The Challenge of Fetal Mortality
- Key findings
- What is the impact of fetal mortality on U.S. families?
- What is the recent trend in fetal mortality?
- Do fetal mortality rates differ among racial and ethnic groups?
- Do twins and other multiple pregnancies have higher fetal mortality rates?
- What is the relationship between fetal mortality and maternal age?
- Do fetal mortality rates differ by number of previous pregnancies?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 16, April 2009
PDF Version (528 KB)
by Marian F. MacDorman, Ph.D., and Sharon Kirmeyer, Ph.D., Division of Vital Statistics
Key findings
Data from the Fetal Death Data File and Linked Birth/Infant Death Data Set, National Vital Statistics System
- The magnitude of fetal mortality is considerable: About 1 million fetal deaths occur at any gestational age in the United States each year, including almost 26,000 at 20 weeks of gestation or more.
- Even when limited to fetal deaths of 20 weeks of gestation or more, nearly as many fetal deaths as infant deaths occur in the United States each year.
- After decades of decline, the U.S. fetal mortality rate (fetal deaths of 20 weeks of gestation or more) did not decrease from 2003 to 2005.
- Fetal mortality rates are substantially higher for non-Hispanic black and American Indian or Alaska Native women than for non-Hispanic white women.
- Compared with the U.S. average, fetal mortality rates are higher for teenagers and for women aged 35 years and over, for twin and higher-order pregnancies, and for women with more than two previous pregnancies.
Fetal mortality is a major, but often overlooked, public health problem. Fetal mortality refers to spontaneous intrauterine death at any time during pregnancy. Fetal deaths later in pregnancy are sometimes referred to as stillbirths (at 20 weeks of gestation or more, or 28 weeks or more, for example) (1,2). Much of the public concern regarding reproductive loss has concentrated on infant mortality, as less is known about fetal mortality. However, the impact of fetal mortality on U.S. families is considerable.
This report examines fetal death data from the National Vital Statistics System (NVSS) (1,3). Vital statistics fetal death data are generally presented for fetal deaths of 20 weeks of gestation or more. Other data sources provide estimates of fetal deaths for all periods of gestation. For example, the National Survey of Family Growth estimates about 1 million fetal losses per year in the United States, with the vast majority of these occurring before 20 weeks of gestation (4).
Keywords: fetal mortality, stillbirth, period of gestation, race and ethnicity
What is the impact of fetal mortality on U.S. families?
In 2005, a total of 25,894 fetal deaths of 20 weeks of gestation or more were reported in the United States, nearly as many as infant deaths (28,384).
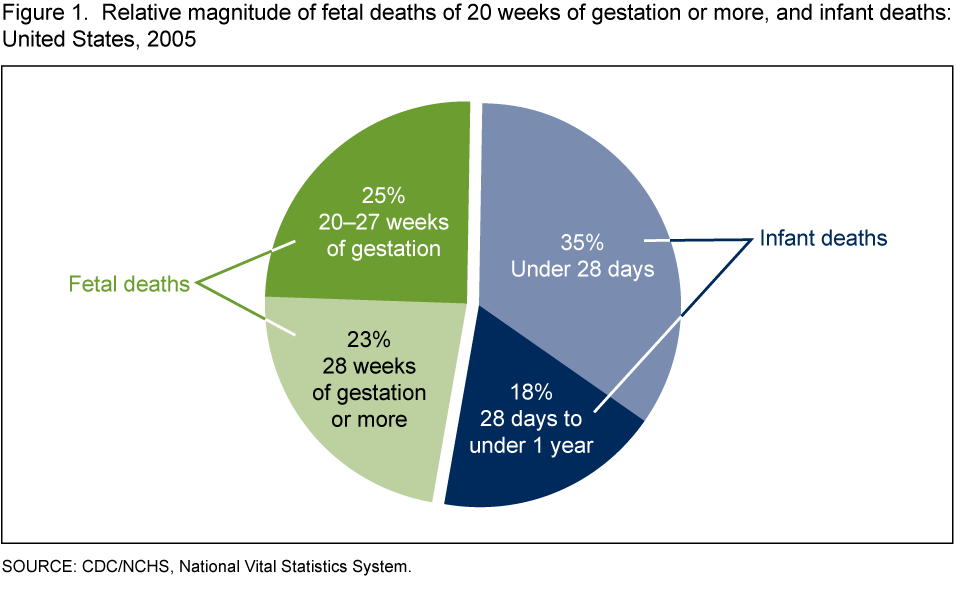
Fetal deaths were nearly evenly divided into those at 20–27 weeks of gestation and those at 28 weeks of gestation or more.
