Smoking and Oral Health in Dentate Adults aged 18–64
- Key findings
- Does oral health status differ by smoking status for dentate adults aged 18–64?
- Does oral health status compared with others the same age differ by smoking status for dentate adults aged 18–64?
- Does the number of oral health problems differ by smoking status for dentate adults aged 18–64?
- Does the length of time since last dental visit differ by smoking status for dentate adults aged 18–64?
- Do the reasons for not seeing a dentist for an oral health problem differ by smoking status for dentate adults aged 18–64?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 85, February 2012
PDF Version (661 KB)
Barbara Bloom, M.P.A.; Patricia F. Adams; Robin A. Cohen, Ph.D.; and Catherine Simile, Ph.D.
Key findings
Data from the National Health Interview Survey, 2008
- Current smokers (16%) were twice as likely as former smokers (8%) and four times as likely as never smokers (4%) to have poor oral health status.
- Current smokers (35%) were almost one and one-half times as likely as former smokers (24%) and more than two times as likely as never smokers (16%) to have had three or more oral health problems.
- Current smokers (19%) were about twice as likely as former smokers (9%) and never smokers (10%) to have not had a dental visit in more than 5 years or have never had one.
- Cost was the reason that most adults with an oral health problem did not see a dentist in the past 6 months; 56% of current smokers, 36% of former smokers, and 35% of never smokers could not afford treatment or did not have insurance.
There is a vast body of literature documenting the adverse effects of cigarette smoking on health (1–5). In 2000 the Surgeon General’s report on oral health noted that lifestyle behaviors such as smoking affect oral health as well as general health. It also emphasized the importance of oral health to overall health (6). This report examines differences among current smokers, former smokers, and never smokers in terms of oral health status, number of oral health problems, and the utilization of dental services. The study is limited to dentate adults aged 18–64.
Keywords: mouth, teeth, cigarette smoking, National Health Interview Survey
Does oral health status differ by smoking status for dentate adults aged 18–64?
- Among dentate adults aged 18–64, the percentages of adults with very good and good oral health status were higher for never smokers than for former smokers, and higher for former smokers than for current smokers, while the percentages of adults with fair and poor oral health status were lower for never smokers than for former smokers, and lower for former smokers than for current smokers (Figure 1).
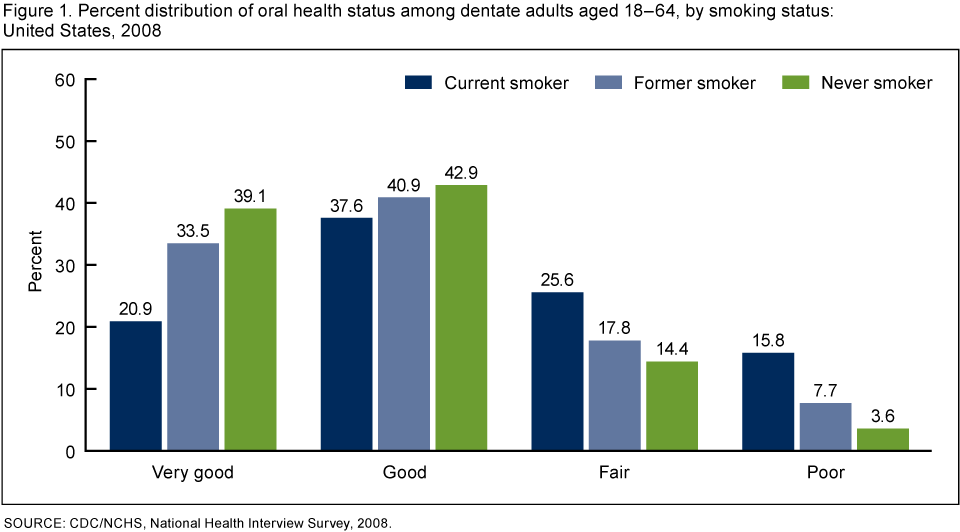
- About 4 out of 10 never smokers had very good oral health status compared with 3 out of 10 former smokers and 2 out of 10 current smokers.
