Trends in Allergic Conditions Among Children: United States, 1997–2011
- Key findings
- The prevalence of food and skin allergies increased in children aged 0–17 years from 1997–2011.
- Younger children were more likely to have skin allergies, while older children were more likely to have respiratory allergies.
- Hispanic children had lower rates of all three types of allergies compared with children of other race or ethnicities. Non-Hispanic black children were more likely to have skin allergies and less likely to have respiratory allergies compared with non-Hispanic white children.
- The prevalence of food and respiratory allergy, but not skin allergy, increased with higher income levels.
- Summary
- Definitions
- Data source and methods
- About the author
- References
- Suggested citation
Number 121, May 2013
PDF Version (444 KB)
Kristen D. Jackson, M.P.H.; LaJeana D. Howie, M.P.H., C.H.E.S.; Lara J. Akinbami, M.D.
Key findings
Data from the National Health Interview Survey, 1997–2011
- The prevalence of food and skin allergies increased in children under age 18 years from 1997–2011.
- The prevalence of skin allergies decreased with age. In contrast, the prevalence of respiratory allergies increased with age.
- Hispanic children had a lower prevalence of food allergy, skin allergy, and respiratory allergy compared with children of other race or ethnicities. Non-Hispanic black children were more likely to have skin allergies and less likely to have respiratory allergies compared with non-Hispanic white children.
- Food and respiratory allergy prevalence increased with income level. Children with family income equal to or greater than 200% of the poverty level had the highest prevalence rates.
Allergic conditions are among the most common medical conditions affecting children in the United States (1–5). An allergic condition is a hypersensitivity disorder in which the immune system reacts to substances in the environment that are normally considered harmless (6,7). Food or digestive allergies, skin allergies (such as eczema), and respiratory allergies (such as hay fever) are the most common allergies among children. Allergies can affect a child’s physical and emotional health and can interfere with daily activities, such as sleep, play, and attending school (8,9). A severe allergic reaction with rapid onset, anaphylaxis, can be life threatening. Foods represent the most common cause of anaphylaxis among children and adolescents (10,11). Early detection and appropriate interventions can help to decrease the negative impact of allergies on quality of life (6). This report presents recent trends in the prevalence of allergies and differences by selected sociodemographic characteristics for children under age 18 years.
Keywords: allergy, National Health Interview Survey
The prevalence of food and skin allergies increased in children aged 0–17 years from 1997–2011.
Among children aged 0–17 years, the prevalence of food allergies increased from 3.4% in 1997–1999 to 5.1% in 2009–2011. The prevalence of skin allergies increased from 7.4% in 1997–1999 to 12.5% in 2009–2011. There was no significant trend in respiratory allergies from 1997–1999 to 2009–2011, yet respiratory allergy remained the most common type of allergy among children throughout this period (17.0% in 2009–2011). Skin allergy prevalence was also higher than food allergy prevalence for each period from 1997–2011 (Figure 1).
Figure 1. Percentage of children aged 0–17 years with a reported allergic condition in the past 12 months: United States, 1997–2011
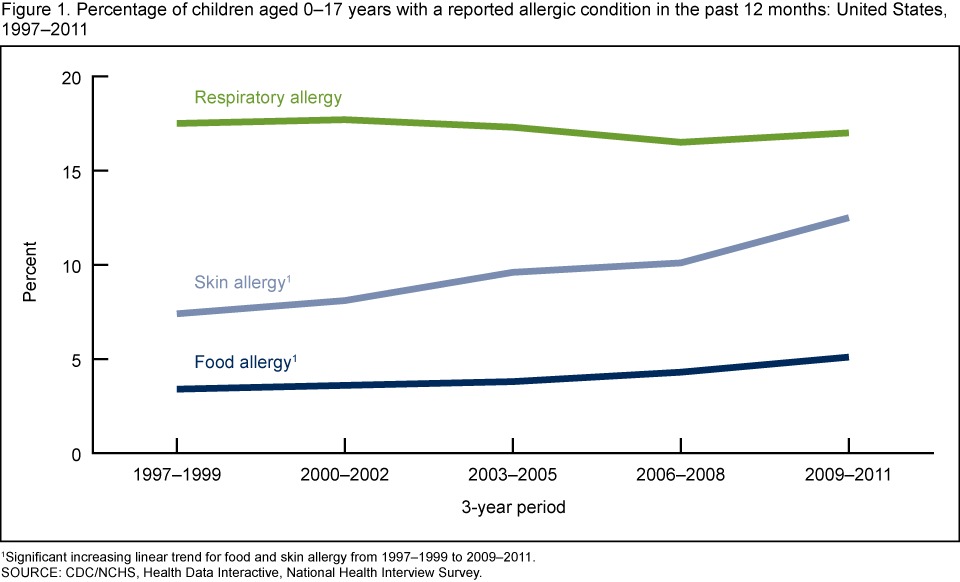
1Significant increasing linear trend for food and skin allergy from 1997–1999 to 2009–2011.
