Healthy People 2000 Progress Review
Immunizations and Infectious Diseases
Date: December 1, 1999
Time: 2-4:00 p.m. EST
This progress review will be broadcast on the Public Health Training Network. Details on how to review the broadcast are provided on the Public Health Training Network home page.
Dr. David Satcher, Assistant Secretary for Health and Surgeon General, will be joined by a panel of experts representing the public and private health sectors. Dr. Walt Orenstein, Director, National Immunization Program, Centers for Disease Control and Prevention (CDC); Dr. James Hughes, Director, National Center for Infectious Diseases, Centers for Disease Control and Prevention (CDC); and Dr. Edward Sondik, Director, National Center for Health Statistics, Centers for Disease Control and Prevention (CDC) will review progress toward the targets for the objectives in priority area 20 of Healthy People 2000, Immunizations and Infectious Diseases. The meeting will 1) provide a progress review of Healthy People 2000 objectives on Immunization and Infectious Diseases; 2) offer an opportunity for those gathered in participating states to discuss key issues with Dr. Satcher and the panel; and, 3) explore actions that might be taken in your state to reduce the incidence of infectious diseases, including those preventable through vaccination, during the next decade.
The primary objectives of this meeting are to:
- Assess progress made in achieving the Healthy People 2000 objectives for immunization and infectious diseases.
- Highlight effective programs that impacted on progress and barriers that have hindered improvement.
- Gain an understanding of how these national objectives are translated into opportunities for action.
Data Section
- Summary tables [PDF – 29 KB]
- Summary tables [PDF – 29 KB]
- Individual objective tables
Presentation
Dr. Edward J. Sondik
Director, National Center for Health Statistics
Control of infections to prevent disease and death is one of the major achievements in public health for the 20th century. As we have been successful against many of the major killers of past centuries, other agents emerge and methods of transmission morph to present new challenges. Immunizations are one of the most effective methods of preventing the spread of infectious diseases. And there have been many other successful strategies–from practicing safe sex to washing your hands.
There are 19 objectives in this Healthy People 2000 priority area. We’ve met two objectives and are moving in the right direction for five more. Even more objectives are showing mixed progress, however for these objectives, most of the news is good. Three objectives are moving away from the target. And we still cannot assess progress in two objectives. It’s only by having the full range of data on all objectives that we can truly monitor the program and redirect–or redouble–efforts where needed. The Healthy People 2010 chapter is making positive strides in this direction.
Perhaps nothing has been more important for ensuring the health of children than building a consensus and making the childhood immunization series universally recommended and widely available. As you can see, all vaccinations show similar trends and have made significant progress over the decade. Healthy People 2000 set a target of 90 percent for these basic immunizations.

The National Immunization Survey shows us that as of 1998, 92 percent of children 19-35 months received the vaccination against measles, mumps, and rubella–called MMR.
For polio, the level is at 91 percent.
Newer recommendations call for four immunizations against DTP. …we fell below 90 percent for the fourth dose of DTP.
We’ve reached the target for three immunizations against DTP, with 96-percent coverage in 1998.
While monitoring the individual vaccines gives us the best way of determining the risk of the population to individual vaccine-preventable diseases, it’s important to determine how many children have received the recommended combined series of four DTP, three polio, and one MMR immunizations. While much progress has been made, at 81 percent in 1998, we are still below the target.

For Healthy People 2010 childhood immunization coverage has been expanded and targets established for three doses of the vaccine for Haemophilus influenzae, type b (Hib3) as well as the introduction of three doses of Hepatitis B vaccine.
This chart shows the remarkable improvement during the 1990’s to exceed the 90-percent target for Hib.
And 87 percent to move close to the target for hepatitis B.
The recently introduced immunization against varicella is only slightly over 40 percent but has more than doubled in just 2 years.