In 2005, the U.S. fetal mortality rate was 6.22 fetal deaths of 20 weeks of gestation or more per 1,000 live births and fetal deaths.
What is the recent trend in fetal mortality?
The U.S. fetal mortality rate declined from 7.49 (fetal deaths of 20 weeks of gestation or more per 1,000 live births and fetal deaths) in 1990 to 6.23 in 2003, but did not decrease thereafter, halting a long-term trend.
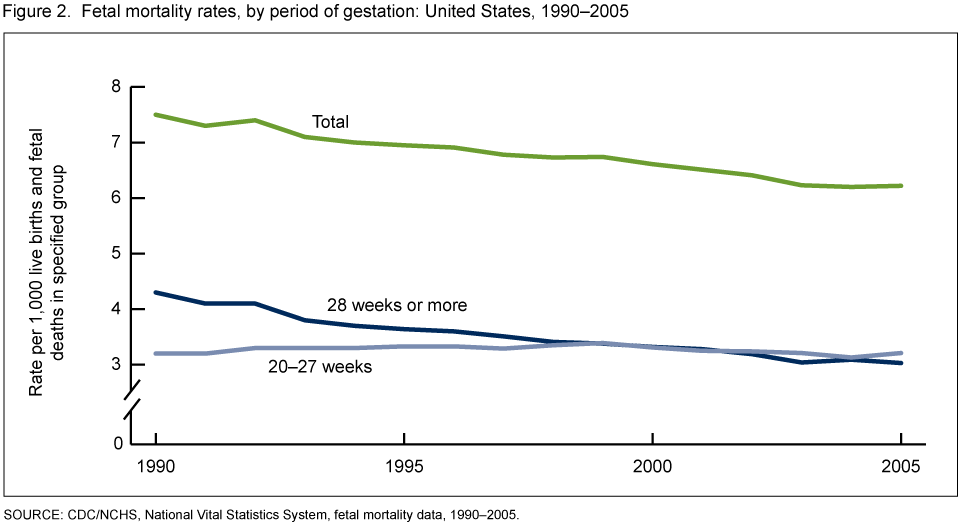
From 1990 to 2003, the rate declined by 17% because of a decrease in late fetal deaths (28 weeks of gestation or more). The fetal mortality rate for 20–27 weeks of gestation did not decline.
The plateau in the U.S. fetal mortality rate from 2003 to 2005 parallels a more long-standing lack of decline in the U.S. infant mortality rate from 2000 to 2005 (1,5,6).
The Healthy People 2010 target goal for the U.S. fetal mortality rate is 4.1 fetal deaths per 1,000 live births and fetal deaths (7). The current U.S. rate is 52% higher than the goal.
Do fetal mortality rates differ among racial and ethnic groups?