SOURCE: CDC/NCHS, Health Data Interactive, National Health Interview Survey.
Younger children were more likely to have skin allergies, while older children were more likely to have respiratory allergies.
Food allergy prevalence was similar among all age groups. Skin allergy prevalence decreased with the increase of age (14.2% among 0–4 years, 13.1% among 5–9 years, and 10.9% among 10–17 years); while respiratory allergy prevalence increased with the increase of age (10.8% among 0–4 years, 17.4% among 5–9 years, and 20.8% among 10–17 years) (Figure 2).
Figure 2. Percentage of children aged 0–17 years with a reported allergic condition in the past 12 months, by age group: United States, average annual 2009–2011
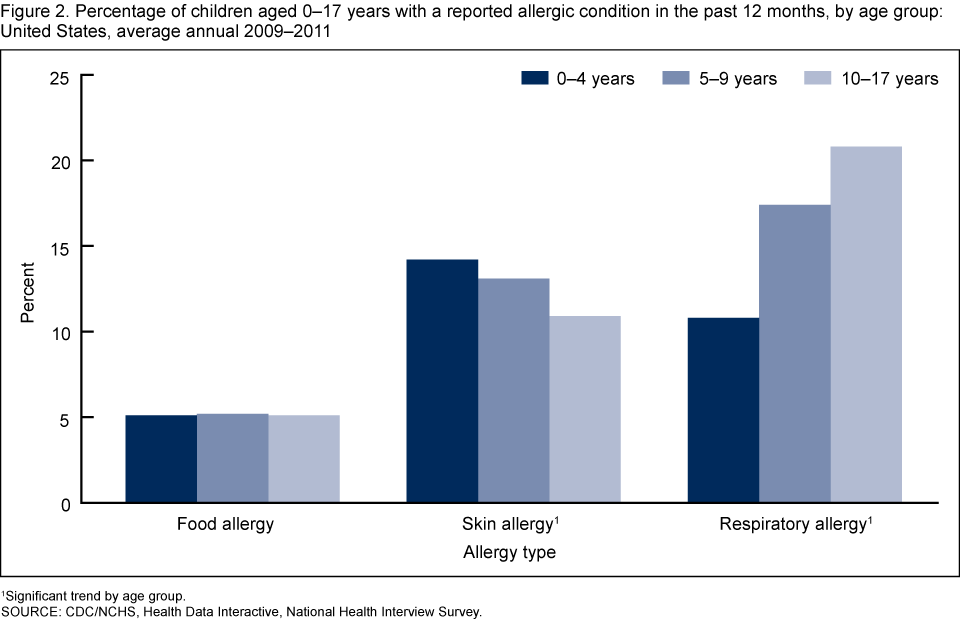
1Significant trend by age group.
SOURCE: CDC/NCHS, Health Data Interactive, National Health Interview Survey.
Hispanic children had lower rates of all three types of allergies compared with children of other race or ethnicities. Non-Hispanic black children were more likely to have skin allergies and less likely to have respiratory allergies compared with non-Hispanic white children.
Hispanic children had a lower prevalence of food allergy (3.6%), skin allergy (10.1%), and respiratory allergy (13.0%) compared with non-Hispanic white and non-Hispanic black children. Non-Hispanic black children had a higher percentage of reported skin allergy (17.4%) compared with non-Hispanic white children (12.0%) and a lower percentage of respiratory allergy (15.6%) compared with non-Hispanic white children (19.1%) (Figure 3).
