 4 weeks after vaccination. A delay in performing the TST removes the concern of any theoretical but transient suppression of TST reactivity from the vaccine.
TST screening can be performed and read before administration of the measles-containing vaccine. This option is the least favored because it delays receipt of the measles-containing vaccine. If a person is suspected to have tuberculosis, not only should the MMR vaccine be withheld before the TST, it should be withheld until after treatment has been initiated because a person with active tuberculosis who is moderately or severely ill should not receive MMR vaccine. In a general screening situation in which tuberculosis is not suspected, a TST may be administered simultaneously with live vaccines or should be deferred for 28 days after vaccination.
No data exist regarding the potential degree of TST suppression that might be associated with other live, attenuated virus vaccines (e.g., varicella or yellow fever). However, in the absence of data, following guidelines for measles-containing vaccine when scheduling TST screening and administering other live, attenuated virus vaccines is prudent. If the opportunity to vaccinate might be missed, vaccination should not be delayed only because of these theoretical considerations. Because of similar concerns about smallpox vaccine and TST suppression, a TST should not be performed until 4 weeks after smallpox vaccination (159).
A more specific test for diagnosis of tuberculosis or latent tuberculosis infection was licensed in 2005. The interferon-gamma release assay (IGRA) requires only one visit to complete and is less sensitive to the effects of previous BCG vaccination (160). The same timing guidelines that apply to the interval between a live vaccine and TST apply to IGRA (i.e., 28 days between live vaccine and IGRA if they do not occur on the same day), because IGRA (like TST) might be suppressed through immunologic mechanisms.
The potential for TST to cause boosting of results should be considered in adults who might have latent tuberculosis and have a negative initial TST (160). The two-step tuberculin test is recommended for certain situations (160). Because this test consists of two TSTs (or a TST followed by IGRA) separated by an interval of 1--3 weeks, there is a greater window of time during which live vaccine replication could suppress reactivity. If a live vaccine is administered, the first dose of a two-step TST should be delayed for 4 weeks, and if additional doses of live vaccines are indicated thereafter, they should be delayed until the second TST (or the IGRA after an initial TST).
TST or IGRA reactivity in the absence of tuberculosis disease is not a contraindication to administration of any vaccine, including live, attenuated virus vaccines. Tuberculosis disease is not a contraindication to vaccination, unless the person is moderately or severely ill. Although no studies have reported on the effects of MMR vaccine on persons with untreated tuberculosis, a theoretical basis exists for concern that measles vaccine might exacerbate tuberculosis disease (2). As a result, before administering MMR to persons with untreated active tuberculosis, initiating antituberculosis therapy is advisable (2). Considering whether concurrent immunosuppression (e.g., immunosuppression caused by HIV infection) is a concern before administering live, attenuated vaccines also is prudent.
Severe Allergy to Vaccine Components
Vaccine components can cause allergic reactions among certain recipients. These reactions can be local or systemic and can include anaphylaxis or anaphylactic-like responses (e.g., generalized urticaria or hives, wheezing, swelling of the mouth and throat, dyspnea, hypotension, and shock). Allergic reactions might be caused by the vaccine antigen, residual animal protein, antimicrobial agents, preservatives, stabilizers, or other vaccine components (161). Children who have had an apparent severe allergic reaction to a vaccine should be evaluated by an allergist to determine the responsible allergen and to make recommendations regarding future vaccination. Components of each vaccine are listed in the respective package insert. An extensive list of vaccine components and their use, as well as the vaccines that contain each component, has been published (162) and also is available from CDC (http://www.cdc.gov/vaccines).
The most common animal protein allergen is egg protein, which is found in influenza and yellow fever vaccines because they are prepared using embryonated chicken eggs. Ordinarily, persons who are able to eat eggs or egg products safely can receive these vaccines; persons who have had an anaphylactic or anaphylactic-like allergy to eggs or egg proteins generally should not receive these vaccines. Asking persons if they can eat eggs without adverse effects is a reasonable way to determine which persons might be at risk for allergic reactions from yellow fever and influenza vaccines. A regimen for administering influenza vaccine to children with egg hypersensitivity and severe asthma has been developed (163,164)
Measles and mumps vaccine viruses are grown in chick embryo fibroblast tissue culture. However, persons with a severe egg allergy can receive measles- or mumps-containing vaccines without skin testing or desensitization to egg protein (2). Rubella and varicella vaccines are grown in human diploid cell cultures and can safely be administered to persons with a severe allergy to eggs or egg proteins. The rare severe allergic reactions after measles or mumps vaccination or MMR are not thought to be caused by egg antigens but to other components of the vaccine (e.g., gelatin) (165--168). MMR, MMRV, and other vaccines contain hydrolyzed gelatin as a stabilizer. Extreme caution should be used when administering vaccines that contain gelatin to persons who have had an anaphylactic reaction to gelatin or gelatin-containing products.
Certain vaccines contain trace amounts of antimicrobial agents or other preservatives (e.g., neomycin or thimerosal) to which patients might be allergic, although such allergies are rare. The information provided in vaccine package inserts should be reviewed carefully before deciding whether a patient with such allergies should receive the vaccine. No licensed vaccine contains penicillin or penicillin derivatives.
Persons who have had anaphylactic reactions to neomycin should not receive vaccines containing neomycin. Most often, a neomycin allergy is a contact dermatitis, a manifestation of a delayed-type (cell-mediated) immune response rather than anaphylaxis (169,170). A history of delayed-type reactions to neomycin is not a contraindication for administration of these vaccines.
Thimerosal, an organic mercurial compound in use since the 1930s, is added to certain immunobiologics as a preservative. Since mid-2001, vaccines routinely recommended for young infants have been manufactured without thimerosal as a preservative. Live, attenuated vaccines have never contained thimerosal. Thimerosal-free formulations of inactivated influenza vaccine are available. Inactivated influenza vaccine also is available in formulations with trace thimerosal, in which thimerosal remains as a manufacturing residual but does not function as a preservative, and in formulations that contain thimerosal as a preservative. Thimerosal at a preservative concentration is present in certain other vaccines that can be administered to children (e.g., Td and DT). Information about the thimerosal content of vaccines is available from FDA (http://www.fda.gov/cber/vaccine/thimerosal.htm).
On the basis of limited scientific data, some investigators have asserted that receiving thimerosal-containing vaccines might induce an allergy. Allergies to thimerosal usually have been described as local delayed-type hypersensitivity reactions (171--173). Thimerosal elicits positive delayed-type hypersensitivity patch tests in 1%--18% of persons tested; however, these tests have limited or no clinical relevance (174,175). The majority of persons do not experience reactions to thimerosal administered as a component of vaccines even when patch or intradermal tests for thimerosal indicate hypersensitivity (175). A local or delayed-type hypersensitivity reaction to thimerosal is not a contraindication to receipt of a vaccine that contains thimerosal.
Latex Allergy
Latex is sap from the commercial rubber tree. Latex contains naturally occurring impurities (e.g., plant proteins and peptides) that might be responsible for allergic reactions. Latex is processed to form natural rubber latex and dry, natural rubber. Natural rubber latex and dry, natural rubber might contain the same plant impurities as latex but in lesser amounts. Natural rubber latex is used to produce medical gloves, catheters, and other products. Dry, natural rubber is used in the tip of syringe plungers, the tip on prefilled syringes, vial stoppers, and injection ports on intravascular tubing. Synthetic rubber and synthetic latex also are used in medical gloves, syringe plungers, and vial stoppers. Synthetic rubber and synthetic latex do not contain natural rubber or natural latex and do not contain impurities linked to allergic reactions. Latex or dry, natural rubber used in vaccine packaging generally is noted in the manufacturers' package inserts.
The most common type of latex sensitivity is a contact-type (type 4) allergy, usually as a result of prolonged contact with latex-containing gloves (176). However, latex allergies associated with injection procedures have been described among patients with diabetes mellitus (177--179). Allergic reactions (including anaphylaxis) after vaccinations are rare. A review of reports to VAERS identified only 28 cases of possible immediate-type anaphylactic reactions among more than 160,000 vaccine adverse event reports (180).
If a person reports a severe (anaphylactic) allergy to latex, vaccines supplied in vials or syringes that contain natural rubber latex should not be administered unless the benefit of vaccination clearly outweighs the risk for a potential allergic reaction. In these cases, providers should be prepared to treat patients who are having an allergic reaction. For latex allergies other than anaphylactic allergies (e.g., a history of contact allergy to latex gloves), vaccines supplied in vials or syringes that contain dry, natural rubber or natural rubber latex may be administered.
Vaccination of Preterm Infants
In the majority of cases, preterm infants (infants born before 37 weeks' gestation), regardless of birth weight, should be vaccinated at the same chronological age and according to the same schedule and using the same precautions as for full-term infants and children. Birth weight and size are not factors in deciding whether to vaccinate a clinically stable preterm infant (181--185), except for hepatitis B vaccination. The full recommended dose of each vaccine should be used. Divided or reduced doses are not recommended.
Decreased seroconversion rates might occur among certain preterm infants (i.e., with low birth weights [<2,000 g]) after administration of hepatitis B vaccine at birth (186). However, by the chronological age of 1 month, all preterm infants, regardless of initial birth weight, are likely to respond as adequately as larger infants (187--189). Preterm infants born to HBsAg-positive mothers and mothers with unknown HBsAg status must receive immunoprophylaxis with hepatitis B vaccine within 12 hours after birth. The initial vaccine dose should not be counted toward completion of the hepatitis B series, and 3 additional doses of hepatitis B vaccine should be administered, beginning when the infant is aged 1 month. For mothers with unknown HBsAg status, attempts should be made to determine HBsAg status. The infant must be given HBIG within 12 hours of birth unless the mother is found to be HBsAg negative (26). Infants weighing <2,000 g born to HBsAg-negative mothers should receive the first dose of the hepatitis B series at chronological age 1 month or at hospital discharge.
If a child aged at least 6 weeks has been in the hospital since birth, deferral of rotavirus vaccine is recommended until the time of discharge (136). The rotavirus vaccine series should not be initiated for infants aged ≥15 weeks, 0 days.
Breastfeeding and Vaccination
Neither inactivated nor live-virus vaccines administered to a lactating woman affect the safety of breastfeeding for women or their infants. Although live viruses in vaccines can replicate in vaccine recipients (i.e., the mother), the majority of live viruses in vaccines have been demonstrated not to be excreted in human milk. Varicella vaccine virus has not been found in human milk (190). Although rubella vaccine virus might be excreted in human milk, the virus usually does not infect the infant. If infection does occur, it is well tolerated because the virus is attenuated (191). Inactivated, recombinant, subunit, polysaccharide, and conjugate vaccines, as well as toxoids, pose no risk for mothers who are breastfeeding or for their infants. Breastfeeding is a contraindication for smallpox vaccination of the mother because of the theoretical risk for contact transmission from mother to infant. Yellow fever vaccine should be avoided in breastfeeding women (19). However, when nursing mothers cannot avoid or postpone travel to areas endemic for yellow fever in which risk for acquisition is high, these women should be vaccinated.
Limited data indicate that breastfeeding can enhance the response to certain vaccine antigens (192). There are no data to suggest that passive transfer of antibodies in human milk can affect the efficacy of live-virus vaccines. Breastfed infants should be vaccinated according to the recommended schedule (193--195).
Vaccination During Pregnancy
Risk to a developing fetus from vaccination of the mother during pregnancy is theoretical. No evidence exists of risk to the fetus from vaccinating pregnant women with inactivated virus or bacterial vaccines or toxoids (196,197). Live vaccines administered to a pregnant woman pose a theoretical risk to the fetus; therefore, live, attenuated virus and live bacterial vaccines generally are contraindicated during pregnancy. Benefits of vaccinating pregnant women usually outweigh potential risks when the likelihood of disease exposure is high, when infection would pose a risk to the mother or fetus, and when the vaccine is unlikely to cause harm. Recommendations for vaccination during pregnancy are developed using ACIP's Guiding Principles for Development of ACIP Recommendations for Vaccination During Pregnancy and Breastfeeding (198).
Pregnant women who received the last dose of tetanus-toxoid--containing vaccine >10 years previously should generally receive Td rather than Tdap while they are pregnant (16), although Tdap is not contraindicated during pregnancy. A dose of Td during pregnancy ensures adequate tetanus immunity in the mother and prevents disease in both mother and infant. In specific situations, the dose of Td can be withheld if the provider is confident the pregnant woman is immune to tetanus (199). Regardless of a recent Td vaccination, pregnant women who have not already received Tdap should receive a dose of Tdap as soon as possible after delivery to ensure pertussis immunity and reduce the risk for transmission to the newborn. Pregnant women who are not vaccinated or are only partially vaccinated against tetanus should complete the primary series (16). Women for whom Td is indicated but who did not complete the recommended 3-dose series during pregnancy should receive follow-up after delivery to ensure the series is completed. Because Tdap is recommended as a one-time dose, pregnant women who previously have received Tdap should receive Td if indicated.
Women in the second and third trimesters of pregnancy are at increased risk for hospitalization from influenza (68,200). Because vaccinating against influenza before the season begins is critical, and because predicting exactly when the season will begin is impossible, routine influenza vaccination is recommended for all women who are or will be pregnant (in any trimester) during influenza season, which in the United States is usually early October through late March (68).
IPV can be administered to pregnant women who are at risk for exposure to wild-type poliovirus infection (201). Hepatitis A, pneumococcal polysaccharide, meningococcal conjugate, and meningococcal polysaccharide vaccines should be considered for women at increased risk for those infections (49,51,202). Pregnant women who must travel to areas where the risk for yellow fever is high should receive yellow fever vaccine because the limited theoretical risk from vaccination is outweighed substantially by the risk for yellow fever infection (19,203). Hepatitis B vaccine is not contraindicated in pregnancy and should be given to a pregnant woman who has an indication for hepatitis B vaccine (26,204).
Pregnancy is a contraindication for smallpox (vaccinia) vaccine and measles-, mumps-, rubella-, and varicella-containing vaccines. Smallpox vaccine is the only vaccine known to harm a fetus when administered to a pregnant woman. In addition, smallpox vaccine should not be administered to a household contact of a pregnant woman (159). Data from studies of children born to mothers vaccinated with rubella vaccine during pregnancy demonstrate rubella antibody levels in unvaccinated infants. This could represent passive transfer of maternal antibody or a fetal antibody response to vaccine virus infection in the fetus. No cases of congenital rubella or varicella syndrome or abnormalities attributable to fetal infection have been observed among infants born to susceptible women who received rubella or varicella vaccines during pregnancy (205--207). Because of the importance of protecting women of childbearing age against rubella and varicella, reasonable practices in any vaccination program include asking women if they are pregnant or might become pregnant in the next 4 weeks; not vaccinating women who state that they are or plan to become pregnant; explaining the theoretical risk for the fetus if MMR, varicella, or MMRV vaccine were administered to a woman who is pregnant; and counseling women who are vaccinated not to become pregnant during the 4 weeks after MMR, varicella, or MMRV vaccination (2,59,205--207). MMRV is an unlikely option for a pregnant woman because the vaccine is only licensed through 12 years of age. Routine pregnancy testing of women of childbearing age before administering a live-virus vaccine is not recommended (2,4). If a pregnant woman is inadvertently vaccinated or becomes pregnant within 4 weeks after MMR or varicella vaccination, she should be counseled about the theoretical basis of concern for the fetus; however, MMR or varicella vaccination during pregnancy should not be considered a reason to terminate pregnancy (2,4,207).
Persons who receive MMR vaccine do not transmit the vaccine viruses to contacts (2). Transmission of varicella vaccine virus to contacts is rare (4). MMR and varicella vaccines should be administered when indicated to children and other household contacts of pregnant women (2,44). Infants living in households with pregnant women should be vaccinated with rotavirus vaccine according to the same schedule as infants in households without pregnant women.
Pregnant women should be evaluated for immunity to rubella and varicella and be tested for the presence of HBsAg during every pregnancy (2,26,60). Women susceptible to rubella and varicella should be vaccinated immediately after delivery. A woman found to be HBsAg positive should be monitored carefully to ensure that the infant receives HBIG and begins the hepatitis B vaccine series no later than 12 hours after birth and that the infant completes the recommended hepatitis B vaccine series on schedule (26). No known risk exists for the fetus from passive immunization of pregnant women with immune globulin preparations.