- Sixteen percent of current smokers had poor oral health status compared with 8% of former smokers and 4% of never smokers.
Does oral health status compared with others the same age differ by smoking status for dentate adults aged 18–64?
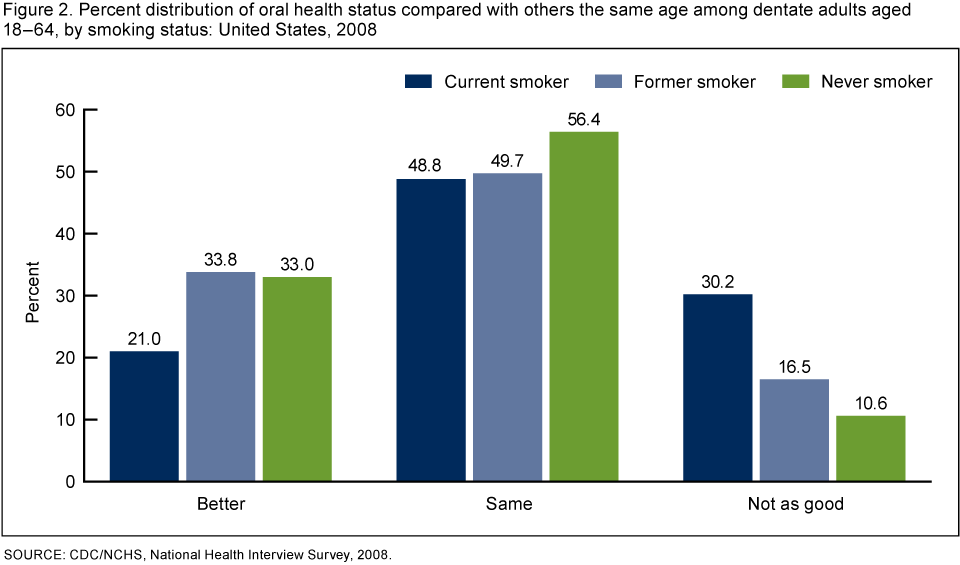
- Among dentate adults aged 18–64, current smokers were less likely than either former smokers or never smokers to evaluate their oral health status as better than others the same age (Figure 2).
- Current smokers (30%) were almost twice as likely as former smokers (17%) and almost three times as likely as never smokers (11%) to evaluate their oral health status as not as good as others the same age.
Does the number of oral health problems differ by smoking status for dentate adults aged 18–64?
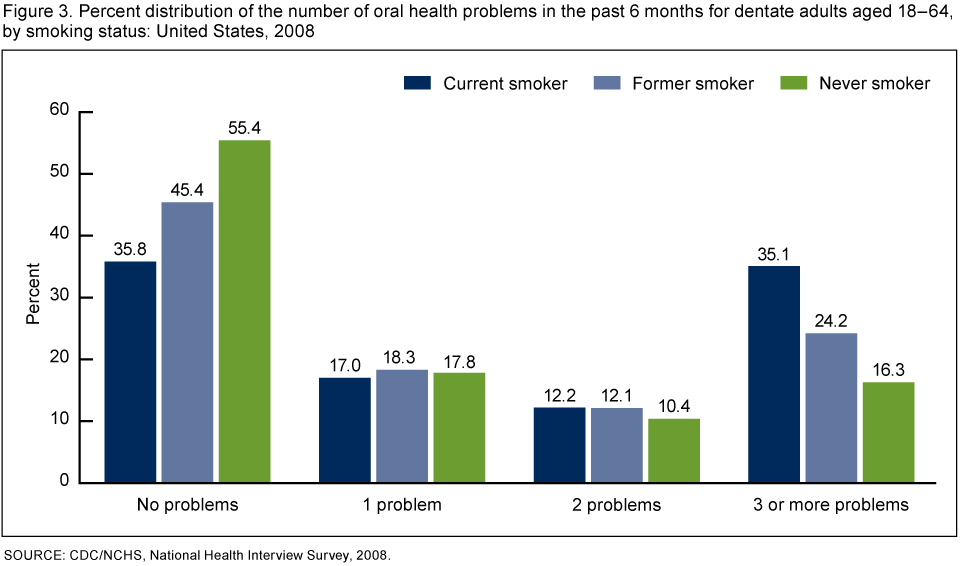
- Among dentate adults aged 18–64, the percentage of adults with no oral health problems was higher for never smokers than for former smokers, and higher for former smokers than for current smokers, while the percentage of adults with three or more problems was lower for never smokers than for former smokers, and lower for former smokers than for current smokers (Figure 3).