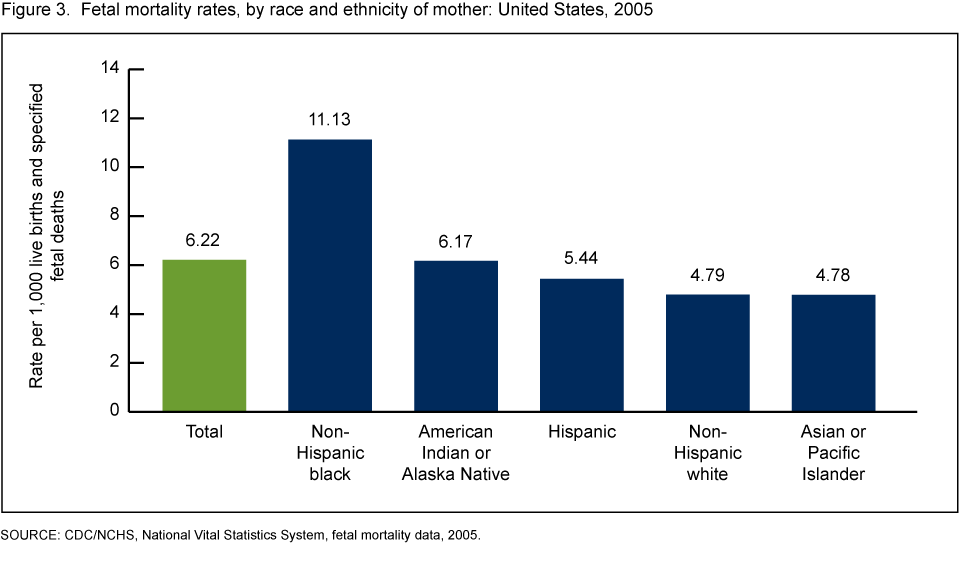
Fetal mortality rates vary considerably by race and ethnicity of the mother. In 2005, the fetal mortality rate for non-Hispanic white women was 4.79 fetal deaths of 20 weeks or more per 1,000 live births and fetal deaths. The rate for Asian or Pacific Islander women was similar (4.78).
In contrast, the fetal mortality rate for non-Hispanic black women was 11.13, or 2.3 times the rate for non-Hispanic white women. The rate for American Indian or Alaska Native women was 29% higher, and for Hispanic women 14% higher, than for non-Hispanic white women.
Part of the higher risk of fetal mortality for non-Hispanic black women relates to their higher risk of preterm delivery. Other factors frequently mentioned as contributing to the black-white fetal mortality gap are differences in maternal preconception health, infection, income, and access to quality health care. However, much of the black-white disparity in fetal mortality remains unexplained (1,8).
Do twins and other multiple pregnancies have higher fetal mortality rates?
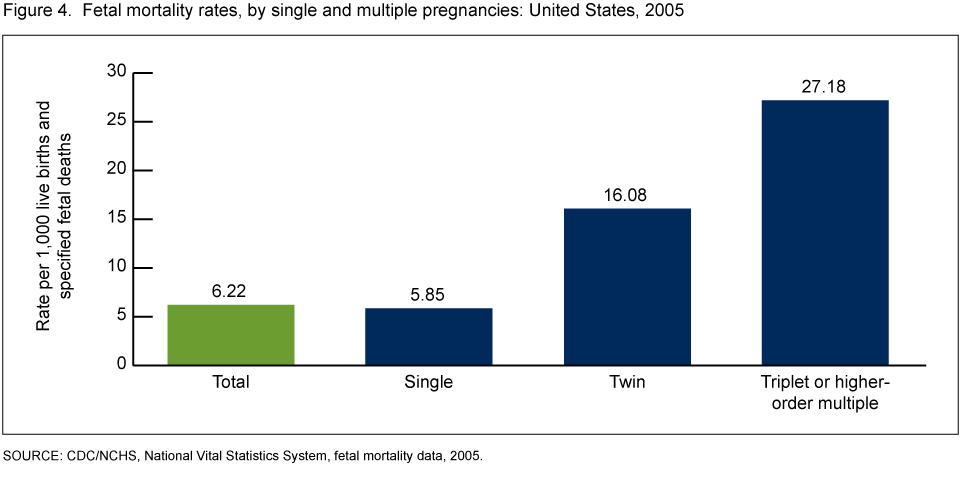
Fetal mortality rates are much higher for twin and triplet and higher-order pregnancies than for pregnancies with a single fetus.
The fetal mortality rate for twin pregnancies (16.08) was 2.7 times the rate for singleton pregnancies (5.85). The fetal mortality rate for triplet and higher-order pregnancies (27.18) was 4.6 times the rate for singleton pregnancies.