Persons Vaccinated Outside the United States
Clinicians have a limited ability to determine whether persons are protected on the basis of their country of origin and their records alone. Vaccines administered outside the United States generally can be accepted as valid if the schedule (i.e., minimum ages and intervals) is similar to that recommended in the United States. With the exception of the influenza vaccine and PPSV, only written documentation should be accepted as evidence of previous vaccination. Written records are more likely to predict protection if the vaccines, dates of administration, intervals between doses, and age at the time of vaccination are comparable to U.S. recommendations. Although vaccines with inadequate potency have been produced in other countries (208,209), the majority of vaccines used worldwide are produced with adequate quality control standards and are potent.
The number of U.S. families adopting children from outside the United States has increased substantially in the last decade (209). Adopted children's birth countries often have vaccination schedules that differ from the recommended childhood vaccination schedule in the United States. Differences in the U.S. schedule and those used in other countries include the vaccines administered, the recommended ages of administration, and the number and timing of doses.
Data are inconclusive regarding the extent to which an internationally adopted child's vaccination record reflects the child's protection. A child's record might indicate administration of MMR vaccine when only single-antigen measles vaccine was administered. A study of children adopted from orphanages in the People's Republic of China, Russia, and countries in Eastern Europe determined that 67% of children with documentation of >3 doses of DTP before adoption had nonprotective titers to these antigens (209). In contrast, children adopted from these countries who received vaccination in the community (not only from orphanages) and had documentation of ≥1 doses of DTP exhibited protective titers 67% of the time (209). However, antibody testing was performed by using a hemagglutination assay, which tends to underestimate protection and cannot directly be compared with antibody concentration (210). Data are likely to remain limited for areas other than the People's Republic of China, Russia, and Eastern Europe. Health-care providers should ensure that household contacts of international adoptees are vaccinated adequately, particularly for measles, hepatitis A, and hepatitis B (211).
Health-care providers may use one of multiple approaches if the immunogenicity of vaccines administered to persons outside the United States is in question. Repeating the vaccinations is an acceptable option that usually is safe and prevents the need to obtain and interpret serologic tests. If avoiding unnecessary injections is desired, judicious use of serologic testing might help determine which vaccinations are needed. For some vaccines, the most readily available serologic tests cannot document protection against infection. These recommendations provide guidance on possible approaches to evaluation and revaccination for each vaccine recommended in the United States (Table 14).
DTaP Vaccine
Vaccination providers can revaccinate children with DTaP vaccine without regard to recorded doses; however, data indicate increased rates of local adverse reactions after the fourth and fifth doses of DTaP (67). If a revaccination approach is adopted and a severe local reaction occurs, serologic testing for specific IgG antibody to tetanus and diphtheria toxins can be measured before administering additional doses. Protective concentration¶¶ indicates that additional doses are unnecessary and subsequent vaccination should occur as age-appropriate. No established serologic correlates exist for protection against pertussis.
For a child whose record indicates receipt of ≥3 doses of DTP or DTaP, serologic testing for specific IgG antibody to both diphtheria and tetanus toxin before additional doses is a reasonable approach. If a protective concentration is present, recorded doses are considered valid, and the vaccination series should be completed as age appropriate. An indeterminate antibody concentration might indicate immunologic memory but waning antibody; serologic testing can be repeated after a booster dose if the vaccination provider wants to avoid revaccination with a complete series.
Alternately, for a child whose records indicate receipt of ≥3 doses, a single booster dose can be administered followed by serologic testing after 1 month for specific IgG antibody to both diphtheria and tetanus toxins. If the child has a protective concentration, the recorded doses are considered valid, and the vaccination series should be completed as age appropriate. Children with an indeterminate concentration after a booster dose should be revaccinated with a complete series.
Hepatitis A Vaccine
Children aged 12--23 months without documentation of hepatitis A vaccination or serologic evidence of immunity should be vaccinated on arrival in the United States (202). Persons who have received 1 dose should receive the second dose if 6--18 months have passed since the first dose was administered.
Hepatitis B Vaccine
Persons not known to be vaccinated for hepatitis B should receive an age-appropriate series of hepatitis B vaccine. A person whose records indicate receipt of ≥3 doses of vaccine are considered protected, and additional doses are not needed if ≥1 dose was administered at age ≥24 weeks. Persons who received their last hepatitis B vaccine dose at an age <24 weeks should receive an additional dose at age ≥24 weeks. People who have received <3 doses of vaccine should complete the series at the recommended intervals and ages.
All foreign-born persons and immigrants, refugees, and internationally adopted children born in Asia, the Pacific Islands, Africa, and other regions of high or intermediate endemicity should be tested for HBsAg, regardless of vaccination status (212). Those determined to be HBsAg-positive should be monitored for development of liver disease. Household members of HBsAg-positive children or adults should be vaccinated if they are not already immune.
Hib Vaccine
Interpretation of a serologic test to verify whether children who were vaccinated >2 months previously are protected against Hib bacteria can be difficult. Because the number of vaccinations needed for protection decreases with age and because adverse events are rare (22), age-appropriate vaccination should be provided. Hib vaccination is not recommended routinely for persons aged ≥5 years (20).
MMR Vaccine
The simplest approach to resolving concerns about MMR vaccination is to revaccinate with 1 or 2 doses of MMR vaccine, depending on age. Serious adverse events after MMR vaccinations are rare (2). No evidence indicates that administering MMR vaccine increases the risk for adverse reactions among persons who are already immune to measles, mumps, or rubella as a result of previous vaccination or natural disease. Doses of measles-containing vaccine administered before the first birthday should not be counted as part of the series (2). Alternatively, serologic testing for IgG antibody to vaccine viruses indicated on the vaccination record can be considered. Serologic testing is widely available for measles and rubella IgG antibody. A person whose record indicates receipt of monovalent measles or measles-rubella vaccine on or after the first birthday and who has protective antibody against measles and rubella should receive 1 or 2 doses of MMR or MMRV as age appropriate to ensure protection against mumps and varicella (and rubella if measles vaccine alone had been administered). If a person whose record indicates receipt of MMR at age ≥12 months has a protective concentration of antibody to measles, no additional vaccination is needed unless a second dose is required for school entry.
Pneumococcal Vaccines
Many industrialized countries are now routinely using pneumococcal vaccines. Although recommendations for pneumococcal polysaccharide vaccine also exist in many countries, the vaccine might not be routinely administered. PCV and PPSV should be administered according to age-appropriate vaccination schedules or as indicated by the presence of underlying medical conditions (25,49).
Poliovirus Vaccine
The simplest approach to vaccinating with poliovirus vaccine is to revaccinate persons aged <18 years with IPV according to the U.S. schedule. Adverse events after IPV are rare (201). Children appropriately vaccinated with 3 doses of OPV in economically developing countries might have suboptimal seroconversion, including to type 3 poliovirus (201). Serologic testing for neutralizing antibody to poliovirus types 1, 2, and 3 can be obtained commercially and at certain state health department laboratories. Persons with protective titers against all three types do not need to repeat doses but should complete the schedule as age appropriate.
Rotavirus Vaccine
Rotavirus vaccination should not be initiated for infants aged ≥15 weeks, 0 days. Infants who began the rotavirus vaccine series outside the United States but who did not complete the series and who are still aged ≤8 months, 0 days, should follow the routine schedule and receive doses to complete the series. If the brand of a previously administered dose is RV5 or unknown, a total of 3 doses of rotavirus vaccine should be documented for series completion. All doses should be administered by age 8 months, 0 days.
Td and Tdap Vaccines
Children aged ≥7 years who need the primary series doses of tetanus-toxoid--containing vaccine should receive Td or Tdap as age appropriate.
Varicella Vaccine
Varicella vaccine is not available in the majority of countries. A person who lacks reliable evidence of varicella immunity should be vaccinated as age appropriate (4,20).
Zoster Vaccine
Zoster vaccination is recommended for all persons aged ≥60 years who have no contraindications, including persons who report a previous episode of zoster or who have chronic medical conditions. The vaccine should be offered at the patient's first clinical encounter with the health-care provider. The vaccine is administered as a single 0.65-mL subcutaneous dose. Zoster vaccination is not indicated to treat acute zoster, to prevent persons with acute zoster from developing postherpetic neuralgia, or to treat ongoing postherpetic neuralgia. Before administration of zoster vaccine, patients do not need to be asked about their history of varicella or to have serologic testing conducted to determine zoster immunity.
Vaccinating Persons with Bleeding Disorders
Because of the risk for hematoma formation after injections, intramuscular injections are often avoided among persons with bleeding disorders by using the subcutaneous or intradermal routes for vaccines that normally are administered intramuscularly. In one study, hepatitis B vaccine was administered intramuscularly to 153 persons with hemophilia. The vaccination was administered with a 23-gauge or smaller caliber needle, followed by application of steady pressure to the site for 1--2 minutes. The vaccinations resulted in a low (4%) bruising rate, and no patients required factor supplementation (213). Whether antigens that produce more local reactions (e.g., pertussis) would produce an equally low rate of bruising is unknown.
When hepatitis B or any other intramuscularly administered vaccine is indicated for a patient with a bleeding disorder, the vaccine should be administered intramuscularly if a physician familiar with the patient's bleeding risk determines that the vaccine can be administered by this route with reasonable safety. If the patient receives antihemophilia or similar therapy, intramuscularly administered vaccinations can be scheduled shortly after such therapy is administered. A fine-gauge needle (23 gauge or smaller caliber) should be used for the vaccination, followed by firm pressure on the site, without rubbing, for at least 2 minutes. The patient or family should be given information on the risk for hematoma from the injection. Patients receiving anticoagulation therapy presumably have the same bleeding risk as patients with clotting factor disorders and should follow the same guidelines for intramuscular administration.
Vaccination Records
Records of Health-Care Providers
Appropriate and timely vaccination documentation helps ensure not only that persons in need of recommended vaccine doses receive them but also that adequately vaccinated patients do not receive excess doses. Curtailing the number of excess doses administered to patients controls costs incurred by patients, providers, insurers, vaccination programs, and other stakeholders. In addition, excess doses of inactivated vaccines might increase the risk for an adverse reaction. Health-care providers who administer vaccines covered by the National Childhood Vaccine Injury Act are required to ensure that the permanent medical record of the recipient (or a permanent office log or file) indicates the date the vaccine was administered, the vaccine manufacturer, the vaccine lot number, and the name, address, and title of the person administering the vaccine. In addition, the provider is required to record the edition date of the VIS distributed and the date those materials were provided. The act considers a health-care provider to be any licensed health-care professional, organization, or institution, whether private or public (including federal, state, and local departments and agencies), under whose authority a specified vaccine is administered. This information should be kept for all vaccines, not just for those required by the act. Providers and staff members also should systematically update patient's permanent medical records to reflect any documented episodes of adverse events after vaccination and any serologic test results related to vaccine-preventable diseases (e.g., those for rubella screening and antibody to HBsAg).
Personal Records of Patients
Official childhood vaccination records have been adopted by every state and territory and the District of Columbia to encourage uniformity of records and to facilitate assessment of vaccination status by schools and child-care centers. The records also are key tools in vaccination education programs aimed at increasing parental and patient awareness of the need for vaccines. A permanent vaccination record card should be established for each newborn infant and maintained by the parent or guardian. The parent or guardian should be educated about the importance of keeping the record up to date and instructed to keep the record indefinitely as part of the child's permanent medical record. These cards should be distributed to new mothers before discharge from the hospital. Using vaccination record cards for adolescents and adults also is encouraged. Standardized adult vaccination records are available at http://www.immunize.org.
Immunization Information Systems
IISs (formerly referred to as immunization registries) are confidential, population-based, computerized information systems that collect and consolidate vaccination data from multiple health-care providers within a geographic area. IISs are a critical tool that can increase and sustain vaccination coverage by consolidating vaccination records from multiple providers, generating reminder and recall vaccination notices for each person, and providing official vaccination forms and vaccination coverage assessments (214).
Changing vaccination providers during the course of an individual's vaccination series is common in the United States. The 2007 National Health Interview Survey Summary Health Statistics for U.S. Children documented that 95% of children have a usual place of health care; 6% go to more than one health venue most of the time. Individual eligibility for Medicaid and resulting enrollment in Medicaid managed-care health plans tends to be sporadic, with an average duration of 9 months and a median of <12 months in 2000 (215). In addition to changes in providers, the vaccination records of persons who have changed vaccination providers often are unavailable or incomplete or might not have been entered into an IIS (214). Missing or inaccurate information regarding vaccines received previously might preclude accurate determination of which vaccines are indicated at the time of a visit, resulting in administration of extra doses.
A fully operational IIS also can prevent duplicate vaccinations, limit missed appointments, reduce vaccine waste, and reduce staff time required to produce or locate vaccination records or certificates. Most IISs have additional capabilities, such as vaccine management, maintenance of lifetime vaccination histories, and interoperability with other health information systems. The National Vaccine Advisory Committee strongly encourages development of community- or state-based IISs and recommends that vaccination providers participate in these systems when possible. One of the national health objectives for 2010 was 95% participation of children aged <6 years in a fully operational population-based IIS (objective 20.1) (216). Participating in an IIS means having two or more vaccinations recorded in the IIS. 2008 IIS data indicate that approximately 75% of children aged <6 years with two or more vaccinations were participating in IISs (217). Inclusion of adults into IISs also would be worthwhile. A new national health objective for 2020 is 80% of adolescents (aged 11--18 years) with two or more age-appropriate vaccinations recorded in IISs (http://www.healthypeople.gov/hp2020/objectives/topicarea.aspx?id=30&topicarea=immunization+and+infectious+diseases).
Vaccination Programs
In the United States, vaccination programs have eliminated many vaccine-preventable diseases and reduced the incidence of several others (218). Because infants and young children were the principle recipients of most vaccines developed during the twentieth century (e.g., poliovirus vaccine), many persons in the United States might believe that vaccinations are solely for the young; however, vaccinations are recommended for persons of all ages (20,28). Improved vaccination coverage can result in additional reductions in the incidence of vaccine-preventable diseases and decrease associated morbidity and mortality. Universal vaccination is a critical part of quality health care and should be accomplished through routine and catch-up vaccination provided in physicians' offices, public health clinics, and other appropriate complementary settings. Every patient encounter represents an opportunity to review and, when needed, improve a patient's vaccination status through administration of recommended vaccines.
Vaccination of Children and Adolescents
Physicians and other pediatric vaccination providers should adhere to the standards for child and adolescent vaccination practices (8). These standards were published by the National Vaccine Advisory Committee and define appropriate vaccination practices for both public and private sectors. The standards provide guidance on practices that eliminate barriers to vaccination, including eliminating unnecessary prerequisites for receiving vaccinations, eliminating missed opportunities to vaccinate, improving procedures to assess vaccination needs, enhancing knowledge about vaccinations among parents and providers, and improving management and reporting of adverse events. In addition, the standards address the importance of recall and reminder systems and using assessments to monitor clinic or office vaccination coverage levels. Health-care providers should simultaneously administer as many vaccine doses as possible as indicated on the Recommended Immunization Schedules for Persons Aged 0 Through 18 Years (20).
Community health-care providers, as well as staff members at both state and local vaccination programs, should coordinate with partners to maximize outreach to populations at risk for undervaccination and vaccine-preventable diseases. For example, the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is a categorical federal grant program administered by the U.S. Department of Agriculture through state health departments. The program provides supplemental foods, health-care referrals, and nutrition education to low-income pregnant, breastfeeding, or postpartum women, as well as to infants and children aged <5 years. More than 8.7 million people participated in this program in 2008 (http://www.fns.usda.gov/pd/wicmain.htm). In collaboration, WIC and state vaccination programs should assess regularly the vaccination coverage levels of WIC participants and develop new strategies and aggressive outreach procedures in sites with coverage levels <90%. Vaccination programs and private providers are encouraged to refer eligible children to obtain WIC nutritional services (219).
Adolescents
Vaccinations are recommended throughout life, including during adolescence. The age range for adolescence is defined as 11--21 years by many professional associations, including the American Academy of Pediatrics and the American Medical Association (220,221). Definitions of these age cutoffs differ depending on the source of the definition and the source's purpose for creating a definition. Vaccination of adolescents is critical for preventing diseases for which adolescents are at particularly high or increasing risk, such as meningococcal disease and human papillomavirus infection. Three vaccines recommended for adolescents have been licensed since 2005: MCV4, HPV, and the Tdap vaccine. A second dose of varicella vaccine is recommended for persons who received 1 dose of varicella vaccine after age 12 months, and this group includes many adolescents. In addition, annual seasonal influenza vaccination is recommended for persons aged >6 months who have no contraindications. To ensure vaccine coverage, clinicians and other health-care providers who treat adolescents must screen for a complete vaccination history on every occasion that an adolescent has an office visit.