As I mentioned, Healthy People 2000 set a target of 90 percent for childhood immunizations for the four DTP, three polio, one MMR series. Looking across the United States, we see that Connecticut has met the target (shown in brown) but that many other States (shown in dark green) fall slightly or substantially below the target. Remember that each percentage point below target represents hundreds of thousands of children who have not received all the recommended doses.
Now let’s turn our attention to the outcome of immunizations as measured in the number of cases of vaccine-preventable diseases. The number of cases differ for each disease, but after an initial surge in the early 1990’s, all except pertussis, have declined dramatically. We’ve made the greatest progress in reducing the number of cases of measles and mumps, nearing the targets set. On the other hand, for pertussis the number of cases has more than doubled over the decade, reaching more than 7,400 cases in 1998. Not shown on this table, diphtheria remains at its baseline level of one case, tetanus has increased from three cases in 1988 to nine in 1998. Polio eradication efforts remain successful with no cases reported since baseline.
The importance of immunization coverage for different diseases is important–so are disparities between racial/ethnic groups. Immunizations and infectious diseases is one of the major areas addressed in the Department of Health and Human Services Initiative to eliminate disparities in health. As we can see in this slide on MMR vaccination coverage, minimal disparities exist among young children. However, we will see that this is not the case for adults.
As this next slides shows, when adolescents and young adults serve as a reservoir for transmission of diseases like pertussis, there isn’t always a clear cause and effect between vaccination coverage in the young preschool population and overall disease incidence. As we noted earlier, cases of pertussis climbed steadily throughout the 1990’s, in this chart using data from CDC’s National Notifiable Disease Surveillance System.
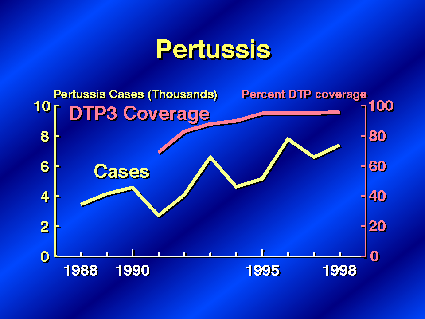
These increases in disease occurred despite increases in DTP vaccination coverage rates among 19 to 35-month-old children, suggesting better control of this disease may require vaccines that can be administered to adolescents and young adults.
Turning to immunizations for older Americans, the year 2000 target for influenza immunizations is 60 percent. The overall influenza immunization coverage rate of 63 percent in 1997 exceeds the target. Despite this progress, the rate for Non-Hispanic whites was almost 50 percent higher than that of non-Hispanic African Americans in 1997. The Hispanic population’s rate also remains considerably below the target.
For pneumococcal vaccinations, progress has been slower. All groups fall short of this target but again significant disparities exist. Older whites are twice as likely as both African American and Hispanic persons to get an immunization once in their lifetime. The cause of these low rates is not entirely clear. The lower pneumococcal coverage in comparison to influenza immunization levels may be attributed to less familiarity by physicians as well as patients with the recommendations. In addition, individuals may be less informed of their vaccination status. We see this as a data challenge and are exploring alternate data sources to collect this information.
Epidemic-related pneumonia and influenza deaths are those that occur above and beyond the normal yearly fluctuations of mortality. Because of the extreme variability in epidemic-related deaths from year to year, they are analyzed in 3-year moving averages. Data from the National Vital Statistics System show rates that fluctuate but have moved toward the target for the last few years.
In summary, immunization coverage for many diseases for both children and adults are moving toward the targets. With a few important exceptions, vaccine-preventable diseases have been reduced. However, as the elderly population continues to increase, vaccinations against influenza and pneumonia will be more important than ever. Thank you. Dr. Satcher.
Infectious Disease Data Highlights
I am pleased to report that there has been significant progress in reducing the scope and impact of infectious diseases.
Over the past decade, cases of bacterial meningitis have plummeted far below the target. And the drop in the rate of cases among Alaska Natives–a group targeted at high risk–has been even more pronounced.