In 2005, 9% of fetal deaths in the United States were from a multiple pregnancy, compared with 3% of live births (1).
The increased risk for multiple pregnancies may relate in part to increased rates of preterm labor, fetal growth restriction, maternal hypertension, and placental and cord problems (9). Many multiple pregnancies also result from assisted reproductive technologies, which may increase fetal mortality risk (10).
What is the relationship between fetal mortality and maternal age?
Fetal mortality rates vary considerably by the age of the mother. Fetal mortality rates were lowest for women aged 25–29 years, and were higher for teenagers and those aged 35 years and over.
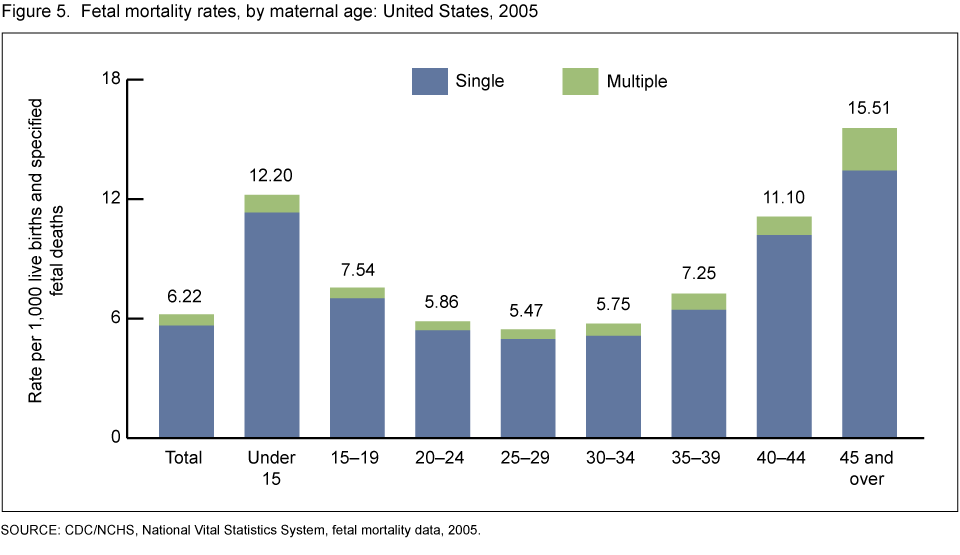
For teenagers, fetal mortality rates were highest for the youngest women. The fetal mortality rate for women under age 15 years was 2.2 times the rate for women aged 25–29 years. The rate for women aged 15–19 years was 38% higher than the rate for women aged 25–29 years.
The higher risk for teenagers may relate to less favorable socioeconomic and behavioral conditions among pregnant teenagers, although biologic immaturity may also play a role, particularly for the youngest teenagers (11).
At the opposite end of the age spectrum, fetal mortality rates also increased rapidly for women aged 35 years and over. The fetal mortality rate for women aged 35–39 years was 33% higher than for women aged 25–29 years. Moreover, the rate for women aged 40–44 years was double and that for women aged 45 years and over was 2.8 times the rate for women aged 25–29 years. Although 9% of fetal deaths were among multiple pregnancies overall, for women aged 45 years and over, the proportion was higher (14%).
Maternal age of 35 years and over appears to be an independent risk factor for fetal death, even after adjusting for medical conditions that are more common among older women, such as hypertension, diabetes, placental problems, and multiple gestation (1,2,11).
Do fetal mortality rates differ by number of previous pregnancies?
Fetal mortality rates were lowest for women with one prior pregnancy (4.87).
Compared with women who had one prior pregnancy, fetal mortality rates were 21% higher for women with no prior pregnancy (5.88).