National goals for vaccination coverage for adolescents aged 13--15 years were included in Healthy People 2010 (216). Targets for 90% coverage were specified for established vaccine recommendations including those for 3 doses of hepatitis B vaccine, 1 dose of MMR vaccine, 1 dose of varicella vaccine (excluding persons with a history of varicella), and 1 dose of Td vaccine. Results of the published 2008 National Immunization Survey---Teen indicate that, for the first time, coverage targets for hepatitis B and MMR vaccines were met. For ≥1 dose of varicella, coverage increased to 86%. However, coverage for ≥1 dose of either Td or Tdap was unchanged at 71%, remaining below the coverage target of 90%. Coverage for MCV4 is 42%. New objectives from Healthy People 2020 include 1 dose of Tdap and ≥2 doses of varicella vaccine (excluding persons who have had varicella disease) (http://www.healthypeople.gov/hp2020/objectives/topicarea.aspx?id=30&topicarea=immunization+and+infectious+diseases).
Ensuring adolescents receive routine and catch-up vaccination and increasing vaccination coverage in this age group present challenges. In general, adolescents do not visit health-care providers frequently. Health-care providers should promote annual preventive visits (217), including one specifically for adolescents aged 11 and 12 years. The annual visits should be used as opportunities to provide routinely recommended vaccine doses, additional catch-up doses needed for lapsed vaccine series, vaccines recommended for high-risk groups, additional doses that might have been recently recommended, and other recommended health-care services.
All vaccine doses should be administered according to ACIP vaccine-specific statements and with the most recent schedules for both routine and catch-up vaccination. Before leaving any visit for medical care, adolescents should be encouraged to schedule return visits for any additional vaccine doses needed. During visits that occur outside of influenza season, providers should discuss and recommend seasonal influenza vaccination and make explicit plans for vaccination, including timing and anticipated setting (e.g., health-care provider's office, school, or pharmacy). Catch-up vaccination with multidose adolescent vaccines generally can occur according to the routine dosing schedule for these vaccines, although in some circumstances the clinician or health-care provider might use minimum intervals for vaccine doses. These circumstances include an outbreak that increases risk for disease or the likelihood that doses will be missed in the future (e.g., because of an impending loss of health-care coverage or transportation challenges). Because of lack of efficacy data for HPV vaccine administration using minimum intervals, providers are encouraged, when possible, to use routine dosing intervals for females aged 11--26 years who have not yet received 3 HPV vaccine doses as recommended (20,28).
One of the challenges of adolescent vaccination is ensuring that current, complete vaccination histories are available. Insurers, covered services, or reimbursement levels can change, and these changes might affect reimbursement for vaccine doses and vaccination services directly while also causing disruptions in an adolescent's access to vaccination providers or venues. In circumstances in which a vaccination record is unavailable, vaccination providers should attempt to obtain this information from various sources (e.g., parent, previous providers, or school records). More detail about how to obtain these records is available at from CDC at http://www.cdc.gov/vaccines/recs/immuniz-records.htm. With the exception of influenza and pneumococcal polysaccharide vaccines, if documentation of a vaccine dose is not available, the adolescent should be considered unvaccinated for that dose. Regardless of the venue in which an adolescent receives a dose of vaccine, that vaccine dose should be documented in the patient's chart or in an office log, and the information should be entered into an IIS. The adolescent also should be provided with a record card that documents the vaccination history.
Adult Vaccination
The incidence of vaccine-preventable diseases in adults in the United States is high. Approximately 45,000 adults die each year from vaccine-preventable diseases, the majority from influenza (222). In 2008, an estimated 44,000 cases of invasive pneumococcal disease were reported with approximately 4,500 deaths, the majority occurring among persons aged >35 years (http://www.cdc.gov/abcs/survreports/spneu08.htm). Because of recent licensure of new vaccines approved for adults and new ACIP recommendations for the use of many vaccines in adults, providers of adult health care now share a greater responsibility for putting these recommendations into practice. In 2009, an estimated 4,070 deaths were caused by infection with the HPV strains causing the majority of cervical cancers in this country that are preventable with HPV vaccine and routine Papanicolaou smear testing (http://www.cancer.org/docroot/home/index.asp). Herpes zoster causes considerable morbidity in adults aged >50 years (55). A painful complication of herpes zoster infection is postherpetic neuralgia, which is characterized by severe pain that can persist for up to a year after the herpes zoster rash has subsided. A vaccine to prevent herpes zoster was licensed in 2006.
In 2003, the National Vaccine Advisory Committee published standards for adult vaccination (222). These standards include ensuring vaccine availability, review of records, communicating the risks and benefits of vaccination, use of standing orders, and recommending simultaneous administration of all indicated doses according to the Recommended Adult Immunization Schedule (28).
Vaccination with vaccines recommended for all adults or for those in specific age groups is generally cost-effective, if not cost-saving, for society. The National Commission on Prevention Priorities (NCPP) ranked clinical preventive services based on clinically preventable disease effects and cost-effectiveness (223). In the NCPP report, influenza vaccination for adults aged ≥50 years and pneumococcal vaccination for adults aged ≥65 years ranked high, with 8 of 10 possible points in the scoring system used. Most other studies have found influenza vaccination reduces or minimizes health care, societal, and individual costs or the productivity losses and absenteeism associated with influenza illness (224--226). Economic analyses among adults aged ≥65 years have found influenza vaccination to be cost-effective (225--227).
A 2008 study of the cost-effectiveness of PPSV demonstrated that vaccination resulted in a gain of $3,341 per quality-adjusted life year; the result is sensitive to vaccine uptake assumptions (228). PPSV administered at ages 50--65 years might be clinically favorable and, depending on cost-effectiveness criteria used, economically favorable (228).
Hepatitis B vaccine is not recommended routinely for all adults. However, multiple studies have established the cost-effectiveness of providing hepatitis B vaccinations at counseling and testing sites for HIV and other sexually transmitted diseases, correctional institutions, drug-abuse treatment centers, and other settings serving adults at risk for hepatitis B virus infection (229--230).
Four studies have estimated the cost-effectiveness of a routine herpes zoster vaccination program of immunocompetent persons aged ≥60 years (231--234). At a vaccine cost of $150 per dose, the societal costs of routinely vaccinating immunocompetent persons aged ≥60 years range from $27,000 to $112,000 per quality-adjusted life year gained (231--234). The estimated cost per quality-adjusted life year for zoster vaccination covers a wide range that appears acceptable compared with either standard thresholds or other established interventions but is at the intermediate to high end of that range.
Vaccination rates in adults are considered suboptimal (235--238). Healthy People 2010 goals for adult vaccination coverage with influenza and pneumococcal polysaccharide vaccines are 90% for each vaccine. For the 2007--2008 season, influenza vaccination coverage among adults aged 50--64 years was 34%, and coverage among adults aged ≥65 years was 66% (67). In 2008, 60% of adults aged ≥65 years received a dose of PPSV (http://www.cdc.gov/nchs/data/hestat/vaccine_coverage.htm). New Healthy People 2020 goals for influenza and pneumococcal polysaccharide vaccines include specific subsets of adults, including institutionalized adults aged ≥18 years (for both influenza and pneumococcal polysaccharide vaccines) and noninstitutionalized adults at high risk aged >18 years (for pneumococcal polysaccharide vaccine) (http://www.healthypeople.gov/hp2020/objectives/topicarea.aspx?id=30&topicarea=immunization+and+infectious+diseases).
The most substantial barrier to vaccination coverage is lack of knowledge about these vaccines among adult patients and adult providers. Other barriers are cost (lack of additional insurance to Medicare) (239) and the lack of financing mechanisms for newly licensed and recommended vaccines.
A common challenge for health-care providers is vaccinating adults with unknown vaccination records. In general (except for influenza and pneumococcal polysaccharide vaccines), adults should receive a vaccine dose if the dose is recommended and no record of previous administration exists. If an adult has a record of military service and does not have records available, providers can assume that the person has received all vaccines recommended by the military at the time of service entry. Serologic testing might be helpful in clarifying immune status if questions remain because at different times and depending on military assignments, there might be interservice and individual differences.
Evidence-Based Interventions to Increase Vaccination Coverage
The independent, nonfederal Task Force on Community Preventive Services, whose membership is appointed by CDC, provides public health decision-makers with recommendations on population-based interventions to promote health and prevent disease, injury, disability, and premature death. The recommendations are based on systematic reviews of the scientific literature about effectiveness and cost-effectiveness of these interventions. In addition, the task force identifies critical information about the other effects of these interventions, the applicability to specific populations and settings, and the potential barriers to implementation. Additional information, including updates of published reviews, is available from The Community Guide at http://www.thecommunityguide.org.
Beginning in 1996, the task force systematically reviewed published evidence on the effectiveness and cost-effectiveness of population-based interventions to increase coverage of vaccines recommended for routine use among children, adolescents, and adults. A total of 197 articles were identified that evaluated a relevant intervention, met inclusion criteria, and were published during 1980--1997. Reviews of 17 specific interventions were published in 1999 (235--238). Using the results of their review, the task force made recommendations about the use of these interventions (238). Several interventions were identified and recommended on the basis of published evidence. Follow-up reviews were published in 2000, and a review of interventions to improve the coverage of adults at high risk was conducted in 2005 (238,239). The interventions and the recommendations are summarized in this report (Table 15).
In 1997, the task force categorized as a recommended strategy vaccination requirements for child care, school, and college (236). When appropriate, health agencies should take necessary steps to develop and enforce these requirements.
A 2008 update of the original task force systematic review of the evidence on the effectiveness of provider assessment and feedback for increasing coverage rates found that this strategy remains an effective intervention. A later update reviewed 19 new studies published during 1997--2007. The updated review supports the original task force recommendation for use of assessment and feedback based on strong evidence of effectiveness. The task force reviewed studies of assessment and feedback as a strategy that were conducted in a range of settings, including private practice, managed care, public health, community health settings, and academic centers. Studies have assessed the effectiveness of this intervention to improve coverage with MMR, DTP, DTaP, Hib, influenza, pneumococcal, and Td vaccines (237). The most updated information on this review is available at http://www.thecommunityguide.org/vaccines/universally/providerassessment.html. As recognized by the task force, routine assessment and feedback of vaccination rates obtained at the provider site is one of the most effective strategies for achieving high, sustainable vaccine coverage. Since 1995, all states receiving federal funds for vaccination programs have been required to conduct annual assessments of vaccination rates both in public health clinics and in private provider offices. Primarily to aid local and state health departments in their efforts to conduct assessments and assist providers, CDC has developed numerous software applications to measure vaccination rates in provider practices.
Other General Programmatic Issues
Programmatic challenges, evolving issues, and effective interventions related to adult and adolescent vaccination programs have been described by other advisory groups and expert groups. Additional evidence-based approaches are being developed for certain issues (e.g., settings for adolescent vaccination delivery) through ongoing research and evaluation. Among current programmatic challenges, vaccine financing is especially difficult because certain problems and solutions differ markedly from one state to another. Practitioners interested in beginning or continuing to provide vaccinations to patients are encouraged to consult with local and state public health vaccination programs to learn about publicly funded programs that might be available in their areas for patients who need vaccination but have insufficient health insurance coverage and no financial resources. If not already participating, providers who care for adolescents and children aged <19 years should enroll in the Vaccines for Children Program (http://www.cdc.gov/vaccines/programs/vfc/default.htm). Through this program's provision of ACIP-recommended, federally purchased vaccines, participating providers are able to fully vaccinate eligible children whose parents might not otherwise be able to afford the vaccinations. Interested providers are encouraged to work with insurers, state and specialty-specific medical organizations, vaccine manufacturers, and other stakeholders to address financial barriers to achieving high vaccination coverage. With availability of safe and effective vaccines for 17 vaccine-preventable diseases, the capacity for realizing the potential benefits of these products in the United States depends on reaching children, adolescents, and adults through dedicated, knowledgeable vaccination providers and efficient, strong vaccination programs at local, state, and federal levels.
Vaccine Information Sources
In addition to these general recommendations, the following sources contain specific and updated vaccine information.
CDC-INFO Contact Center
The CDC-INFO contact center is supported by CDC and provides public health-related information, including vaccination information, for health-care providers and the public, 24 hours a day, 7 days a week (telephone [English and Spanish]: 800-232-4636; telephone [TTY]: 800-232-6348).
CDC's National Center for Immunization and Respiratory Diseases
CDC's National Center for Immunization and Respiratory Diseases website provides direct access to vaccination recommendations of ACIP, vaccination schedules, automated child schedulers, an adult immunization scheduler, vaccine safety information, publications, provider education and training, and links to other vaccination-related websites (http://www.cdc.gov/vaccines).
MMWR
ACIP recommendations regarding vaccine use, statements of vaccine policy as they are developed, and reports of specific disease activity are published by CDC in the MMWR series and can be found at http://www.cdc.gov/vaccines/pubs/ACIP-list.htm. Electronic subscriptions are free (http://www.cdc.gov/mmwr/mmwrsubscribe.html). Subscriptions to print versions also are available from the Superintendent of Documents, U.S. Government Printing Office, Washington, D.C. 20402-9235 (telephone: 202-512-1800).
American Academy of Pediatrics (AAP)
Every 3 years, AAP issues the Red Book: Report of the Committee on Infectious Diseases, which contains a composite summary of AAP and ACIP recommendations concerning infectious diseases and vaccinations for infants, children, and adolescents (telephone: 888-227-1770; website: http://www.aap.org).
American Academy of Family Physicians (AAFP)
Information from the professional organization of family physicians is available at http://www.aafp.org.
Immunization Action Coalition
The Immunization Action Coalition provides extensive free provider and patient information, including translations of VISs into multiple languages. Printed materials are reviewed by CDC for technical accuracy (http://www.immunize.org and http://www.vaccineinformation.org).
National Network for Immunization Information
This National Network for Immunization Information is an affiliation of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, AAP, the American Nurses Association, AAFP, the National Association of Pediatric Nurse Practitioners, the American College of Obstetricians and Gynecologists, the University of Texas Medical Branch, the Society for Adolescent Medicine, and the American Medical Association. This source provides the public, health professionals, policy makers, and the media with up-to-date, scientifically valid information (http://www.immunizationinfo.org).
Vaccine Education Center
Located at the Children's Hospital of Philadelphia, the Vaccine Education Center provides patient and provider vaccine information (http://www.vaccine.chop.edu).
Institute for Vaccine Safety
Located at Johns Hopkins University School of Public Health, the Institute for Vaccine Safety provides information about vaccine safety concerns and objective and timely information to physicians and health-care providers and parents (http://www.vaccinesafety.edu).
Group on Immunization Education of the Society of Teachers of Family Medicine
The Group on Immunization Education of the Society of Teachers of Family Medicine provides information for clinicians, including the free program Shots. Shots includes the childhood, adolescent, and adult schedules for iPhone, Palm, and Windows devices, as well as online versions (http://www.immunizationed.org).
State and Local Health Departments
State and local health departments provide technical advice through hotlines, e-mail, and websites, including printed information regarding vaccines and immunization schedules, posters, and other educational materials.
Acknowledgments
The members of the Advisory Committee on Immunization Practices are grateful for the contributions of Doug Campos-Outcalt MD, University of Arizona College of Medicine, Phoenix, Arizona; Patricia Stinchfield, MS, National Association of Pediatric Nurse Practitioners, Cherry Hill, New Jersey; and Christine Robinette Curtis, MD, Shannon Stokely, MPH, and Gregory Wallace, MD, CDC, Atlanta, Georgia.
References
- Plotkin SA. Immunologic correlates of protection induced by vaccination. Pediatr Infect Dis J 2001;20:63--75.
- CDC. Measles, mumps, and rubella---vaccine use and strategies for elimination of measles, rubella, and congenital rubella syndrome and control of mumps: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1998;47(No. RR-8).
- Watson JC, Pearson JA, Markowitz LE, et al. An evaluation of measles revaccination among school-entry-aged children. Pediatrics 1996;97:613--8.
- CDC. Prevention of varicella: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2007;56(No. RR-4).