- More than one-half of never smokers (55%) had no oral health problems compared with one-third of current smokers (36%).
- Approximately equal percentages of current smokers, former smokers, and never smokers had one or two oral health problems.
- Current smokers (35%) were almost one and one-half times as likely as former smokers (24%) and more than two times as likely as never smokers (16%) to have three or more oral health problems.
Does the length of time since last dental visit differ by smoking status for dentate adults aged 18–64?
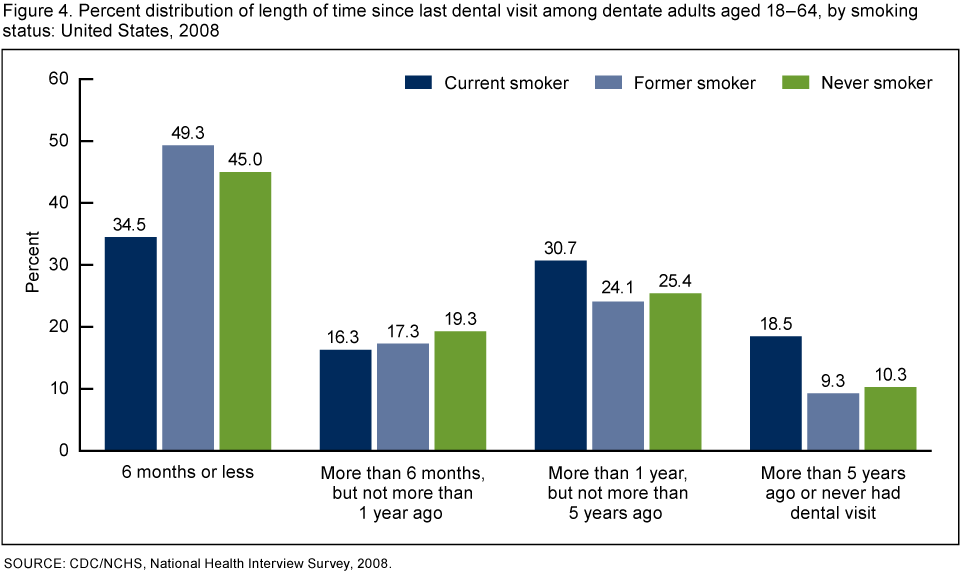
- Among dentate adults aged 18–64, about one-third of current smokers had a dental visit in the last 6 months (35%), compared with about one-half of former smokers (49%) and never smokers (45%) (Figure 4).
- Current smokers (19%) were about twice as likely as former smokers (9%) and never smokers (10%) to have not had a dental visit in more than 5 years or have never had one.
Do the reasons for not seeing a dentist for an oral health problem differ by smoking status for dentate adults aged 18–64?
- Among dentate adults aged 18–64 with an oral health problem who did not see a dentist in the past 6 months, the main reason was cost; 56% of current smokers, 36% of former smokers, and 35% of never smokers could not afford treatment or did not have insurance (Table).
- Never smokers and former smokers were more likely than current smokers to forgo a dental visit for a problem because they thought it was not important.
- Approximately equal percentages of current smokers, former smokers, and never smokers did not visit the dentist for an oral health problem because they were afraid.