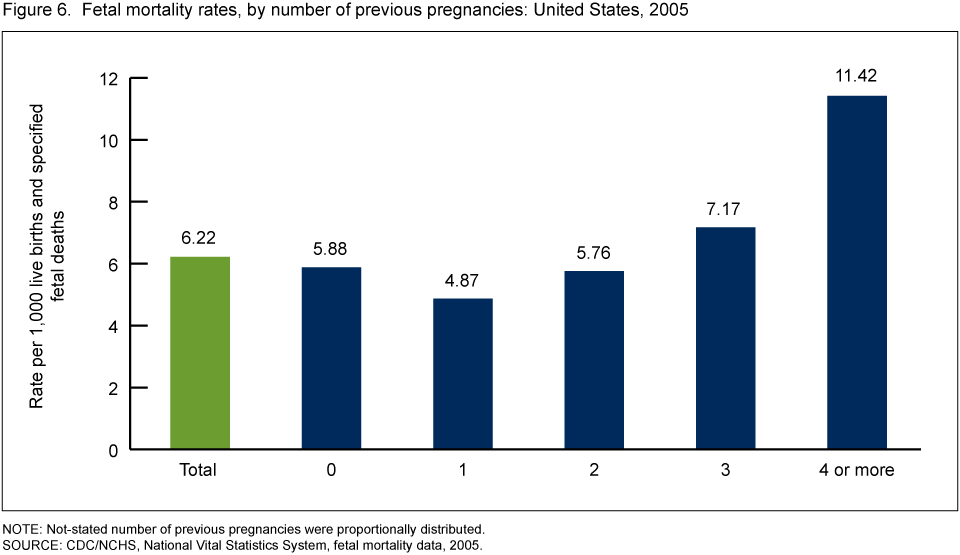
Rates also increased sharply for women with two or more prior pregnancies. Compared with women who had one prior pregnancy, fetal mortality rates were 18% higher for women with two prior pregnancies, 47% higher for women with three prior pregnancies, and 134% higher for women with four or more prior pregnancies. These patterns are consistent with data from other countries (12,13).
Summary
An estimated 1 million fetal deaths at any gestational age occur in the United States each year. After decades of decrease, the U.S. fetal mortality rate (fetal deaths of 20 weeks of gestation or more) did not decline from 2003 to 2005. The 2005 U.S. fetal mortality rate of 6.22 is 52% higher than the Healthy People 2010 target goal of 4.1. There is evidence of underreporting of fetal deaths in the early part of the reporting period (at or near 20 weeks of gestation) (1,3). Still, knowledge of the substantial differences in fetal mortality rates by maternal race and ethnicity, maternal age, single compared with multiple pregnancies, and number of prior pregnancies can help target prevention efforts.
Previously, much of the public health concern regarding reproductive loss was concentrated on infant mortality, in part due to lesser awareness of the magnitude of fetal mortality, its causes, and prevention strategies. However, there is a growing awareness of the effect of fetal mortality on U.S. families. NCHS is working to improve the quality of cause-of-fetal-death data from vital statistics, with enhanced quality control for data as well as an automated coding system under development. The National Institute of Child Health and Human Development is sponsoring the Stillbirth Collaborative Research Network, a major multicenter research study into the causes and prevention of fetal death (14). The Centers for Disease Control and Prevention has initiated active surveillance of fetal deaths in Iowa and Metropolitan Atlanta (15).
Considerable effort has been put into programs aimed at reducing infant mortality in the United States, with sometimes limited results. Prevention of fetal mortality may represent a previously underutilized opportunity to improve perinatal health.
Definitions
Fetal death: Death prior to delivery of a product of human conception irrespective of the duration of pregnancy, and which is not an induced termination of pregnancy (1).
Stillbirth: A fetal death that occurs later in pregnancy (at 20 weeks of gestation or more, or 28 weeks or more, for example).
Fetal mortality rate: Number of fetal deaths per 1,000 live births and fetal deaths. Rates based on data from NVSS are generally presented for fetal deaths of 20 weeks of gestation or more.
Infant death: Death of a live-born infant before his or her first birthday. Often divided into neonatal death (under 28 days of age) and postneonatal death (28 days to under 1 year of age).
Number of previous pregnancies: The vital statistics fetal death data contain information on the number of previous live births (now living or dead), and the number of previous other pregnancy outcomes (spontaneous or induced losses or ectopic pregnancies). These items are summed to yield the number of previous pregnancies.