Figure 3. Percentage of children aged 0–17 years with a reported allergic condition in the past 12 months, by race and ethnicity: United States, average annual 2009–2011
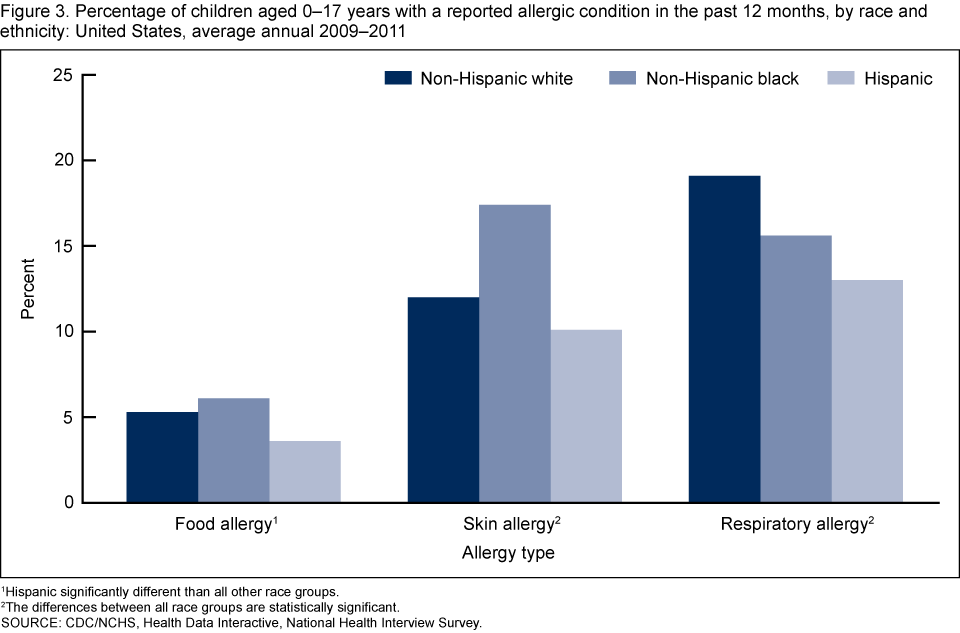
1Hispanic significantly different than all other race groups.
2The differences between all race groups are statistically significant.
SOURCE: CDC/NCHS, Health Data Interactive, National Health Interview Survey.
The prevalence of food and respiratory allergy, but not skin allergy, increased with higher income levels.
The prevalence of both food allergy and respiratory allergy increased with the increase of income level. Among children with family income less than 100% of the poverty level, 4.4% had a food allergy and 14.9% had a respiratory allergy. Food allergy prevalence among children with family income between 100% and 200% of the poverty level was 5.0%, and respiratory allergy prevalence was 15.8%. Among children with family income above 200% of the poverty level, food allergy prevalence was 5.4%, and respiratory allergy prevalence was 18.3%. There was no significant difference in the prevalence of skin allergy by poverty status (Figure 4).