- CDC. Human rabies prevention---United States, 2008: recommendations of the Advisory Committee on Immunization Practices. MMWR 2008;57(No. RR-3).
- Levine L, Edsall G. Tetanus toxoid: what determines reaction proneness [Letter]. J Infect Dis 1981;144:376.
- Edsall G, Elliot MW, Peebles TC, Levine L, Eldred MC. Excessive use of tetanus toxoid boosters. JAMA 1967;202:17--9.
- National Vaccine Advisory Committee. Standards for child and adolescent immunization practices. Pediatrics 2003;112:958--63.
- Hutchins SS, Escolan J, Markowitz LE, et al. Measles outbreak among unvaccinated preschool-age children: opportunities missed by health care providers to administer measles vaccine. Pediatrics 1989;83:369--74.
- Deforest A, Long SS, Lischner HW, et al. Simultaneous administration of measles-mumps-rubella vaccine with booster doses of diphtheria-tetanus-pertussis and poliovirus vaccines. Pediatrics 1988;81:237--46.
- King GE, Hadler SC. Simultaneous administration of childhood vaccines: an important public health policy that is safe and efficacious. Pediatr Infect Dis J 1994;13:394--407.
- Dashefsky B, Wald E, Guerra N, Byers C. Safety, tolerability, and immunogenicity of concurrent administration of Haemophilus influenzae type B conjugate vaccine (meningococcal protein conjugate) with either measles-mumps-rubella vaccine or diphtheria-tetanus-pertussis and oral poliovirus vaccines in 14- to 23-month-old infants. Pediatrics 1990;85:682--9.
- Giammanco G, Li Volti S, Mauro L, et al. Immune response to simultaneous administration of a recombinant DNA hepatitis B vaccine and multiple compulsory vaccines in infancy. Vaccine 1991;9:747--50.
- CDC. Typhoid immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1994;43(No. RR-14).
- DeStefano F, Goodman RA, Noble GR, McClary GD, Smith SJ, Broome CV. Simultaneous administration of influenza and pneumococcal vaccines. JAMA 1982;247:2551--4.
- CDC. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine. MMWR 2006;55(No. RR-17).
- Yvonnet B, Coursaget P, Deubel V, Diop-Mar I, Digoutte JP, Chiron J. Simultaneous administration of hepatitis B and yellow fever vaccines. J Med Virol 1986;19:307--11.
- Stefano I, Sato HK, Pannuti CS, et al. Recent immunization against measles does not interfere with the sero-response to yellow fever vaccine. Vaccine 1999;17:1042--6.
- CDC. Yellow fever vaccine: recommendations of the Immunization Practices Advisory Committee (ACIP), 2010. MMWR 2010:59(No. RR-7).
- CDC. Recommended immunization schedules for persons aged 0 through 18 years---United States, 2011. MMWR 2011;60(5).
- Shinefield HR, Black S, Ray P, et al. Safety and immunogenicity of heptavalent pneumococcal CRM197 conjugate vaccine in infants and toddlers. Pediatr Infect Dis J 1999;18:757--63.
- CDC. Haemophilus b conjugate vaccines for prevention of Haemophilus influenzae type b disease among infants and children two months of age and older: recommendations of the ACIP. MMWR 1991;40(No. RR-1).
- CDC. Pertussis vaccination: use of acellular pertussis vaccines among infants and young children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1997;46(No. RR-7).
- CDC. Preventing tetanus, diphtheria, and pertussis among adolescents: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2006;55(No. RR-3).
- CDC. Prevention of pneumococcal disease among infants and young children---use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2010;59(No. RR-11).
- CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP); part 1: immunization of infants, children, and adolescents. MMWR 2005;54(No. RR-16).
- American Academy of Pediatrics. Committee on Infectious Diseases. Policy statement: recommended childhood and adolescent immunization schedules---United States, 2010. Pediatrics 125:195--6.
- CDC. Recommended adult immunization schedule---United States, 2011. MMWR 2011;60(4).
- Woodin KA, Rodewald LE, Humiston SG, Carges MS, Schaffer SJ, Szilagyi PG. Physician and parent opinions: are children becoming pincushions from immunizations? Arch Pediatr Adolesc Med 1995;149:845--9.
- Kuppermann M, Nease RF, Ackerson LM, et al. Parents' preferences for outcomes associated with childhood vaccinations. Pediatr Infect Dis J 2000;19:129--33.
- Meyerhoff A, Jacobs RJ, Greenberg DP, Yagoda B, Castles CG. Clinician satisfaction with vaccination visits and the role of multiple injections: results from the COVISE study (Combination Vaccines Impact on Satisfaction and Epidemiology). Clin Pediatr 2004;43:87--93.
- Marshall GS, Happe LE, Lunacsek, OE, et al. Use of combination vaccines is associated with improved coverage rates. Pediatr Infect Dis J 2007; 26:496--500.
- Kalies H, Grote V, Verstraeten T, et al. The use of combination vaccines has improved timeliness of vaccination in children. Pediatr Infect Dis J. 2006;25:507--12.
- Happe LE, Lunacsek OE, Kruzikas DT, et al. Impact of a pentavalent combination vaccine on immunization timeliness in a state Medicaid population. Pediatr Infect Dis J 2009;28:98--101.
- CDC. Recommendations from the Advisory Committee on Immunization Practices (ACIP) regarding administration of combination MMRV vaccine. MMWR 2010;59(No. RR-3).
- Thompson LA, Irigoyen M, M LA, et al. The impact of DTaP-IPV-HB vaccine on use of health services for young infants. Pediatr Infect Dis J 2006;25:826--31.
- Denoel PA, Goldblatt D, de Vleeshauwer I, et al. Quality of the Haemophilus influenza type b (Hib) antibody response induced by diphtheria-tetanus-acellular pertussis/Hib combination vaccines. Clin Vaccine Immunol 2007;14:1362--9.
- Weniger BG, Chen RT, Jacobsen SH, et al. Addressing the challenges to immunization practice with an economic algorithm for vaccine selection. Vaccine 1998;16:1885--97.
- CDC. Notice to readers. FDA approval for infants of a Haemophilus influenzae type b conjugate and hepatitis B (recombinant) combined vaccine. MMWR 1997;46:107--9.
- CDC. FDA approval of a Haemophilus b conjugate vaccine combined by reconstitution with an acellular pertussis vaccine. MMWR 1996;45:993--5.
- CDC. Notice to readers: FDA approval for a combined hepatitis A and B vaccine. MMWR 2001;50:806--7.
- CDC. Notice to readers. FDA licensure of diphtheria and tetanus toxoids and acellular pertussis adsorbed, hepatitis B (recombinant), and poliovirus vaccine combined, (PEDIARIX) for use in infants. MMWR 2003;52:203--4.
- CDC. Notice to readers. Licensure of a combined live attenuated measles, mumps, rubella, and varicella vaccine. MMWR 2005;54:1212--4.
- CDC. Licensure of a diphtheria and tetanus toxoids and acellular pertussis adsorbed and inactivated poliovirus vaccine and guidance for use as a booster dose. MMWR 2008;57:1078--9.
- CDC. Licensure of a diphtheria and tetanus toxoids and acellular pertussis adsorbed, inactivated poliovirus, and Haemophilus b conjugate vaccine and guidance for use in infants and children. MMWR 2008;57:1079--80.
- Plotkin S. Correlates of vaccine-induced immunity. Clin Infec Dis 2008;47:401--9.
- Midthun K, Horne AD, Goldenthal KL. Clinical safety evaluation of combination vaccines. Dev Biol Stand 1998;95:245--9.
- Pichichero ME. Impact of a birth dose of hepatitis B vaccine on the reactogenicity and immunogenicity of diphtheria-tetanus-acellular pertussis-hepatitis B-inactivated poliovirus-Haemophilus influenzae type b combination vaccination. Pediatr Infect Dis J 2002;21:854--9.
- CDC. Prevention of pneumococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1997;46(No. RR-8).
- CDC. Diphtheria, tetanus, and pertussis: recommendations for vaccine use and other preventive measures: recommendations of the Immunization Practices Advisory Committee (ACIP). MMWR 1991;40(RR-10).
- CDC. Prevention and control of meningococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2005;54 (RR-7).
- Petralli JK, Merigan TC, Wilbur JR. Action of endogenous interferon against vaccinia infection in children. Lancet 1965;2:401--5.
- Petralli, JK, Merigan TC, Wilbur JR. Circulating interferon after measles vaccination. N Engl J Med 1965;273:198--201.
- Verstraeten T, Jumaan AO, Mullooly JP, et al. A retrospective cohort study of the association of varicella vaccine failure with asthma, steroid use, age at vaccination, and measles-mumps-rubella vaccination. Pediatrics 2003;112:98--103.
- CDC. Prevention of herpes zoster: Recommendations of the Advisory Committee on Immunization Practices. MMWR 2008;57(No. RR-5).
- Siber GR, Werner BC, Halsey NA, et al. Interference of immune globulin with measles and rubella immunization. J Pediatr 1993;122:204--11.
- Mason W, Takahashi M, Schneider T. Persisting passively acquired measles antibody following gamma globulin therapy for Kawasaki disease and response to live virus vaccination [Abstract 311]. Presented at the 32nd meeting of the Interscience Conference on Antimicrobial Agents and Chemotherapy; Los Angeles, California; October 1992.
- Kaplan JE, Nelson DB, Schonberger LB, et al. Effect of immune globulin on the response to trivalent oral poliovirus and yellow fever vaccinations. Bull World Health Organ 1984;62:585--90.
- Black NA, Parsons A, Kurtz JB, McWhinney N, Lacey A, Mayon-White RT. Post-partum rubella immunization: a controlled trial of two vaccines. Lancet 1983;2:990--2.
- CDC. Control and prevention of rubella: evaluation and management of suspected outbreaks, rubella in pregnant women, and surveillance for congenital rubella syndrome. MMWR 2001;50(No. RR-12).
- Siber GR, Snydman DR. Use of immune globulin in the prevention and treatment of infections. In: Remington J, Swartz M, eds. Current clinical topics in infectious diseases, vol. 12. Oxford: Blackwell Scientific; 1992.
- Greenberg DP, Lieberman JM, Marcy SM, et al. Enhanced antibody responses in infants given different sequences of heterogeneous Haemophilus influenzae type b conjugate vaccines. J Pediatr 1995;126:206--11.
- Anderson EL, Decker MD, Englund JA, et al. Interchangeability of conjugated Haemophilus influenzae type b vaccines in infants. JAMA 1995;273:849--53.
- Piazza M, Abrescia N, Picciotto L, et al. Demonstration of the interchangeability of 2 types of recombinant anti-hepatitis-B vaccine. Boll Soc Ital Biol Sper 1993;69:273--80.
- Bryan JP, Henry CH, Hoffman AG, et al. Randomized, cross-over, controlled comparison of two inactivated hepatitis A vaccines. Vaccine 2000;19:743--50.
- Greenberg DP, Pickering LK, Senders SD, et al. Interchangeability of two diphtheria-tetanus-acellular pertussis vaccines in infancy. Pediatrics 2002;109:666--72.
- CDC. Use of diphtheria toxoid-tetanus toxoid-acellular pertussis vaccine as a five-dose series: supplemental recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2000;49(No. RR-13).
- CDC. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR 2010;59(No. RR-8).
- Szilagyi PG, Rodewald LE. Missed opportunities for immunizations: a review of the evidence. J Public Health Manag Pract 1996;2:18--25.
- Halsey NA, Boulos R, Mode F, et al. Response to measles vaccine in Haitian infants 6 to 12 months old: influence of maternal antibodies, malnutrition, and concurrent illnesses. N Engl J Med 1985;313:544--9.
- Ndikuyeze A, Munoz A, Stewart S, et al. Immunogenicity and safety of measles vaccine in ill African children. Int J Epidemiol 1988;17:448--55.
- Lindegren ML, Atkinson WA, Farizo VM, Stehr-Green PA. Measles vaccination in pediatric emergency departments during a measles outbreak. JAMA 1993;270:2222--3.
- Atkinson W, Markowitz L, Baughman A, et al. Serologic response to measles vaccination among ill children [Abstract 422]. Abstracts of the 32nd Interscience Conference on Antimicrobial Agents and Chemotherapy; October 1992; Anaheim, California.
- Orenstein WA, Rodewald LE, Hinman AR, Schuchat A. Immunization in the United States. In: Vaccines. Plotkin SA, Orenstein WA, Offit PA, eds. 5th ed. China: Saunders/Elsevier; 2008.
- Lewis T, Osborn LM, Lewis K, Brockert J, Jacobsen J, Cherry JD. Influence of parental knowledge and opinions on 12-month diphtheria, tetanus, and pertussis vaccination rates. Am J Dis Child 1988;142:283--6.
- Farizo KM, Stehr-Green PA, Markowitz LE, Patriarca PA. Vaccination levels and missed opportunities for measles vaccination: a record audit in a public pediatric clinic. Pediatrics 1992;89:589--92.
- CDC. Syncope after vaccination---United States, January 2005--July 2007. MMWR 2008;57:457--60.
- Liebermann P. Anaphylaxis and anaphylactoid reactions. In: Middleton's allergy: principles and practice. Adkinson NF, Yunginger JW, Busse LW, Bochner BS, Holgate ST, Simons FE, eds. 6th ed. Philadelphia, PA: Mosby; 2003.
- Nakayama T, Aizawa C, Kuno-Sakai H. A clinical analysis of gelatin allergy and determination of its causal relationship to the previous administration of gelatin-containing acellular pertussis vaccine combined with diphtheria and tetanus toxoids. J Allergy Clin Immunol 1999;103:321--5.
- Brotherton JM, Gold MS, Kemp AS et al. Anaphylaxis following quadrivalent human papillomavirus vaccination. CMAJ 2008;179: 525--33.
- Ruggeberg JU, Gold MS, Bayas J, et al. Anaphylaxis: case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2007;25:5675-5684.
- Sampson HA, Munoz-Furlong A, Bock SA, et al. Symposium on the definition and management of anaphylaxis : summary report. J Allergy Clin Immunol 2005;115:584--91.
- Mosby's Drug Consult. 16th ed. Elsevier St Louis, MO; 2003. [Epinephrine.]
- CDC. Update: vaccine side effects, adverse reactions, contraindications, and precautions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1996;45(No. RR-12).
- CDC. Guideline for hand hygiene in health-care settings: recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. MMWR 2002;51(No. RR-16).
- Occupational Safety and Health Administration. Occupational exposure to bloodborne pathogens; needlesticks and other sharps injuries; final rule (29 CFR Part 1910). Federal Register January 18, 2001;66:5318--25. Available at http://www.osha.gov/FedReg_osha_pdf/FED20010118A.pdf.
- Drucker E, Alcabes PG, Marx PA. The injection century: massive unsterile injections and the emergence of human pathogens. Lancet 2001;358:1989--92.
- International Health Care Worker Safety Center. List of safety-engineered sharp devices and other products designed to prevent occupational exposures to bloodborne pathogens. Charlottesville, VA: University of Virginia; 2001. Available at http://www.healthsystem.virginia.edu/internet/epinet/safetydevice.cfm.
- National Alliance for the Primary Prevention of Sharps Injuries. NAPPSI: National Alliance for the Primary Prevention of Sharps Injuries. Carlsbad, CA: NAPPSI; 2001. Available at http://www.nappsi.org.
- Shaw FE Jr, Guess HA, Roets JM, et al. Effect of anatomic injection site, age and smoking on the immune response to hepatitis B vaccination. Vaccine 1989;7:425--30.
- Zuckerman JN. Importance of injecting vaccines into muscle: different patients need different needle sizes. Brit Med J 2000;321:1237--8.
- Ipp MM, Gold R, Goldback M, et al. Adverse reactions to diphtheria, tetanus, pertussis-polio vaccination at 18 months of age: effect of injection site and needle length. Pediatrics 1989;83:679--82.
- Michaels L, Poole RW. Injection granuloma of the buttock. Can Med Assoc J 1970;102:626--8.
- Haramati N, Lorans R, Lutwin M, Kaleya RN. Injection granulomas: intramuscle or intrafat? Arch Fam Med 1994;3:146--8.
- Bergeson PS, Singer SA, Kaplan AM. Intramuscular injections in children. Pediatrics 1982;70:944--8.
- Poland GA, Borrund A, Jacobson RM, et al. Determination of deltoid fat pad thickness: implications for needle length in adult immunization. JAMA 1997;277:1709--11.