Table. Percentage of all dentate adults aged 18-64 who did not see a dentist for an oral health problem in the past 6 months, by reason and smoking status: United States, 2008
| Smoking status | |||
|---|---|---|---|
| Reasons for not seeing a dentist | Current smokers | Former smokers | Never smokers |
| Percent (standard error) | |||
| Could not afford/no insurance | 56.2 (1.66) | 36.4 (1.85) | 34.9 (1.12) |
| Didn’t think problem was important | 22.7 (1.40) | 27.6 (1.69) | 27.9 (1.09) |
| Problem went away | 19.8 (1.33) | 23.1 (1.61) | 29.2 (1.17) |
| Afraid | 10.9 (0.89) | 9.1 (1.16) | 9.6 (0.70) |
| Didn’t think dentist could fix problem | 5.1 (0.63) | 7.8 (1.03) | 5.7 (0.53) |
| Waiting for an appointment | 3.6 (0.64) | 5.0 (0.83) | 4.1 (0.44) |
| No transportation | 4.2 (0.68) | 1.6 (0.42) | 2.2 (0.36) |
Note: Reason categories are not mutually exclusive.
Source: CDC/NCHS, National Health Interview Survey, 2008.
Summary
This report shows that among dentate adults aged 18–64 there are differences in oral health status and oral health care utilization among current smokers, former smokers, and never smokers. Overall, current smokers had a poorer oral health status and more oral health problems than either former smokers or never smokers. Current smokers were also more likely to delay routine dental visits. When current smokers experienced a mouth or tooth problem, they were less likely to visit a dental health professional because they were unable to afford dental care than former smokers or never smokers. However, current smokers were more likely to think that their oral health problem was important.
The evidence for an association between tobacco use and oral diseases has been clearly shown in every Surgeon General’s report on tobacco since 1964 (6). Tobacco use is a risk factor for oral cancers, periodontal diseases, and dental caries, among other diseases. Oral health problems may be early warning signs of other medical problems such as diabetes, HIV, heart disease, or stroke (6). Good oral health is integral to good general health.
Definitions
Terms related to oral health
Dental visit: Any visit to a dentist’s office (including oral surgeons, orthodontists, or other dental specialists) for treatment or advice, including services by a technician or hygienist acting under a dentist’s supervision.
Dentate persons: Persons who have one or more of their permanent teeth.
Interval since last dental visit: Length of time prior to the week of interview since a dentist, dental hygienist, oral surgeon, orthodontist or other dental specialist was last visited for treatment or advice of any type.
Oral health problems: Based on the questions: “DURING THE PAST 6 MONTHS, have you had any of the following problems that lasted more than a day? …Pain in your jaw joint, …Sores in your mouth, …Difficulty eating or chewing, …Bad breath, …Dry mouth.” “DURING THE PAST 6 MONTHS, have you had any of the following problems? …A toothache or sensitive teeth, …Bleeding gums, …Crooked teeth, …Broken or missing teeth, …Stained or discolored teeth, …Loose teeth not due to an injury, …Broken or missing fillings.”
Oral health status: Based on the question: “How would you describe the condition of your mouth and [if dentate] teeth? Would you say very good, good, fair or poor?” There was an additional question about oral health status compared with others the same age: “Would you say the condition of your mouth and [if dentate] teeth is better than, the same as or not as good as other people your age?”
Reason for not seeing a dentist or other dental health professional for an oral health problem: For adults who had at least one oral health problem (see above), based on the questions: “DURING THE PAST 6 MONTHS, why didn’t you see a dentist for the problems with your mouth or teeth? …You didn’t think it was important…the problem went away, …You could not afford treatment or you didn’t have insurance, …You didn’t have transportation, …You were afraid to see a dentist, …You were waiting for an appointment, …You didn’t think a dentist could fix the problem.”
Terms related to smoking status
Current smokers: Adults who have smoked 100 cigarettes in their lifetime and currently smoke cigarettes every day (daily) or some days (nondaily).
Former smokers: Adults who have smoked at least 100 cigarettes in their lifetime, but currently do not smoke.