Figure 4. Percentage of children aged 0–17 years with a reported allergic condition in the past 12 months, by poverty status: United States, average annual 2009–2011
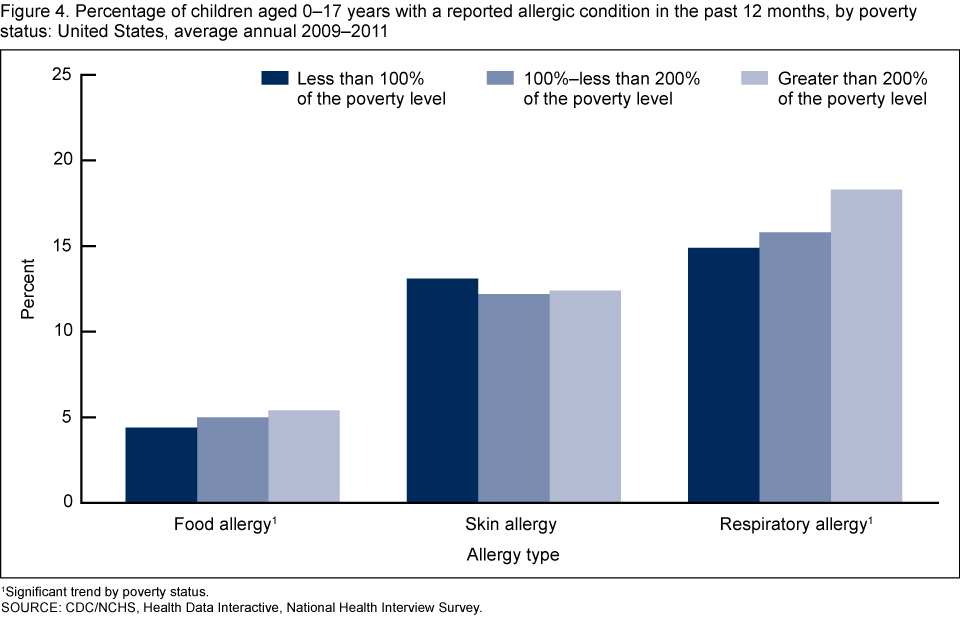
1Significant trend by poverty status.
SOURCE: CDC/NCHS, Health Data Interactive, National Health Interview Survey.
Summary
Among children under age 18 years in the United States, the prevalence of food and skin allergies increased from 1997–1999 to 2009–2011. The prevalence of respiratory allergy, which is the most prevalent type of allergy among children, did not change during this period. There was no significant difference in food allergy prevalence between age groups. However, skin allergy decreased with the increase of age, and respiratory allergy increased with the increase of age. The prevalence of allergies varies by race and ethnicity, with Hispanic children having the lowest prevalence of food, skin, and respiratory allergies compared with non-Hispanic white and non-Hispanic black children. Non-Hispanic black children were more likely to have skin allergies and less likely to have respiratory allergies compared with non-Hispanic white children. The prevalence of allergies differed by poverty status. Food allergy and respiratory allergy increased with the increase of income level, but there was no difference in the prevalence of skin allergy by poverty status.
Definitions
Respiratory allergy prevalence: Estimated based on affirmative responses to either of the two National Health Interview Survey (NHIS) question(s): “During the past 12 months, has your child had hay fever?” and “During the past 12 months, has your child had any kind of respiratory allergy?”
Food allergy prevalence: Estimated based on an affirmative response to the NHIS question: “During the past 12 months, has your child had any kind of food or digestive allergy?”
Skin allergy prevalence: Estimated based on an affirmative response to the NHIS question: “During the past 12 months, has your child had eczema or any kind of skin allergy?”
Poverty status: Based on family income, family size, and the number of children in the family; and for families with two or fewer adults, on the age of the adults in the family. The poverty level is based on a set of income thresholds that vary by family size and composition. Families or individuals with income below their appropriate thresholds are classified as below the poverty level. These thresholds are updated annually by the U.S. Census Bureau to reflect changes in the Consumer Price Index for all urban consumers (12). Estimates by poverty status from NHIS are based on both reported and imputed family income (13).
Data source and methods
Prevalence estimates for allergic conditions were obtained from the Health Data Interactive (HDI) table, “Allergic conditions, ages 0–17: U.S., 1997–2011,” available from the Health Data Interactive website. NHIS data were used to estimate the prevalence of allergic conditions for this HDI table.
NHIS data are collected continuously throughout the year for the Centers for Disease Control and Prevention’s National Center for Health Statistics by interviewers from the U.S. Census Bureau. NHIS collects information about the health and the health care of the civilian noninstitutionalized U.S. population. Interviews are conducted in respondents’ homes, but follow-ups to complete the interviews may be conducted over the telephone. The Sample Child component collects detailed data on health conditions for a randomly selected child in households with at least one child. All of the data in the Sample Child component are obtained from a proxy respondent and not from medical records. A responsible adult, usually a parent, responds to the survey questions as proxy for the sample child. For further information about NHIS and the questionnaire, visit the NHIS website.