- Groswasser J, Kahn A, Bouche B, Hanquinet S, Perlmuter N, Hessel L. Needle length and injection technique for efficient intramuscular vaccine delivery in infants and children evaluated through an ultrasonographic determination of subcutaneous and muscle layer thickness. Pediatrics 1997;100:400--3.
- Ipp M, Taddio A, Sam J, et al. Vaccine-related pain: randomized controlled trial of two injection techniques. Arch Dis Child 2007;92:1105--8.
- Middleman AB, Anding R, Tung C. Effect of needle length when immunizing obese adolescents with Hepatitis B vaccine. Pediatrics 2010;125:e1--e5.
- Scheifele D, Bjornson G, Barreto L, Meekison W, Guasparini R. Controlled trial of Haemophilus influenzae type b diphtheria toxoid conjugate combined with diphtheria, tetanus and pertussis vaccines, in 18-month-old children, including comparison of arm versus thigh injection. Vaccine 1992;10:455--60.
- Hingson RA, Davis HS, Rosen M. Historical development of jet injection and envisioned uses in mass immunization and mass therapy based upon two decades' experience. Mil Med 1963;128:516--24.
- Weniger BG, Papania MJ. Alternative vaccine delivery methods [Chapter 61]. In: Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines, 5th ed. China: Saunders/Elsevier;2008;135
- Simonsen L, Kane A, Lloyd J, Zaffran M, Kane M. Unsafe injections in the developing world and transmission of bloodborne pathogens: a review. Bull World Health Organ 1999;77:789--800.
- Kane A, Lloyd J, Zaffran M, Simonsen L, Kane M. Transmission of hepatitis B, hepatitis C and human immunodeficiency viruses through unsafe injections in the developing world: model-based regional estimates. Bull World Health Organ 1999;77:801--7.
- CDC. Hepatitis B associated with jet gun injection---California. MMWR 1986;35:373--6.
- Canter J, Mackey K, Good LS, et al. Outbreak of hepatitis B associated with jet injections in a weight reduction clinic. Arch Intern Med 1990;150:1923--7.
- Hoffman PN, Abuknesha RA, Andrews NJ, Samuel D, Lloyd JS. Model to assess the infection potential of jet injectors used in mass immunization. Vaccine 2001;19:4020--7.
- Kelly K, Loskutov A, Zehrung D, et al. Preventing contamination between injections with multiple-use nozzle needle-free injectors: A safety trial. Vaccine 2008;26:1344--52.
- Gray L, Watt L, Blass EM. Skin-to-skin contact is analgesic in healthy newborns. Pediatrics 2000;105:1--6.
- Gray L, Miller LW, Philipp BL, Blass EM. Breastfeeding is analgesic in healthy newborns. Pediatrics 2002;109:590--3.
- Taddio A, Nulman I, Goldbach M, Ipp M, Koren G. Use of lidocaine-prilocaine cream for vaccination pain in infants. J Pediatr 1994;124:643--8.
- Uhari M. Eutectic mixture of lidocaine and prolocaine for alleviating vaccination pain in infants. Pediatrics 1993;92:719--21.
- Halperin SA, McGrath P, Smith B, Houston T. Lidocaine-prilocaine patch decreases the pain associated with subcutaneous administration of measles-mumps-rubella vaccine but does not adversely affect the antibody response. J Pediatr 2000;136:789--94.
- Frayling IM, Addison GM, Chatterge K, Meakin G. Methaemoglobinaemia in children treated with prilocaine-lignocaine cream. Brit Med J 1990;301:153--4.
- Reis E, Holubkov R. Vapocoolant spray is equally effective as EMLA cream in reducing immunization pain in school-aged children. Pediatrics 1997;100:1--6.
- American Academy of Pediatrics: Steering Committee on Quality Improvement and Management, Subcommittee on Febrile Seizures. Febrile seizures: clinical practice guideline for the long-term management of the child with simple febrile seizures. Pediatrics. 2008;121:1281--6.
- Cook IF, Murtagh J. Comparative immunogenicity of hepatitis B vaccine administered into the ventrogluteal area and anterolateral thigh in infants. J Paediatr Child Health 2002:38;393--6.
- Redfield RR, Innis BL, Scott RM, Cannon HG, Bancroft WH. Clinical evaluation of low-dose intradermally administered hepatitis B vaccine: a cost reduction strategy. JAMA 1985;254:3203--6.
- Coleman PJ, Shaw FE, Serovich J, Hadler SC, Margolis HS. Intradermal hepatitis B vaccination in a large hospital employee population. Vaccine 1991;9:723--7.
- Fishbein DB, Sawyer LA, Reid-Sanden FL, Weir EH. Administration of human diploid-cell rabies vaccine in the gluteal area [Letter]. N Eng J Med 1988;318:124--5.
- CDC. Inadvertent misadministration of meningococcal conjugate vaccine---United States, June--August 2005. MMWR 2006;55:101--7.
- Belshe BB, Newman FK, Cannon J, et al. Serum antibody responses after intradermal vaccination against influenza. N Engl J Med 2004;351:2286--94.
- CDC. Guidelines for maintaining and managing the vaccine cold chain. MMWR 2003;52:1023--5.
- Langley A, Grant S, ed. Proceedings of the National Vaccine Storage Workshop; June 28--30, 2004; Brisbane, Australia. Maroochydore: Queensland Health; 2004.
- Department of Health and Ageing. National vaccine storage guidelines: Strive for 5. Canberra: Commonwealth of Australia; 2005.
- Atkinson WL, Kroger AT, Pickering LK. General immunization practices. In: Vaccines. Plotkin SA, Orenstein WA, Offit PA. eds. 5th ed. China: Saunders/Elsevier; 2008.
- Algood HM, Lin PL, Flynn JL. Tumor necrosis factor and chemokine interactions in the formation and maintenance of granulomas in tuberculosis. Clin Infect Dis 2005;41:189--93.
- Ehlers S. Tumor necrosis factor and its blockade in granulomatous infections: differential modes of action of infliximab and etanercept. Clin Infect Dis 2005;41:199--203.
- Deepe GS, Smelt S, Louie JS. Tumor necrosis factor inhibition and opportunistic infections. Clin Infect Dis 2005;41:187--8.
- Filler SG, Yeaman MR, Sheppard DC. Tumor necrosis factor inhibition and invasive fungal infections. Clin Infect Dis 2005;41:208--12.
- Moore TA, Lau HY, Cogen AL, Standiford TJ. Defective innate antibacterial host responses during murine Klebsiella pneumoniae bacteremia: tumor necrosis factor (TNF) receptor 1 deficiency versus therapy with anti-TNF. Clin Infect Dis 2005;41:213--7.
- CDC. Tuberculosis associated with blocking agents against tumor necrosis factor-alpha---California, 2002--2003. MMWR 2004;53:683--6.
- Markert ML, Hummell DS, Rosenblatt HM, et al. Complete DiGeorge syndrome: persistence of profound immunodeficiency. J Pediatr 1998;132:15--21.
- Anonymous. 110 Warning signs of primary immunodeficiency [Poster]. New York, NY: Jeffrey Modell Foundation Medical Advisory Board; 2004.
- Grossberg R, Harpaz R, Rubtcova E, Loparev V, Seward JF, Schmid DS. Secondary transmission of varicella vaccine virus in a chronic care facility for children. J Pediatr 2006;148:842--4.
- CDC. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2009;58(No. RR-2).
- Sixbey JW. Routine immunization of the immunocompromised child. Adv Pediatr Infect Dis 1987;2:79--114.
- Wright PF, Hatch MH, Kasselberg AG, Lowry SP, Wadlington WB, Karzon DT. Vaccine-associated poliomyelitis in a child with sex-linked agammaglobulinemia. J Pediatr 1977;91:408--12.
- Wyatt HV. Poliomyelitis in hypogammaglobulinemics. J Infect Dis 1973;128:802--6.
- Davis LE, Bodian D, Price D, Butler IJ, Vickers JH. Chronic progressive poliomyelitis secondary to vaccination of an immunodeficient child. N Engl J Med 1977;297:241--5.
- CDC. Disseminated Mycobacterium bovis infection from BCG vaccination of a patient with acquired immunodeficiency syndrome. MMWR 1985;34:227--8.
- Ninane J, Grymonprez A, Burtonboy G, Francois A, Cornu G. Disseminated BCG in HIV infection. Arch Dis Child 1988;63:1268--9.
- Redfield RR, Wright DC, James WD, Jones TS, Brown C, Burke DS. Disseminated vaccinia in a military recruit with human immunodeficiency virus (HIV) disease. N Engl J Med 1987;316:673--6.
- CDC. Measles pneumonitis following measles-mumps-rubella vaccination of a patient with HIV infection, 1993. MMWR 1996;45:603--6.
- Derryck A, LaRussa P, Steinberg S, Capasso M, Pitt J, Gershon AA. Varicella and zoster infection in children with human immunodeficiency virus infection. Pediatr Infect Dis J 1998;17:931--3.
- CDC. Guidelines for the Prevention and Treatment of Opportunistic Infections Among HIV-exposed and HIV-infected children: recommendations from CDC, the National Institutes of Health, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics. MMWR 2009;58(No. RR-11).
- Levin MJ, Gershon AA, Weinberg A, et al. Immunization of HIV-infected children with varicella vaccine. J Pediatr 2001;139:305--10.
- Sprauer MA, Markowitz LE, Nicholson JKA, et al. Response of human immunodeficiency virus-infected adults to measles-rubella vaccination. J Acquir Immune Defic Syndr 1993;6:1013--6.
- McLaughlin M, Thomas P, Onorato I, et al. Live virus vaccines in human immunodeficiency virus-infected children: a retrospective survey. Pediatrics 1988;82:229--33.
- Onorato IM, Markowitz LE, Oxtoby MJ. Childhood immunization, vaccine-preventable diseases and infection with human immunodeficiency virus. Pediatr Infect Dis J 1988;6:588--95.
- Palumbo P, Hoyt L, Demasio K, Oleske J, Connor E. Population-based study of measles and measles immunization in human immunodeficiency virus-infected children. Pediatr Infect Dis J 1992;11:1008--14.
- Tomblyn M, Chiller T, Einsele et al. Guidelines for preventing infectious complications among hematopoietic cell transplant recipients: a global perspective. Biol Blood Marrow Transplant 15:1143--1238; 2009.
- Ljungman P, Cordonnier C, Einsele H, et al. Vaccination of hematopoietic cell transplant recipients. Bone Marrow Transplant 2009;44:521--6.
- American Academy of Pediatrics. Immunization in special clinical circumstances. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS. eds. Red Book: 2009 Report of the Committee on Infectious Diseases. 28th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2009.
- Brodtman DH, Rosenthal DW, Redner A, Lanzkowsky P, Bonagura VR. Immunodeficiency in children with acute lymphoblastic leukemia after completion of modern aggressive chemotherapeutic regimens. J Pediatr 2005;146:654--61.
- Starr S, Berkovich S. Effects of measles, gamma-globulin-modified measles and vaccine measles on the tuberculin test. N Engl J Med 1964;270:386--91.
- Brickman HF, Beaudry PH, Marks MI. Timing of tuberculin tests in relation to immunization with live viral vaccines. Pediatrics 1975;55:392--6.
- Berkovich S, Starr S. Effects of live type 1 poliovirus vaccine and other viruses on the tuberculin test. N Engl J Med 1966;274:67--72.
- CDC. Recommendations for using smallpox vaccine in a pre-event vaccination program: supplemental recommendations of the Advisory Committee on Immunization Practices (ACIP) and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR 2003;52(No. RR-7).
- CDC. Updated guidelines for using interferon gamma release assays to detect Mycobacterium tuberculosis infection---United States, 2010. MMWR 2010;59(No. RR-5).
- Grabenstein JD. Clinical management of hypersensitivities to vaccine components. Hospital Pharmacy 1997;32:77--87.
- Grabenstein JD. ImmunoFacts: vaccines & immunologic drugs. St. Louis, MO: Wolters Kluwer;Facts & Comparisons; 2010.
- Kelso JM. Administration of influenza vaccine to patients with egg allergy. J Allergy Clin Immunol 2010;125:800--2.
- Wood RA, Berger M, Dreskin SC, et al. An algorithm for treatment of patients with hypersensitivity reactions after vaccines. Pediatrics. 2008;122:e771--e7.
- Kelso JM, Jones RT, Yunginger JW. Anaphylaxis to measles, mumps, and rubella vaccine mediated by IgE to gelatin. J Allergy Clin Immunol 1993;91:867--72.
- Sakaguchi M, Ogura H, Inouye S. IgE antibody to gelatin in children with immediate-type reactions to measles and mumps vaccines. J Allergy Clin Immunol 1995;96:563--5.
- Sakaguchi M, Yamanaka T, Ikeda K, et al. IgE-mediated systemic reactions to gelatin included in the varicella vaccine. J Allergy Clin Immunol 1997;99:263--4.
- Sakaguchi M, Nakayama T, Inouye S. Food allergy to gelatin in children with systemic immediate-type reactions, including anaphylaxis, to vaccines. J Allergy Clin Immunol 1996;98:1058--61.
- Reitschel RL, Bernier R. Neomycin sensitivity and the MMR vaccine [Letter]. JAMA 1981;245:571.
- Elliman D, Dhanraj B. Safe MMR vaccination despite neomycin allergy [Letter]. Lancet 1991;337:365.
- Aberer W. Vaccination despite thimerosal sensitivity. Contact Dermatitis 1991;24:6--10.
- Kirkland LR. Ocular sensitivity to thimerosal: a problem with hepatitis B vaccine? South Med J 1990;83:497--9.
- Cox NH, Forsyth A. Thiomersal allergy and vaccination reactions. Contact Dermatitis 1988;18:229--33.
- Möller H. All these positive tests to thimerosal. Contact Dermatitis 1994;31:209--13.
- Wantke F, Demmer CM, Götz M, Jarisch R. Contact dermatitis from thimerosal: 2 year's experience with ethylmercuric chloride in patch testing thimerosal-sensitive patients. Contact Dermatitis 1994;30:115--8.
- Slater JE. Latex allergy. J Allergy Clin Immunol 1994;94:139--49.
- Towse A, O'Brien M, Twarog FJ, Braimon J, Moses A. Local reaction secondary to insulin injection: a potential role for latex antigens in insulin vials and syringes. Diabetes Care 1995;18:1195--7.
- Bastyr EJ. Latex allergen allergic reactions [Letter]. Diabetes Care 1996;19:546.
- MacCracken J, Stenger P, Jackson T. Latex allergy in diabetic patients: a call for latex-free insulin tops [Letter]. Diabetes Care 1996;19:184.
- Russell M, Pool V, Kelso J, Tomazic-Jezic V. Vaccination of persons allergic to latex: a review of safety data in the Vaccine Adverse Event Reporting System (VAERS). Vaccine 2004;23:664--7.
- Bernbaum JC, Daft A, Anolik R, et al. Response of preterm infants to diphtheria-tetanus-pertussis immunizations. J Pediatr 1985;107:184--8.
- Koblin BA, Townsend TR, Munoz A, Onorato I, Wilson M, Polk BF. Response of preterm infants to diphtheria-tetanus-pertussis vaccine. Pediatr Infect Dis J 1988;7:704--11.
- Smolen P, Bland R, Heiligenstein E, et al. Antibody response to oral polio vaccine in premature infants. J Pediatr 1983;103:917--9.
- Omenaca F, Garcia-Sicilia J, Garcia-Corbeira P, et al. Response of preterm newborns to immunization with a hexavalent diphtheria-tetanus-acellular pertussis-hepatitis B virus-inactivated polio and Haemophilus influenzae type b vaccine: first experiences and solutions to a serious and sensitive issue. Pediatrics 2005;116:1292--8.
- Shinefield H, Black S, Ray P, Fireman B, Schwalee M, Lewis E. Efficacy, immunogenicity and safety of heptavalent pneumococcal conjugate vaccine in low birthweight preterm infants. Ped Inf Dis J 2002;21:182--6.
- Lau YL, Tam AY, Ng KW, et al. Response of preterm infants to hepatitis B vaccine. J Pediatr 1992;121:962--5.
- Patel DM, Butler J, Feldman S, Graves GR, Rhodes PG. Immunogenicity of hepatitis B vaccine in healthy very low birth weight infants. J Pediatr 1997;131:641--3.