Data source and methods
This report contains data from the Fetal Death Data File and Linked Birth/Infant Death Data Set, NVSS. The vital statistics Fetal Death Data File contains information from all Reports of Fetal Death filed in the 50 states, the District of Columbia, and selected U.S. territories. Although reporting requirements for fetal deaths vary somewhat by state, fetal mortality rates from NVSS are generally presented for fetal deaths of 20 weeks of gestation or more (1). Fetal death data from NVSS are available by a wide range of maternal and infant characteristics (1). The Linked Birth/Infant Death Data Set provides information on infant deaths and live births in the United States (5). Fetal Death and Linked Birth/Infant Death data sets are available from the NCHS website.
About the authors
Marian F. MacDorman and Sharon Kirmeyer are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Vital Statistics, Reproductive Statistics Branch.
References
- MacDorman MF, Kirmeyer S. Fetal and perinatal mortality, United States, 2005. National vital statistics reports; vol 57 no 8. Hyattsville, MD: National Center for Health Statistics. 2009.
- American College of Obstetricians and Gynecologists. Management of stillbirth. ACOG Practice Bulletin No 102. Obstet Gynecol 113:748–61. 2009.
- Martin JA, Hoyert DL. The national fetal death file. Semin Perinatol 21:3–11. 2002.
- Ventura SJ, Abma JC, Mosher WD, et al. Estimated pregnancy rates by outcome for the United States, 1990–2004. National vital statistics reports; vol 56 no 15. Hyattsville, MD: National Center for Health Statistics. 2008.
- Mathews TJ, MacDorman MF. Infant mortality statistics from the 2005 period linked birth/infant death data set. National vital statistics reports; vol 57 no 2. Hyattsville, MD: National Center for Health Statistics. 2008.
- MacDorman MF, Mathews TJ. Recent trends in infant mortality in the United States. NCHS data brief, no 9. Hyattsville, MD: National Center for Health Statistics. 2008.
- U.S. Department of Health and Human Services. Healthy People 2010, 2nd ed. With: Understanding and improving health, Objectives for improving health; Volumes I and II. Washington, DC: U.S. Government Printing Office. November 2000.
- Vintzileos AM, Ananth CV, Smulian JC, et al. Prenatal care and black-white fetal death disparity in the United States: Heterogeneity by high-risk conditions. Obstet Gynecol 99:483–9. 2002.
- Goldenberg RL, Kirby R, Dulhane JF. Stillbirth: A review. J Matern Fetal Neonatal Med 16:79–94. 2004.
- Wright VC, Chang J, Jeng G, Macaluso M. Assisted reproductive technology surveillance, United States, 2005. MMWR 57(SS-5): 1–23. 2008.
- Bateman BT, Simpson LL. Higher rate of stillbirth at the extremes of reproductive age: A large nationwide sample of deliveries in the United States. Am J Obstet Gynecol 194:840–5. 2006.
- Huang DY, Usher RH, Kramer MS, et al. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol 95:215–21. 2000.
-
Golding J. Epidemiology of fetal and neonatal death. In: Keeling, JW (Ed.). Fetal and Neonatal Pathology, 3rd edition, 175–90. London:
Springer-Verlag. 2001. - Silver RM, Verner MW, Reddy U, et al. Work-up of stillbirth: A review of the evidence. Am J Obstet Gynecol 196:433–44. 2007.
- Duke W, Williams L, Correa A. Using active birth defects surveillance programs to supplement data on fetal death reports: Improving surveillance data on stillbirths. Birth Defects Res A Clin Mol Teratol 82:799-804. 2008.
Suggested citation
MacDorman M, Kirmeyer S. The challenge of fetal mortality. NCHS data brief, no 16. Hyattsville, MD: National Center for Health Statistics. 2009.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Director
Edward J. Sondik, Ph.D.
Acting Co-Deputy Directors
Jennifer H. Madans, Ph.D.
Michael H. Sadagursky