NHIS is designed to yield a sample that is representative of the civilian noninstitutionalized population of the United States, and the survey uses weighting to produce national estimates. Data weighting procedures are described in more detail elsewhere (14). Point estimates and estimates of corresponding variances for the HDI estimates were calculated using SUDAAN software (15) to account for the complex sample design of NHIS. The Taylor series linearization method was chosen for variance estimation.
Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. Terms such as “higher” and “lower” indicate statistically significant differences. Terms such as “no difference” indicate that the statistics being compared were not significantly different. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not significant. All estimates shown in this report have a relative standard error less than or equal to 30%. The significance of trends was tested using weighted least squares regression models of the log of each outcome and Joinpoint software (16) to determine whether an apparent change over time was statistically significant, taking into account the standard error for each data point. Because there were limited data points over the period, linear regression (zero joinpoints) was specified for all models.
About the author
Kristen D. Jackson, LaJeana D. Howie, and Lara J. Akinbami are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Office of Analysis and Epidemiology.
References
- Friedman AH, Morris TL. Allergies and anxiety in children and adolescents: A review of the literature. J Clin Psychol Med Settings 13(3):318–31. 2006.
- Gupta RS, Springston EE, Smith B, Kim JS, Pongracic JA, Wang X, Holl J. Food allergy knowledge, attitudes, and beliefs of parents with food-allergic children in the United States. Pediatr Allergy Immunol 21(6):927–34. 2010.
- Vassallo MF, Banerji A, Rudders SA, Clark S, Mullins RJ, Camargo CA Jr. Season of birth and food allergy in children. Ann Allergy Asthma Immunol 104(4):307–13. 2010.
- Akinbami LJ, Moorman JE, Garbe PL, Sondik EJ. Status of childhood asthma in the United States, 1980–2007. Pediatrics 123 Suppl 3:S131–45. 2009.
- Mailhol C, Lauwers-Cances V, Rancé F, Paul C, Giordano-Labadie F. Prevalence and risk factors for allergic contact dermatitis to topical treatment in atopic dermatitis: A study in 641 children. Allergy 64(5):801–6. 2009.
- Stone KD. Atopic diseases of childhood. Curr Opin Pediatr 14(5):634–46. 2002.
- Muraro A, Roberts G, Clark A, Eigenmann PA, Halken S, Lack G. The management of anaphylaxis in childhood: Position paper of the European Academy of Allergology and Clinical Immunology. Allergy 62(8):857–71. 2007.
- Baiardini I, Braido F, Brandi S, Canonica GW. Allergic diseases and their impact on quality of life. Ann Allergy Asthma Immunol 97(4):419–28. 2006.
- Marklund B, Ahlstedt S, Nordstrom G. Health-related quality of life among adolescents with allergy-like conditions—with emphasis on food hypersensitivity. Health Qual Life Outcomes 2:65. 2004.
- De Silva IL, Mehr SS, Tey D, Tang ML. Paediatric anaphylaxis: A 5 year retrospective review. Allergy 63(8):1071–6. 2008.
- Lee JK, Vadas P. Anaphylaxis: Mechanisms and management. Clin Exp Allergy 41(7):923–38. 2011.
- U.S. Census Bureau. Poverty. 2012.
- Schenker N, Raghunathan TE, Chiu PL, et al. Multiple imputation of family income and personal earnings in the National Health Interview Survey: Methods and examples. Hyattsville, MD: National Center for Health Statistics. 2010.
- Botman SL, Moore TF, Moriarity CL, Parsons VL. Design and estimation for the National Health Interview Survey, 1995–2004. National Center for Health Statistics. Vital Health Stat 2(130). 2000.
- SUDAAN, release 9.1 [computer software]. Research Triangle Park, NC: RTI International. 2004.
- Joinpoint Regression Program, version 3.4 [computer software]. Bethesda, MD: National Institutes of Health, National Cancer Institute. 2010.
Suggested citation
Jackson KD, Howie LD, Akinbami LJ. Trends in allergic conditions among children: United States, 1997–2011. NCHS data brief, no 121. Hyattsville, MD: National Center for Health Statistics. 2013.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S. Acting Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemology
Irma E. Arispe, Ph.D., Director