- Kim SC, Chung EK, Hodinka RL, et al. Immunogenicity of hepatitis B vaccine in preterm infants. Pediatrics 1997;99:534--6.
- Losonsky GA, Wasserman SS, Stephens I, et al. Hepatitis B vaccination of premature infants: a reassessment of current recommendations for delayed immunization. Pediatrics 1999;103:14.
- Bohlke K, Galil K, Jackson LA, et al. Postpartum varicella vaccination: is the vaccine virus excreted in breast milk? Obstet Gynecol 2003;102:970--7.
- Krogh V, Duffy LC, Wong D, Rosenband M, Riddlesberger KR, Ogra PL. Postpartum immunization with rubella virus vaccine and antibody response in breast-feeding infants. J Lab Clin Med 1989;113:695--9.
- Pickering LK, Granoff DM, Erickson JR, et al. Modulation of the immune system by human milk and infant formula containing nucleotides. Pediatrics 1998;101:242--9.
- Kim-Farley R, Brink E, Orenstein W, Bart K. Vaccination and breast feeding [Letter]. JAMA 1982;248:2451--2.
- Patriarca PA, Wright PF, John TJ. Factors affecting the immunogenicity of oral polio vaccine in developing countries: review. Rev Infect Dis 1991;13:926--39.
- Hahn-Zoric M, Fulconis F, Minoli I, et al. Antibody responses to parenteral and oral vaccines are impaired by conventional and low-protein formulas as compared to breast feeding. Acta Paediatr Scand 1990;79:1137--42.
- Koren G, Pastuszak A, Ito S. Drugs in pregnancy. N Engl J Med 1998;338:1128--37.
- Grabenstein JD. Vaccines and antibodies in relation to pregnancy and lactation. Hospital Pharmacy 1999;34:949--60.
- CDC. Guiding principles for development of ACIP recommendations for vaccinating during pregnancy and breastfeeding. MMWR 2008;57:580.
- CDC. Prevention of pertussis, tetanus, and diphtheria among pregnant and postpartum women and their infants: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2008;57(No. RR-4).
- Neuzil KM, Reed GW, Mitchel EF, Simonsen L, Griffin MR. Impact of influenza on acute cardiopulmonary hospitalizations in pregnant women. Am J Epidemiol 1998;148:1094--102.
- CDC. Poliomyelitis prevention in the United States: updated recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2000;49(No. RR-5).
- CDC. Prevention of hepatitis A through active or passive immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2006;55(No. RR-7).
- Tsai TF, Paul R, Lynberg MC, Letson GW. Congenital yellow fever virus infection after immunization in pregnancy. J Infect Dis 1993;168:1520--3.
- CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP) part II: immunization of adults. MMWR 2006; 55(No. RR-16)[1-33].
- Wilson E, Goss MA, Marin M, et al. Varicella vaccine exposure during pregnancy: data from 10 years of the pregnancy registry. J Infect Dis 2008;197 (Suppl 2):S178--84.
- CDC. Revised ACIP recommendation for avoiding pregnancy after receiving a rubella-containing vaccine. MMWR 2001;50:1117.
- CDC. Rubella vaccination during pregnancy---United States, 1971--1988. MMWR 1989;38:289--93.
- Murray TS, Groth E, Weitzman C, Cappello M. Epidemiology and management of infectious diseases in international adoptees. Clin Microbiol Rev 2005;18:510--20.
- Hostetter MK. Infectious diseases in internationally adopted children: findings in children from China, Russia, and Eastern Europe. Adv Pediatr Infect Dis 1999;14:147--61.
- Kriz B, Burian V, Sladky K, et al. Comparison of titration results of diphtheric antitoxic antibody obtained by means of Jensen's method and the method of tissue cultures and haemagglutination. J Hyg Epidemiol Microbiol Immunol 1978;22:485--93.
- CDC. Updated recommendations from the Advisory Committee on Immunization Practices (ACIP) for use of hepatitis A vaccine in close contacts of newly arriving international adoptees. MMWR 2009;58.
- CDC. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR 2008;57(No. RR-8).
- Evans DI, Shaw A. Safety of intramuscular injection of hepatitis B vaccine in haemophiliacs. BMJ 1990;300:1694--5.
- CDC. Immunization information system progress---United States, 2006. MMWR 2008;57:289--91.
- US Department of Health and Human Services, Health Care Financing Administration; DeParle N, ed. A profile of Medicaid: chartbook 2000. Washington, DC: Health Care Financing Administration. Available at http://www.cms.hhs.gov/thechartseries. Accessed December 13, 2010.
- US Department of Health and Human Services. Immunization and infectious diseases. In: Healthy people 2010 (conference ed., vol. 1). Washington, DC: US Government Printing Office; 2000.
- Mangione-Smith R, DeChristofaro A, Setodji C, et al. The quality of ambulatory care delivered to children in the United States. NEJM 2007; 375:1515--23.
- Roush SW, Murphy TV. Historical comparisons of morbidity and mortality for vaccine-preventable diseases in the United States. JAMA 2007;298:2155--63.
- CDC. Recommendations of the Advisory Committee on Immunization Practices (ACIP). Notice to readers: Programmatic strategies to increase vaccination coverage by age 2 years---linkage of vaccination and WIC services. MMWR 1996;45:217--8.
- Hagan JF, Shaw JS, Duncan PM, eds. Bright futures: guidelines for health supervision on infants, children and adolescents. 3rd ed. Elk Grove Village, IL: American Academy of Pediatrics; 2008.
- CDC. Immunization of adolescents: recommendations of the Advisory Committee on Immunization Practices (ACIP), the American Academy of Pediatrics (AAP), the American Academy of Family Physicians (AAFP), and the American Medical Association (AMA). MMWR 1996;45(No. RR-13).
- Poland GA, Shefer AM, McCauley M, et al. Standards for adult immunization practices. Am J Prev Med 2003;25:144--50.
- Maciosek MV, Coffield AB, Edwards NM, et al. Priorities among effective clinical preventive services: results of a systematic review and analysis. Am J Prev Med. 2006;31:52--61.
- Riddiough MA, Sisk JE, Bell JC. Influenza Vaccination. JAMA 1983;249:3189--95.
- Nichol KL. Cost-benefit analysis of a strategy to vaccinate healthy working adults against influenza. Arch Intern Med 2001;161: 749--59.
- Nichol KL, Mallon KP, Mendelman PM. Cost benefit of influenza vaccination in healthy, working adults: an economic analysis based on the results of a clinical trial of trivalent live attenuated influenza virus vaccine. Vaccine 2003;21:2207--17.
- Bridges CB, Thompson WW, Meltzer MI, et al. Effectiveness and cost-benefit of influenza vaccination of healthy working adults: a randomized controlled trial. JAMA 2000;284:1655--63.
- Smith KJ, Zimmerman RK, Lin CJ, et al. Alternative strategies for adult pneumococcal polysaccharide vaccination: a cost-effectiveness analysis. Vaccine 2008; 26:1420--31.
- Pisu M, Meltzer MI, Lyerla R. Cost-effectiveness of hepatitis B vaccination of prison inmates. Vaccine 2002;21:312--21.
- Rich JD, Ching CG, Lally MA, et al. A review of the case for hepatitis B vaccination of high-risk adults. Am J Med 2003; 114:316--8.
- Pellissier JM, Brisson M, Levin MJ. Evaluation of the cost-effectiveness in the United States of a vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. Vaccine 2007;25:8326--37.
- Insinga RP, Itzler RF, Pellissier JM, Saddier P, Nikas AA. The incidence of herpes zoster in a United States administrative database. J Gen Intern Med 2005;20:748--53.
- Rothberg MB, Virapongse A, Smith KJ. Cost-effectiveness of a vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. Clin Infect Dis 2007; 44:1280--8.
- Hornberger J, Robertus K. Cost-effectiveness of a vaccine to herpes zoster and postherpetic neuralgia in older adults. Ann Intern Med 2006;145:317-25.
- Shefer A, Briss P, Rodewald L, et al. Improving immunization coverage rates: an evidence-based review of the literature. Epidemiol Rev 1999;21:96--142.
- CDC. Vaccine-preventable diseases: improving vaccination coverage in children, adolescents, and adults; a report on recommendations of the Task Force on Community Preventive Services. MMWR 1999;48(No. RR-8).
- Briss PA, Rodewald LE, Hinman AR, et al. Reviews of evidence regarding interventions to improve vaccination coverage in children, adolescents, and adults. Am J Prev Med 2000;18:97--140.
- Task Force on Community Preventive Services. Recommendations regarding interventions to improve vaccination coverage in children, adolescents, and adults. Am J Prev Med 2000;18:92--6.
- Ndiaye SM, Hopkins DP, Shefer AM, et al. Interventions to improve influenza, pneumococcal polysaccharide, and hepatitis B vaccination coverage among high-risk adults: a systematic review. Am J Prev Med. 2005;28(Suppl 5):248--79.
* During measles outbreaks, if cases are occurring among infants aged <12 months, measles vaccination of infants as young as 6 months can be used as an outbreak control measure. However, doses administered at ages <12 months should not be counted as part of the series (Source: CDC. Measles, mumps, and rubella vaccine use and strategies for elimination of measles, rubella, and congenital rubella syndrome and control of mumps: recommendations of the Advisory Committee on Immunization Practices [ACIP]. MMWR 1998;47[No. RR-8]).
† In certain situations, local or state requirements might mandate that doses of selected vaccines be administered on or after specific ages. For example, a school entry requirement might not accept a dose of MMR or varicella vaccine administered before the child's first birthday. ACIP recommends that physicians and other health-care providers comply with local or state vaccination requirements when scheduling and administering vaccines.
§ Provider assessment should include number of injections, vaccine availability, likelihood of improved coverage, likelihood of patient return, and storage and cost considerations.
¶ The exception is the 2-dose hepatitis B vaccination series for adolescents aged 11--15 years. Only Recombivax HB (Merck Vaccine Division) should be used in this schedule. Engerix-B (GlaxoSmithKline) is not approved by FDA for this schedule.
** Based on expert opinion.
†† National Childhood Vaccine Injury Act of 1986. 42 U.S.C. Sect. 300aa-26 (1986).
§§ If the gluteal muscle is chosen, injection should be administered lateral and superior to a line between the posterior superior iliac spine and the greater trochanter or in the ventrogluteal site, the center of a triangle bounded by the anterior superior iliac spine, the tubercle of the iliac crest, and the upper border of the greater trochanter.
¶¶ Enzyme immunoassay tests are available. Physicians should contact the laboratory performing the test for interpretive standards and limitations. Protective concentrations for antibody to diphtheria and tetanus toxins are defined as >0.1 IU/mL.
Abbreviations
AAFP -- American Academy of Family Physicians
AAP -- American Academy of Pediatrics
ACIP -- Advisory Committee on Immunization Practices
DT -- pediatric diphtheria-tetanus toxoid
DTaP -- pediatric diphtheria and tetanus toxoids and acellular pertussis
FDA -- Food and Drug Administration
GBS -- Guillain-Barré syndrome
HBIG -- hepatitis B immune globulin
HBsAg -- hepatitis B surface antigen
Hib -- Haemophilus influenzae type b
HIV -- human immunodeficiency virus
HPV -- human papillomavirus
HCT -- hematopoietic cell transplant
IgG -- immunoglobulin G
IGIV -- intravenous immune globulin
IPV -- inactivated poliovirus
LAIV -- live, attenuated influenza vaccine
MCV4 -- quadrivalent meningococcal conjugate vaccine
MMR -- measles, mumps, and rubella
MMRV -- measles, mumps, rubella, and varicella
MPSV4 -- quadrivalent meningococcal polysaccharide vaccine
OPV -- oral poliovirus
OSHA -- Occupational Safety and Health Administration
PCV -- pneumococcal conjugate vaccine
PRP-OMP -- Haemophilus influenzae type b-polyribosylribitol phosphate-meningococcal outer membrane protein conjugate
PPSV -- pneumococcal polysaccharide vaccine
RV1 -- live, attenuated monovalent rotavirus vaccine
RV5 -- live, reassortant pentavalent rotavirus vaccine
Td -- adult tetanus and diphtheria toxoids
Tdap -- tetanus and reduced diphtheria toxoids and acellular pertussis (for adolescents and adults)
TIV -- trivalent inactivated influenza vaccine
TST -- tuberculin skin test
VAERS -- Vaccine Adverse Event Reporting System
VIS -- vaccine information statement
ZOS -- herpes zoster vaccine
Glossary
Adverse event. An untoward event that occurs after a vaccination that might be caused by the vaccine product or vaccination process. Adverse events include those that have the following characteristics: 1) vaccine induced (caused by the intrinsic characteristic of the vaccine preparation and the individual response of the vaccinee): these events would not have occurred without vaccination (e.g., vaccine-associated paralytic poliomyelitis); 2) vaccine potentiated: the events would have occurred anyway but were precipitated by the vaccination (e.g., first febrile seizure in a predisposed child); 3) programmatic error: the event was caused by technical errors in vaccine preparation, handling, or administration; and 4) coincidental: the event was associated temporally with vaccination by chance or caused by underlying illness. Special studies are needed to determine whether an adverse event is a reaction to the vaccine or the result of another cause (Sources: Chen RT. Special methodological issues in pharmacoepidemiology studies of vaccine safety. In: Strom BL, ed. Pharmacoepidemiology. 3rd ed. Sussex, England: John Wiley & Sons; 2000:707--32; and Fenichel GM, Lane DA, Livengood JR, Horwitz SJ, Menkes JH, Schwartz JF. Adverse events following immunization: assessing probability of causation. Pediatr Neurol 1989;5:287--90).
Adverse reaction. An undesirable medical condition that has been demonstrated to be caused by a vaccine. Evidence for the causal relation is usually obtained through randomized clinical trials, controlled epidemiologic studies, isolation of the vaccine strain from the pathogenic site, or recurrence of the condition with repeated vaccination (i.e., rechallenge); synonyms include side effect and adverse effect.
Adjuvant. A vaccine component distinct from the antigen that enhances the immune reponse to the antigen.
Antitoxin. A solution of antibodies against a toxin. Antitoxin can be derived from either human (e.g., tetanus immune globulin) or animal (usually equine) sources (e.g., diphtheria and botulism antitoxin). Antitoxins are used to confer passive immunity and for treatment.
Hyperimmune globulin (specific). Special preparations obtained from blood plasma from donor pools preselected for a high antibody content against a specific antigen (e.g., hepatitis B immune globulin, varicella-zoster immune globulin, rabies immune globulin, tetanus immune globulin, vaccinia immune globulin, cytomegalovirus immune globulin, botulism immune globulin).
Immune globulin. A sterile solution containing antibodies, which are usually obtained from human blood. It is obtained by cold ethanol fractionation of large pools of blood plasma and contains 15%--18% protein. Intended for intramuscular administration, immune globulin is primarily indicated for routine maintenance of immunity among certain immunodeficient persons and for passive protection against measles and hepatitis A.
Immunobiologic. Antigenic substances (e.g., vaccines and toxoids) or antibody-containing preparations (e.g., globulins and antitoxins) from human or animal donors. These products are used for active or passive immunization or therapy. Examples of immunobiologics include antitoxin, immune globulin and hyperimmune globulin, monoclonal antibodies, toxoids, and vaccines.
Intravenous immune globulin. A product derived from blood plasma from a donor pool similar to the immune globulin pool, but prepared so that it is suitable for intravenous use. Intravenous immune globulin is used primarily for replacement therapy in primary antibody-deficiency disorders, for treatment of Kawasaki disease, immune thrombocytopenic purpura, hypogammaglobulinemia in chronic lymphocytic leukemia, and certain cases of human immunodeficiency virus infection (Table 5).
Monoclonal antibody. An antibody product prepared from a single lymphocyte clone, which contains only antibody against a single antigen.
Simultaneous. In the context of vaccine timing and spacing, occurring on the same clinic day, at different anatomic sites, and not combined in the same syringe.
Toxoid. A modified bacterial toxin that has been made nontoxic, but retains the ability to stimulate the formation of antibodies to the toxin.