Never smokers: Adults who have never smoked a cigarette or who have smoked fewer than 100 cigarettes in their entire lifetime.
Caveat
Oral health status is based on the sample adult’s self-assessment of the condition of his/her mouth and teeth. Therefore, an individual’s oral health status may differ from the evaluation of oral health status by a dental health professional. In addition, it is important to note that data in this report are not age-adjusted in order to provide a measure of oral health burden. Some of the oral health problems experienced by current and former smokers may be due to their age rather than to their smoking status. Younger adults are more likely to have never smoked and oral health problems may also be associated with age, independently of smoking.
Data source and methods
Data from the 2008 National Health Interview Survey (NHIS) were used for this analysis. NHIS data are collected continuously throughout the year for the National Center for Health Statistics (NCHS), Centers for Disease Control and Prevention, by interviewers from the U.S. Bureau of the Census. The NHIS collects information about the health and health care of the civilian, noninstitutionalized U.S. population. Interviews are conducted in respondents’ homes, but follow-ups to complete interviews may be conducted over the telephone. The family component collects information on all family members and the sample adult component collects additional data from one randomly selected adult (the “sample adult”). If a child is present in the family, the sample child component collects additional data on one randomly selected child (the “sample child”). Questions about oral health and smoking are from the sample adult component. In 2008, information was collected on a total of 16,414 persons aged 18–64 from the sample adult component of the survey. For further information about the NHIS, including the questionnaire, see the NHIS website.
NHIS is designed to yield a sample representative of the civilian noninstitutionalized population of the United States, and this analysis uses weights to produce national estimates. Data weighting procedures are described in more detail elsewhere (7). Point estimates and estimates of corresponding variances for this analysis were calculated using SUDAAN software (8) to account for the complex sample design of the NHIS. The Taylor series linearization method was chosen for variance estimation. All estimates shown in this report meet the NCHS standard of reliability (relative standard error less than or equal to 30%). Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. Terms such as “higher than” and “less than” indicate statistically significant differences. Terms such as “similar” and “no difference” indicate that the statistics being compared were not significantly different. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not significant.
About the authors
Barbara Bloom, Patricia F. Adams, Robin A. Cohen, and Catherine M. Simile are with the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics, Division of Health Interview Statistics.
References
- U.S. Public Health Service. Smoking and health: A report of the advisory committee to the Surgeon General of the Public Health Service. U.S. Department of Health, Education, and Welfare. Public Health Service. Centers for Disease Control. PHS Publication No. 1103. 1964.
- U.S. Department of Health and Human Services. Reducing the health consequences of smoking: 25 years of progress. A report of the Surgeon General. Rockville, Maryland. U.S. Department of Health and Human Services, Centers for Disease Control, Center for Chronic Disease Prevention and Health Promotion. Office on Smoking and Health. DHHS. Publication No. (CDC) 89–8411. 1989.
- CDC. The health consequences of smoking: A report of the Surgeon General. National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. Washington, DC: U.S. Government Printing Office.
- Tobacco use: Targeting the Nation’s leading killer—At a glance 2010 [PDF – 3.2 MB] [online]. CDC, National Center for Chronic Disease Prevention and Health Promotion.
- National Center for Health Statistics. Health, United States, 2010 With Special Feature on Death and Dying. Hyattsville, MD. 2011.
- U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health. 2000.
- Botman SL, Moore TF, Moriarity CL, Parsons VL. Design and estimation for the National Health Interview Survey, 1995–2004. National Center for Health Statistics. Vital Health Stat 2(130). 2000.
- Research Triangle Institute. SUDAAN (Release 10.0). [Computer Software.] Research Triangle Park, NC. 2008.
Suggested citation
Bloom B, Adams PF, Cohen RA, Simile CM. Smoking and oral health in dentate adults aged 18–64. NCHS data brief, no 85. Hyattsville, MD: National Center for Health Statistics. 2012.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Interview Statistics
Jane F. Gentlemen, Ph.D., Director