
How antimicrobial resistance happens.

AR can spread between people, animals, and the environment, and can cause deadly infections.

Combat AR through infection prevention, improved antibiotic/antifungal use, actions to slow spread.

The AR Solutions Initiative invests to detect, respond, contain & prevent drug-resistant infections.
Antimicrobial Resistance Laboratory Networks Resources
Resources about CDC's AR Lab Network for U.S. labs for quicker response to antimicrobial resistance.
About CDC's Global Antimicrobial Resistance Laboratory and Response Network to fight antimicrobial
A summary of antibiotic and antifungal resistance testing offered through CDC’s AR Lab Network.
Find resources and testing information for U.S. laboratories.
LAARC laboratory assessment tool helps improve AR detection and reporting.
The AR Isolate Bank helps researchers develop new drugs and tests to fight drug resistance.
Featured
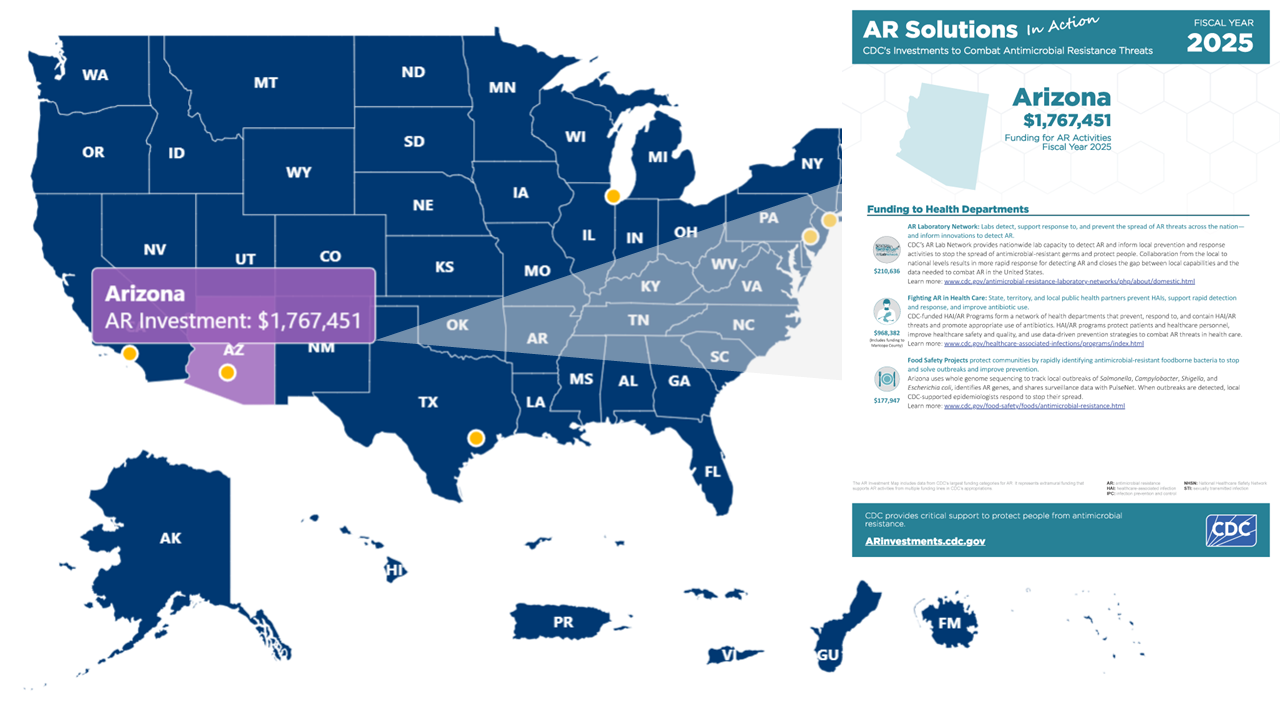
Map highlights CDC investments to protect Americans from drug-resistant infections.
CDC's 2019 AR Threats Report includes national estimates for 18 antimicrobial-resistant germs.
The U.S. lost progress combating AR in 2020 due, in large part, to effects of the COVID-19 pandemic.

Global antimicrobial resistance (AMR) experts collaborate to strengthen efforts to combat AMR.

Feature stories: Learn how CDC and partners are addressing antimicrobial resistance.

Key messages, graphics, and toolkits for U.S. Antibiotic Awareness Week.