Vaccination and immunization. The terms vaccine and vaccination are derived from vacca, the Latin term for cow. Vaccine was the term used by Edward Jenner to describe material used (i.e., cowpox virus) to produce immunity to smallpox. The term vaccination was used by Louis Pasteur in the 19th century to include the physical act of administering any vaccine or toxoid. Immunization is a more inclusive term, denoting the process of inducing or providing immunity by administering an immunobiologic. Immunization can be active or passive. Active immunization is the production of antibody or other immune responses through administration of a vaccine or toxoid. Passive immunization means the provision of temporary immunity by the administration of preformed antibodies. Although persons often use the terms vaccination and immunization interchangeably in reference to active immunization, the terms are not synonymous because the administration of an immunobiologic cannot be equated automatically with development of adequate immunity.
Vaccine. A suspension of live (usually attenuated) or inactivated microorganisms (e.g., bacteria or viruses) or fractions thereof administered to induce immunity and prevent infectious disease or its sequelae. Some vaccines contain highly defined antigens (e.g., the polysaccharide of Haemophilus influenzae type b or the surface antigen of hepatitis B); others have antigens that are complex or incompletely defined (e.g., Bordetella pertussis antigens or live, attenuated viruses).
|
TABLE 1. (Continued) Recommended and minimum ages and intervals between vaccine doses*,† |
|---|
|
Abbreviations: DTaP = diphtheria and tetanus toxoids and acellular pertussis; HepA = hepatitis A; HepB = hepatitis B; Hib = Haemophilus influenzae type b; HPV = human papillomavirus; IPV = inactivated poliovirus; LAIV = live, attenuated influenza vaccine; MCV4 = quadrivalent meningococcal conjugate vaccine; MMR = measles, mumps, and rubella; MMRV = measles, mumps, rubella, and varicella; MPSV4 = quadrivalent meningococcal polysaccharide vaccine; PCV = pneumococcal conjugate vaccine; PPSV = pneumococcal polysaccharide vaccine; PRP-OMB = polyribosylribitol phosphate-meningococcal outer membrane protein conjugate; Td = tetanus and diphtheria toxoids; TIV = trivalent inactiated influenza vaccine; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis; Var = varicella vaccine. * Combination vaccines are available. Use of licensed combination vaccines is generally preferred to separate injections of their equivalent component vaccines. When administering combination vaccines, the minimum age for administration is the oldest age for any of the individual components; the minimum interval between doses is equal to the greatest interval of any of the individual components. † Information on travel vaccines, including typhoid, Japanese encephalitis, and yellow fever, is available at http://www.cdc.gov/travel. Information on other vaccines that are licensed in the United States but not distributed, including anthrax and smallpox, is available at http://www.bt.cdc.gov. § Combination vaccines containing the hepatitis B component are available (see Table 2). These vaccines should not be administered to infants aged <6 weeks because of the other components (i.e., Hib, DTaP, HepA, and IPV). ¶ HepB-3 should be administered at least 8 weeks after HepB-2 and at least 16 weeks after HepB-1 and should not be administered before age 24 weeks. ** Calendar months. †† The minimum recommended interval between DTaP-3 and DTaP-4 is 6 months. However, DTaP-4 need not be repeated if administered at least 4 months after DTaP-3. §§ For Hib and PCV, children receiving the first dose of vaccine at age ≥7 months require fewer doses to complete the series. ¶¶ If PRP-OMP (Pedvax-Hib, Merck Vaccine Division) was administered at ages 2 and 4 months, a dose at age 6 months is not necessary. *** A fourth dose is not needed if the third dose was administered at ≥4 years and at least 6 months after the previous dose. ††† Combination MMRV vaccine can be used for children aged 12 months--12 years. See text for details. §§§ The minimum interval from Varicella-1 to Varicella-2 for persons beginning the series at age ≥13 years is 4 weeks. ¶¶¶ One dose of influenza vaccine per season is recommended for most persons. Children aged <9 years who are receiving influenza vaccine for the first time or who received only 1 dose the previous season (if it was their first vaccination season) should receive 2 doses this season. **** The minimum age for inactivated influenza vaccine varies by vaccine manufacturer. See package insert for vaccine-specific minimum ages. †††† Revaccination with meningococcal vaccine is recommended for previously vaccinated persons who remain at high risk for meningococcal disease. (Source: CDC. Updated recommendations from the Advisory Committee on Immunization Practices (ACIP) for revaccination of persons at prolonged increased risk for meningococcal disease. MMWR 2009;58:[1042--3]). §§§§ Only 1 dose of Tdap is recommended. Subsequent doses should be given as Td. For one brand of Tdap, the minimum age is 11 years. For management of a tetanus-prone wound in persons who have received a primary series of tetanus-toxoid--containing vaccine, the minimum interval after a previous dose of any tetanus-containing vaccine is 5 years. ¶¶¶¶ A second dose of PPSV 5 years after the first dose is is recommended for persons aged ≤65 years at highest risk for serious pneumococcal infection and those who are likely to have a rapid decline in pneumococcal antibody concentration. (Source: CDC. Prevention of pneumococcal disease: recommendations of the Advisory Committee on Immunization Practices [ACIP]. MMWR 1997;46[No. RR-8]). ***** Bivalent HPV vaccine is approved for females aged 10--25 years. Quadrivalent HPV vaccine is approved for males and females aged 9--26 years. ††††† The minimum age for HPV-3 is based on the baseline minimum age for the first dose (i.e., 108 months) and the minimum interval of 24 weeks between the first and third dose. Dose 3 need not be repeated if it is administered at least 16 weeks after the first dose. §§§§§ The first dose of rotavirus must be administered at age 6 weeks through 14 weeks and 6 days. The vaccine series should not be started for infants aged ≥15 weeks, 0 days. Rotavirus should not be administered to children older than 8 months, 0 days of age regardless of the number of doses received between 6 weeks and 8 months, 0 days of age. ¶¶¶¶¶ If 2 doses of Rotarix (GlaxoSmithKline) are administered as age appropriate, a third dose is not necessary. ****** Herpes zoster vaccine is recommended as a single dose for persons aged ≥60 years. |
|
Vaccine† |
Trade name (year licensed) |
Age range |
Routinely recommended ages |
|---|---|---|---|
|
Hib-HepB |
Comvax (1996) |
6 weeks--71 months |
Three-dose schedule at 2, 4, and 12--15 months of age |
|
DTaP/Hib |
TriHIBit (1996) |
15--18 months |
Fourth dose of Hib and DTaP series |
|
HepA-HepB |
Twinrix (2001) |
≥18 years |
Three doses on a schedule of 0, 1, and 6 months |
|
DTaP-HepB-IPV |
Pediarix (2002) |
6 weeks--6 years |
Three-dose series at 2, 4 and 6 months of age |
|
MMRV |
ProQuad (2005) |
12 months--12 years |
Two doses, the first at 12--15 months, the second at 4--6 years |
|
DTaP-IPV |
Kinrix (2008) |
4--6 years |
Fifth dose of DTaP and fourth dose of IPV |
|
DTaP-IPV/Hib |
Pentacel (2008) |
6 weeks--4 years |
Four-dose schedule at 2, 4, 6, and 15--18 months of age |
|
Abbreviations: DT = diphtheria and tetanus toxoids; DTaP = diphtheria and tetanus toxoids and acellular pertussis; FDA = Food and Drug Administration; HepA = hepatitis A; HepB = hepatitis B; Hib = Haemophilus influenzae type b; IPV = inactivated poliovirus; MMR = measles, mumps, and rubella; MMRV = measles, mumps, rubella, and varicella; Td = tetanus and diphtheria toxoids; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis. Source: American Academy of Pediatrics. Passive immunization. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, eds. Red book: 2009 report of the Committee on Infectious Diseases. 28th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2009. * Although MMR, DTaP, DT, Td, and Tdap are combination vaccines, they are not included on this list because they are not available in the United States as single-antigen products. † A dash ( - ) between vaccine products indicates that products are supplied in their final form by the manufacturer and do not require mixing or reconstitution by the user. A slash ( / ) indicates that the products must be mixed or reconstituted by the user. |
|||
|
TABLE 6. (Continued) Contraindications and precautions* to commonly used vaccines |
||
|---|---|---|
|
Vaccine |
Contraindications |
Precautions |
|
PCV |
Severe allergic reaction (e.g., anaphylaxis) after a previous dose (of PCV7, PCV13, or any diphtheria toxoid--containing vaccine) or to a component of a vaccine (PCV7, PCV13, or any diphtheria toxoid--containing vaccine) |
Moderate or severe acute illness with or without fever |
|
TIV |
Severe allergic reaction (e.g., anaphylaxis) after previous dose or to vaccine component, including egg protein |
GBS <6 weeks after a previous dose of influenza vaccine Moderate or severe acute illness with or without fever |
|
LAIV |
Severe allergic reaction (e.g., anaphylaxis) after previous dose or to vaccine component, including egg protein Pregnancy Immunosuppression Certain chronic medical conditions*** |
GBS <6 weeks after a previous dose of influenza vaccine Moderate of severe acute illness with or without fever |
|
PPSV |
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component |
Moderate or severe acute illness with or without fever |
|
MCV4 |
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component |
Moderate or severe acute illness with or without fever |
|
MPSV4 |
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component |
Moderate or severe acute illness with or without fever |
|
HPV |
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component |
Pregnancy Moderate or severe acute illness with or without fever |
|
Rotavirus |
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component SCID |
Altered immunocompetence other than SCID History of intussusception Chronic gastrointestinal disease††† Spina bifida or bladder exstrophy††† Moderate or severe acute illness with or without fever |
|
Zoster |
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component Substantial suppression of cellular immunity Pregnancy |
Moderate or severe acute illness with or without fever |
|
Abbreviations: DT = diphtheria and tetanus toxoids; DTaP = diphtheria and tetanus toxoids and acellular pertussis; GBS = Guillian-Barré syndrome; HBsAg = hepatitis B surface antigen; Hib = Haemophilus influenzae type b; HIV = human immunodeficiency virus; HPV = human papillomavirus; IPV = inactivated poliovirus; LAIV = live, attenuated influenza vaccine; MCV4 = quadrivalent meningococcal conjugate vaccine; MMRV = measles, mumps, rubella, and varicella; MPSV4 = quadrivalent meningococcal polysaccharide vaccine; PCV = pneumococcal conjugate vaccine; PPSV = pneumococcal polysaccharide vaccine; SCID = severe combined immunodeficiency; Td = tetanus and diphtheria toxoids; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis; TIV = trivalent inactivated influenza vaccine. * Events or conditions listed as precautions should be reviewed carefully. Benefits of and risks for administering a specific vaccine to a person under these circumstances should be considered. If the risk from the vaccine is believed to outweigh the benefit, the vaccine should not be administered. If the benefit of vaccination is believed to outweigh the risk, the vaccine should be administered. Whether and when to administer DTaP to children with proven or suspected underlying neurologic disorders should be decided on a case-by-case basis. † HIV-infected children may receive varicella and measles vaccine if CD4+ T-lymphocyte count is >15%. (Source: Adapted from American Academy of Pediatrics. Passive immunization. In: Pickering LK, ed. Red book: 2009 report of the committee on infectious diseases. 28th ed. Elk Grove Village, IL: American Academy of Pediatrics: 2009.) § MMR and varicella vaccines can be administered on the same day. If not administered on the same day, these vaccines should be separated by at least 28 days. ¶ Substantially immunosuppressive steroid dose is considered to be ≥2 weeks of daily receipt of 20 mg or 2 mg/kg body weight of prednisone or equivalent. ** See text and Table 5 for details. †† Measles vaccination might suppress tuberculin reactivity temporarily. Measles-containing vaccine can be administered on the same day as tuberculin skin testing. If testing cannot be performed until after the day of MMR vaccination, the test should be postponed for ≥4 weeks after the vaccination. If an urgent need exists to skin test, do so with the understanding that reactivity might be reduced by the vaccine. §§ Hepatitis B vaccination should be deferred for infants weighing <2,000 g if the mother is documented to be HBsAg-negative at the time of the infant's birth. Vaccination can commence at chronological age 1 month or at hospital discharge. For infants born to HBsAg-positive women, hepatitis B immune globulin and hepatitis B vaccine should be administered within 12 hours after birth, regardless of weight. ¶¶ Vaccine should be deferred for the appropriate interval if replacement immune globulin products are being administered (see Table 5). *** Source: CDC. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR 2010;59(No. RR-8). ††† For details, see CDC. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices. MMWR 2009;58(No. RR-2). |
||
|
TABLE 7. (Continued) Conditions commonly misperceived as contraindications to vaccination |
|
|---|---|
|
Vaccine |
Conditions commonly misperceived as contraindications (i.e., vaccination may be administered under these conditions) |
|
Rotavirus |
Prematurity Immunosuppressed household contacts Pregnant household contacts |
|
Zoster |
Therapy with low-dose methotrexate (≤0.4 mg/kg/week), azathioprine (≤3.0 mg/kg/day), or 6-mercaptopurine (≤1.5 mg/kg/day) for treatment of rheumatoid arthritis, psoriasis, polymyositis, sarcoidosis, inflammatory bowel disease, or other conditions Health-care providers of patients with chronic diseases or altered immunocompetence Contacts of patients with chronic diseases or altered immunocompetence Unknown or uncertain history of varicella in a U.S.-born person |
|