There’s been a significant decline in hepatitis B and C to exceed the targets, shown by the green and yellow dots on the right. And while the rate of cases of hepatitis A has also declined, it is still above its target, shown in pink.

Two population groups were targeted for special efforts to reduce hepatitis A. There has been remarkable progress in reducing the incidence rate among American Indians. The rate dropped from its peak of 364 to 30 per 100,000 in 1998. Among Hispanics the rate declined by 24 percent but the rate is still considerably above its target, shown in green.

For hepatitis B, many special targets were set for those at higher risk. In recent years there has been progress in reducing the number of cases in each of the groups you see tracked on this table. The targets have been reached for all groups except Asian/Pacific Islander children. This objective illustrates the success of a variety of prevention strategies utilized for each population group.
There’s been progress in reducing the rate of hepatitis C infections. We see a bounce up again in 1996, which may reflect the difficulty to measure this infection among specific population groups. Or annual variability may be at play. Later data will be useful to clarify the trend.
Now, we turn our attention to another aspect of the fight against infectious disease, antimicrobial resistance. It’s ironic–but well recognized–that the very efforts to prevent or treat some conditions may result in those methods or medicines becoming ineffective and the disease becoming an even greater threat. There are also infections that are acquired in the process of obtaining medical care.
For all but low-risk surgical patients, the wound infection rate has dropped significantly to exceed the targets. This is true particularly for high-risk patients, for whom the rate has been cut in half. These data from the National Nosocomial Infection Surveillance System provide current data to monitor infections among intensive care patients.
2010 hopes to curb the use of antibiotic prescriptions for the common cold prescriptions, which offer little for that condition but later render the patient susceptible to diseases now resistant to those same antibiotics. The baseline data from the National Ambulatory Medical Care Survey (or NAMCS for short) show a rate of over 2,500 prescriptions per 100,000 population. The target for 2010 would reduce use by half.
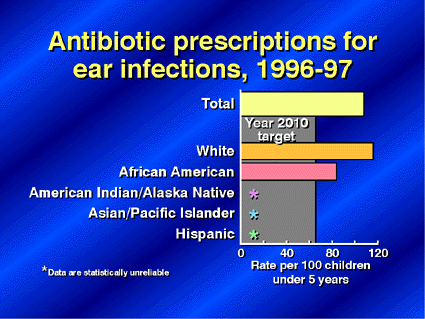
The situation is similar with regard to treating ear infections among children. NAMCS baseline data show antibiotic prescription rates for whites are 38 percent higher than for blacks. For the total, 108 antibiotic prescriptions for ear infections per 100,000 children far exceeds the target of 65 prescriptions per 100,000 set for 2010.
Efforts to control tuberculosis have been impacted by antimicrobial resistance. TB case rates had been decreasing for many decades until the late 1980’s when the rates began to increase. Although TB has decreased after peaking in the mid 1990’s, the goal of 3.5 cases per 100,000 is unlikely to be reached. The resurgence of TB in the late 1980’s was due to related outbreaks in correctional facilities and hospitals, the HIV epidemic, imported cases from immigrants from TB-endemic areas, and the occurrence of difficult to treat multidrug-resistant TB.
There’s been little change in the percent of TB patients who complete treatment. Assuring the completion of preventive therapy is an important method of preventing active disease in persons with latent TB infections.
There was not time today to cover all of the objectives in this area; however, all the data and charts presented are available at the NCHS web page. Data include other objectives–such as removing financial barriers to immunization–or reducing rates of illness in group settings or during international travel. These topics, and more, will also be addressed in Healthy People 2010.
- Office of Disease Prevention and Health Promotion Healthy People 2000 Web Page
- National Immunization Program
- National Center for Infectious Diseases
- National Center for HIV, STD, and TB Prevention
- National Association for County and City Health Officials Data Systems
- National Immunization Survey
- National Vital Statistics System
- National Health Interview Survey
- National Nursing Home Survey