Abbreviations: DT = diphtheria and tetanus toxoids; DTP = diphtheria toxoid, tetanus toxoid, and pertussis; DTaP = diphtheria and tetanus toxoids and acellular pertussis; HBsAg = hepatitis B surface antigen; Hib = Haemophilus influenzae type b; HPV = human papillomavirus; IPV = inactivated poliovirus; LAIV = live, attenuated influenza vaccine; MCV4 = quadrivalent meningococcal conjugate vaccine; MMR = measles, mumps, and rubella; MPSV4 = quadrivalent meningococcal polysaccharide vaccine; PCV = pneumococcal conjugate vaccine; PPSV = pneumococcal polysaccharide vaccine; Td = tetanus and diphtheria toxoids; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis; TIV = trivalent inactivated influenza vaccine. * Antibacterial drugs might interfere with Ty21a oral typhoid vaccine, and certain antiviral drugs might interfere with varicella-containing vaccines and LAIV. † Hepatitis B vaccination should be deferred for infants weighing <2,000 g if the mother is documented to be HBsAg-negative at the time of the infant's birth. Vaccination can commence at chronological age 1 month or at hospital discharge. For infants born to HBsAg-positive women, hepatitis B immune globulin and hepatitis B vaccine should be administered within 12 hours after birth, regardless of weight. § MMR and varicella vaccines can be administered on the same day. If not administered on the same day, these vaccines should be separated by at least 28 days. ¶ HIV-infected children should receive immune globulin after exposure to measles. HIV-infected children can receive varicella and measles vaccine if CD4+ T-lymphocyte count is >15%. (Source: Adapted from American Academy of Pediatrics. Passive immunization. In: Pickering LK, ed. Red book: 2009 report of the Committee on Infectious Diseases. 28th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2009.) ** Measles vaccination might suppress tuberculin reactivity temporarily. Measles-containing vaccine can be administered on the same day as tuberculin skin testing. If testing cannot be performed until after the day of MMR vaccination, the test should be postponed for at least 4 weeks after the vaccination. If an urgent need exists to skin test, do so with the understanding that reactivity might be reduced by the vaccine. †† If a vaccinee experiences a presumed vaccine-related rash 7--25 days after vaccination, the person should avoid direct contact with immunocompromised persons for the duration of the rash. |
|
|
TABLE 9. Dose and route of administration for selected vaccines |
||
|---|---|---|
|
Vaccine |
Dose |
Route |
|
DTaP, DT, Td, Tdap |
0.5 mL |
IM |
|
DTaP-HepB-IPV |
0.5 mL |
IM |
|
DTaP/Hib |
0.5 mL |
IM |
|
DTaP-IPV/Hib |
0.5 mL |
IM |
|
DTaP-IPV |
0.5 mL |
IM |
|
Hib |
0.5 mL |
IM |
|
Combination Hib/HepB |
0.5 mL |
IM |
|
HepA |
≤18 years: 0.5 mL ≥19 years: 1.0 mL |
IM |
|
HepB |
≤19 years: 0.5 mL* ≥20 years: 1.0 mL |
IM |
|
HepA-HepB |
≥18 years: 1.0 mL |
IM |
|
LAIV |
0.2 mL divided dose between nares |
Intranasal spray |
|
TIV |
6--35 months: 0.25 mL ≥3 years: 0.5 mL |
IM |
|
MMR |
0.5 mL |
SC |
|
MMRV |
0.5 mL |
SC |
|
MCV4 |
0.5 mL |
IM |
|
MPSV4 |
0.5 mL |
SC |
|
PCV |
0.5 mL |
IM |
|
PPSV |
0.5 mL |
IM or SC |
|
HPV (HPV2 or HPV4) |
0.5 mL |
IM |
|
IPV |
0.5 mL |
IM or SC |
|
Rotavirus (RV1 or RV5) |
(1.0 mL or 2.0 mL) |
Oral |
|
Varicella |
0.5 mL |
SC |
|
Herpes zoster |
0.65 mL |
SC |
|
Abbreviations: DT = diphtheria and tetanus toxoids; DTP = diphtheria toxoid, tetanus toxoid, and pertussis; DTaP = diphtheria and tetanus toxoids and acellular pertussis; HepA = hepatitis A; HepB = hepatitis B; Hib = Haemophilus influenzae type b; HPV = human papillomavirus; HPV2 = bivalent HPV vaccine; HPV4 = quadrivalent HPV vaccine; IM = intramuscular; IPV = inactivated poliovirus; LAIV = live, attenuated influenza vaccine; MCV4 = quadrivalent meningococcal conjugate vaccine; MMR = measles, mumps, and rubella; MMRV = measles, mumps, rubella, and varicella; MPSV4 = quadrivalent meningococcal polysaccharide vaccine; PCV = pneumococcal conjugate vaccine; PPSV = pneumococcal polysaccharide vaccine; SC = subcutaneous; Td = tetanus and diphtheria toxoids; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis; TIV = trivalent inactivated influenza vaccine. Source: Adapted from Immunization Action Coalition: http://www.immunize.org. * Persons aged 11--15 years may be administered Recombivax HB (Merck), 1.0 mL (adult formulation) on a 2-dose schedule. |
||
|
Vaccines |
Vaccine storage temperature |
Diluent storage temperature |
Comments |
|---|---|---|---|
|
Nonlyophilized, aluminum-adjuvanted vaccines |
|||
|
Diphtheria-tetanus--containing vaccines (DT, Td) or pertussis-containing vaccines (DTaP, Tdap) |
35°F--46°F (2°C--8°C) Do not freeze. |
No diluent* |
Irreversible loss of potency occurs with exposure to freezing temperatures. |
|
HepA and HepB |
35°F--46°F (2°C--8°C) Do not freeze. |
No diluent |
Irreversible loss of potency occurs with exposure to freezing temperatures. |
|
PCV |
35°F--46°F (2°C--8°C) Do not freeze. |
No diluent |
Irreversible loss of potency occurs with exposure to freezing temperatures. |
|
HPV† |
35°F--46°F (2°C--8°C) Do not freeze. |
No diluent |
Irreversible loss of potency occurs with exposure to freezing temperatures. |
|
Nonlyophilized, non--aluminum-adjuvanted vaccines |
|||
|
PRP-OMP Hib |
35°F--46°F (2°C--8°C) |
No diluent |
--- |
|
IPV |
35°F--46°F (2°C--8°C) |
No diluent |
Data on thermostability properties of these vaccines are lacking. |
|
MCV4†,§ |
35°F--46°F (2°C--8°C) |
No diluent |
Data on thermostability properties of these vaccines are lacking. |
|
PPSV |
35°F--46°F (2°C--8°C) |
No diluent |
Data on thermostability properties of these vaccines are lacking. |
|
TIV† |
35°F--46°F (2°C--8°C) |
No diluent |
Data on thermostability properties of these vaccines are lacking. |
|
Lyophilized (nonvaricella) vaccines |
|||
|
PRP-T Hib† |
35°F--46°F (2°C--8°C)¶ |
35°F--46°F (2°C--8°C) Do not freeze. |
--- |
|
MMR† |
35°F--46°F (2°C--8°C)¶ |
35°F--77°F (2°C--25°C) Can be refrigerated or stored at room temperature |
Do not expose to light or temperatures above the recommended range. |
|
MPSV4 |
35°F--46°F (2°C--8°C)¶ |
Data are lacking on ideal pre-reconstitution storage requirements. After reconstitution, vaccine should be stored at 35°F--46°F (2°C--8°C). Do not freeze. |
Freeze dried (lyophilized) vaccine. Data on the effect of freezing temperatures on potency are lacking. |
|
Varicella-containing vaccines |
|||
|
MMRV† |
-58°F--5°F (-50°C to -15°C) |
35°F--77°F (2°C--25°C) Can be refrigerated or stored at room temperature |
--- |
|
Varicella† |
≤5°F (≤--15°C) |
35°F--77°F (2°C--25°C) Can be refrigerated or stored at room temperature |
--- |
|
Herpes zoster† |
≤5°F (≤--15°C) |
35°F--77°F (2°C--25°C) Can be refrigerated or stored at room temperature |
--- |
|
Noninjectable vaccines |
|||
|
RV5 vaccine† |
35°F--46°F (2°C--8°C) Do not freeze. |
No diluent |
--- |
|
RV1 vaccine† |
35°F--46°F (2°C--8°C) Do not freeze. |
The diluent may be stored at a controlled room temperature 20°C--25°C (68°F--77°F). Do not freeze. |
--- |
|
LAIV |
35°F--46°F (2°C--8°C) |
No diluent |
Do not expose to temperatures above the recommended range. |
|
Abbreviations: DT = diphtheria and tetanus toxoids; DTaP = diphtheria and tetanus toxoids and acellular pertussis; HepA = hepatitis A; HepB = hepatitis B; Hib = Haemophilus influenzae type b; HPV = human papillomavirus; IPV = inactivated poliovirus; LAIV = live, attenuated influenza vaccine; MCV4 = quadrivalent meningococcal conjugate vaccine; MMR = measles, mumps, and rubella; MMRV = measles, mumps, rubella, and varicella; MPSV4 = quadrivalent meningococcal polysaccharide vaccine; PCV = pneumococcal conjugate vaccine; PPSV = pneumococcal polysaccharide vaccine; PRP-OMB = polyribosylribitol phosphate-meningococcal outer membrane protein conjugate; PRP-T = polyribosylribitol phosphate polysaccharide conjugated to a tetanus toxoid; RV = rotavirus; RV1 = live, attenuated monovalent rotavirus vaccine; RV5 = live, reassortment pentavalent rotavirus vaccine; Td = tetanus and diphtheria toxoids; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis; TIV = trivalent inactivated influenza vaccine. Source: Adapted from Atkinson WL, Kroger AT, Pickering LK. General immunization practices. In: Plotkin SA, Orenstein WA, editors. Vaccines. 35th ed. Philadelphia, PA: Elsevier; 2008; and CDC. Guidelines for maintaining and managing the vaccine cold chain. MMWR 2003;52:1023--5. * DTaP--Tripedia is sometimes used as a diluent for ActHib. † Protect from light. § There are two meningococcal conjugate vaccines; Menactra is nonlyophilized, and Menveo is lyophilized. Both powder and diluent should be stored at 35°F--46°F. ¶ The lyophilized pellet may be stored at freezer temperature; the reconstituted vaccine should be stored at refrigerator temperature. |
|||
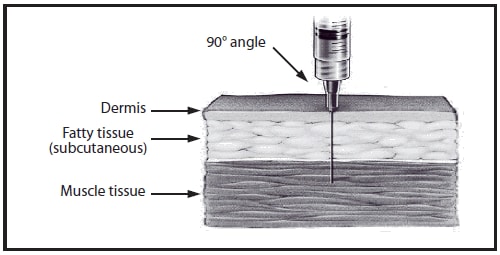
Source: Adapted from California Immunization Branch.
Alternate Text: This drawing shows intramuscular needle insertion into a cross-section of skin. The needle is inserted at a 90-degree angle and penetrates the dermis, fatty tissue (subcutaneous), and muscle tissue.

Source: Adapted from Minnesota Department of Health.
Alternate Text: This drawing shows a mother holding an infant. The anterolateral aspect of the infant's thigh is shaded, showing the proper site for intramuscular/subcutaneous vaccine administration.
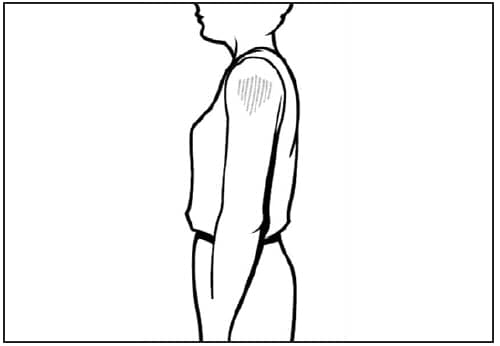
Source: Adapted from Minnesota Department of Health.
Alternate Text: This line drawing is a side view of a child. The deltoid muscle of the arm is shaded, showing the proper site for intramuscular vaccine administration.
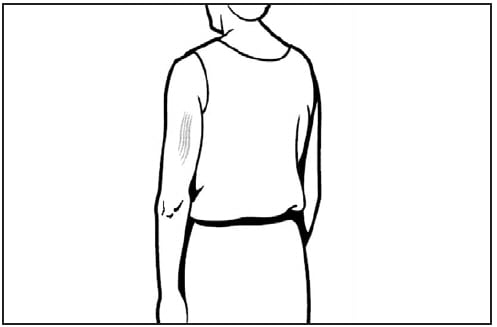
Source: Adapted from Minnesota Department of Health.
Alternate Text: This drawing is a back view of a person. The triceps muscle of the arm is shaded, showing the proper site for subcutaneous vaccine administration.
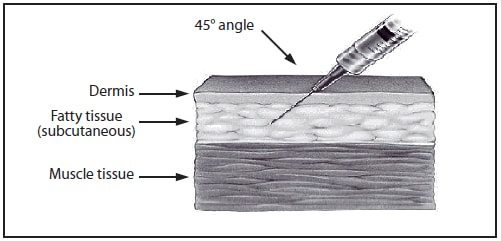
Source: Adapted from California Immunization Branch.
Alternate Text: This drawing shows subcutaneous needle insertion into a cross-section of skin. The needle is inserted at a 45-degree angle and penetrates the dermis and fatty tissue (subcutaneous) but not the muscle tissue.
Source: Adapted from Immunization Action Coalition. Available at http://www.immunize.org/catg.d/p3039.pdf. Accessed December 1, 2010.
Alternate Text: This figure shows a sample vaccine temperature log from the Immunization Action Coalition, including refrigerator temperatures, freezer temperatures, and date and time. Shaded areas indicate temperatures at which immediate action should be taken.
Advisory Committee on Immunization Practices
Membership List, October 2009
Chair: Carol Baker, MD, Baylor College of Medicine, Houston, Texas.
Executive Secretary: Larry Pickering, MD, National Center for Immunization and Respiratory Diseases, CDC, Atlanta, Georgia.
Members: Lance Chilton, MD, University of New Mexico, Albuquerque, New Mexico; Paul Cieslak, MD, Oregon Public Health Division, Portland, Oregon; Kristen Ehresmann, MPH, Minnesota Department of Health, St. Paul, Minnesota; Janet Englund, MD, University of Washington and Children's Hospital and Regional Medical Center, Seattle, Washington; Franklyn Judson, MD, University of Colorado HealthSciences Center, Denver, Colorado; Wendy Keitel, MD, Baylor College of Medicine, Houston, Texas; Susan Lett, MD, Massachusetts Department of Public Health, Boston, Massachusetts; Michael Marcy, MD, UCLA Center for Vaccine Research, Torrance, California; Cody Meissner, MD, Tufts Medical Center, Boston, Massachusetts; Kathleen Neuzil, MD, University of Washington; Seattle, Washington; Mark Sawyer, MD, University of California - San Diego, California; Ciro Valent Sumaya, MD, Texas A&M Health Science Center, College Station, Texas; Jonathan Temte, MD, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin.
Ex Officio Members: James E. Cheek, MD, Indian Health Service, Albuquerque, New Mexico; Wayne Hachey, DO, Department of Defense, Falls Church, Virginia; Geoffrey S. Evans, MD, Health Resources and Services Administration, Rockville, Maryland; Bruce Gellin, MD, National Vaccine Program Office, Washington, District of Columbia; Linda Murphy, Centers for Medicare and Medicaid Services, Baltimore, Maryland; George T. Curlin, MD, National Institutes of Health, Bethesda, Maryland; Norman Baylor, PhD, Food and Drug Administration, Bethesda, Maryland; Linda Kinsinger, MD, Department of Veterans Affairs, Durham, North Carolina.
Liaison Representatives: American Academy of Family Physicians, Doug Campos-Outcalt, MD, Phoenix, Arizona; American Academy of Pediatrics, Joseph Bocchini, MD, Shreveport, Louisiana, David Kimberlin, MD, Birmingham, Alabama; American College Health Association, James C. Turner, MD, Charlottesville, Virginia; American College of Obstetricians and Gynecologists, Stanley Gall, MD, Louisville, Kentucky; American College of Physicians, Gregory Poland, MD, Rochester, Minnesota; American Geriatrics Society, Kenneth Schmader, MD, Durham, North Carolina; America's Health Insurance Plans, Mark Netoskie, MD, MBA, Houston, Texas; American Medical Association, Litjen Tan, PhD, Chicago, Illinois; American Osteopathic Association, Stanley Grogg, DO, Tulsa, Oklahoma; American Pharmacists Association, Stephan L. Foster, PharmD, Memphis, Tennessee; Association for Prevention Teaching and Research, W. Paul McKinney, MD, Louisville, Kentucky; Biotechnology Industry Organization, Clement Lewin, PhD, Cambridge, Massachusetts; Canadian National Advisory Committee on Immunization, Joanne Langley, MD, Halifax, Nova Scotia, Canada; Department of Health, United Kingdom David M. Salisbury, MD, London, United Kingdom; Healthcare Infection Control Practices Advisory Committee, Alexis Elward, MD, St. Louis, Missouri; Infectious Diseases Society of America, Samuel L. Katz, MD, Durham, North Carolina; National Association of County and City Health Officials, Jeff Duchin, MD, Seattle, Washington; National Association of Pediatric Nurse Practitioners, Patricia Stinchfield, MPH, St Paul, Minnesota; National Foundation for Infectious Diseases, William Schaffner, MD, Nashville, Tennessee; National Immunization Council and Child Health Program, Mexico, Vesta Richardson, MD, Mexico City, Mexico; National Medical Association, Patricia Whitley-Williams, MD, New Brunswick, New Jersey; National Vaccine Advisory Committee, Guthrie Birkhead, MD, Albany, New York; Pharmaceutical Research and Manufacturers of America, Damian A. Braga, Swiftwater, Pennsylvania, Peter Paradiso, PhD, Collegeville, Pennsylvania; Society for Adolescent Medicine, Amy Middleman, MD, Houston, Texas; Society for Healthcare Epidemiology of America, Harry Keyserling, MD, Atlanta, Georgia.
Members of the General Recommendations on Immunization Working Group
Advisory Committee on Immunization Practices (ACIP), Ciro V. Sumaya, MD; Lance Chilton, MD; Susan Lett, MD; Mark H. Sawyer, MD; ACIP Liaison and Ex-Officio Members, Doug Campos-Outcalt, MD, American Academy of Family Physicians; Geoffrey S. Evans, MD, Health Resources and Services Administration; Stephan L. Foster, PharmD, American Pharmacists Association; Stanley Grogg, DO, American Osteopathic Association; Harry Keyserling, MD, Society for Healthcare Epidemiology of America; CDC staff members, William L. Atkinson, MD, Angela Calugar, MD, Ted Cieslak, MD, Amanda Cohn, MD, Christine Robinette Curtis, MD, Carol Friedman, DO,* Sophie Greer, Andrew Kroger, MD, Nancy Levine, PhD, Elaine Miller, Gina Mootrey, DO, Larry Pickering, MD, Jean Smith, MD, Greg Wallace, MD; other members and consultants, Richard Clover, MD, University of Louisville School of Public Health; Sandra Jo Hammer, RN, California Department of Public Health; Kelly L. Moore, MD, Tennessee Department of Health; Lorry Rubin, MD, Schneider Children's Hospital; Shainoor Ismail, MD, Public Health Agency of Canada; Deborah Wexler, MD, Immunization Action Coalition; Richard Zimmerman, MD, University of Pittsburgh School of Medicine.
* Deceased.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
References to non-CDC sites on the Internet are provided as a service to MMWR readers and do not constitute or imply endorsement of these organizations or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of pages found at these sites. URL addresses listed in MMWR were current as of the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.
