Antidepressant Use in Persons Aged 12 and Over: United States, 2005–2008
- Key findings
- About one in 10 Americans aged 12 and over takes antidepressant medication.
- Non-Hispanic white persons are more likely to take antidepressant medication than persons of other races and ethnicities.
- Females are more likely than males to take antidepressant medication at every level of depression severity.
- About 14% of Americans taking antidepressant medication have done so for 10 years or longer.
- Less than one-third of persons taking a single antidepressant have seen a mental health professional in the past year.
- Summary
- Definitions
- Data sources and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 76, October 2011
PDF Version (768 KB)
Laura A. Pratt, Ph.D.; Debra J. Brody, M.P.H.; and Qiuping Gu, M.D., Ph.D.
Key findings
Data from the National Health and Nutrition Examination Surveys, 2005–2008
- Eleven percent of Americans aged 12 years and over take antidepressant medication.
- Females are more likely to take antidepressants than are males, and non-Hispanic white persons are more likely to take antidepressants than are non-Hispanic black and Mexican-American persons.
- About one-third of persons with severe depressive symptoms take antidepressant medication.
- More than 60% of Americans taking antidepressant medication have taken it for 2 years or longer, with 14% having taken the medication for 10 years or more.
- Less than one-third of Americans taking one antidepressant medication and less than one-half of those taking multiple antidepressants have seen a mental health professional in the past year.
Antidepressants were the third most common prescription drug taken by Americans of all ages in 2005–2008 and the most frequently used by persons aged 18–44 years (1). From 1988–1994 through 2005–2008, the rate of antidepressant use in the United States among all ages increased nearly 400% (1).
This data brief discusses all antidepressants taken, regardless of the reason for use. While the majority of antidepressants are taken to treat depression, antidepressants also can be taken to treat anxiety disorders, for example. The report describes antidepressant use among Americans aged 12 and over, including prevalence of use by age, sex, race and ethnicity, income, depression severity, and length of use.
Keywords: prescription medication, depression, National Health and Nutrition Examination Survey, mental health
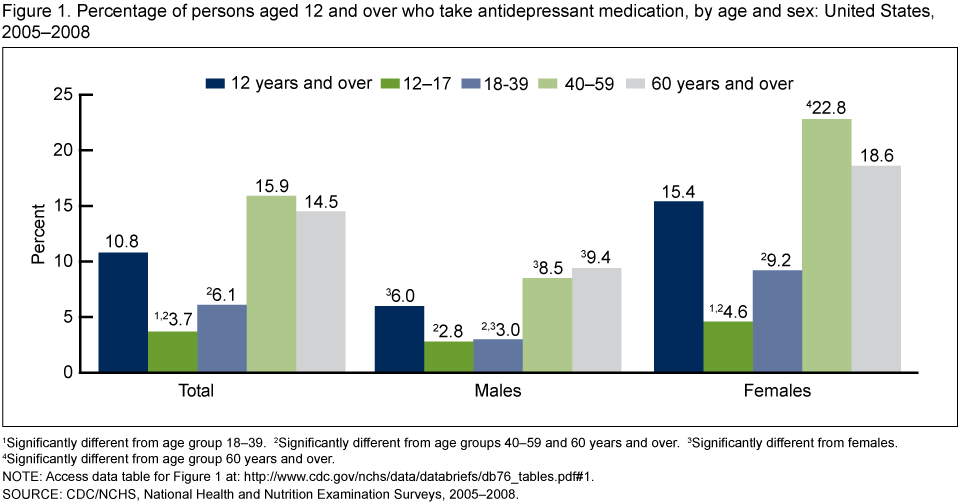
About one in 10 Americans aged 12 and over takes antidepressant medication.
1 Significantly different from age group 18–39.
2 Significantly different from age groups 40–59 and 60 and over.
3 Significantly different from females.
4 Significantly different from age group 60 and over.
NOTE: Access data table for Figure 1 [PDF – 12 KB]
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005–2008.
- Overall, females are 2½ times as likely to take antidepressant medication as males. However, there is no difference by sex in rates of antidepressant use among persons aged 12–17 (Figure 1).
- Twenty-three percent of women aged 40–59 take antidepressants, more than in any other age-sex group.
- Among both males and females, those aged 40 and over are more likely to take antidepressants than those in younger age groups.
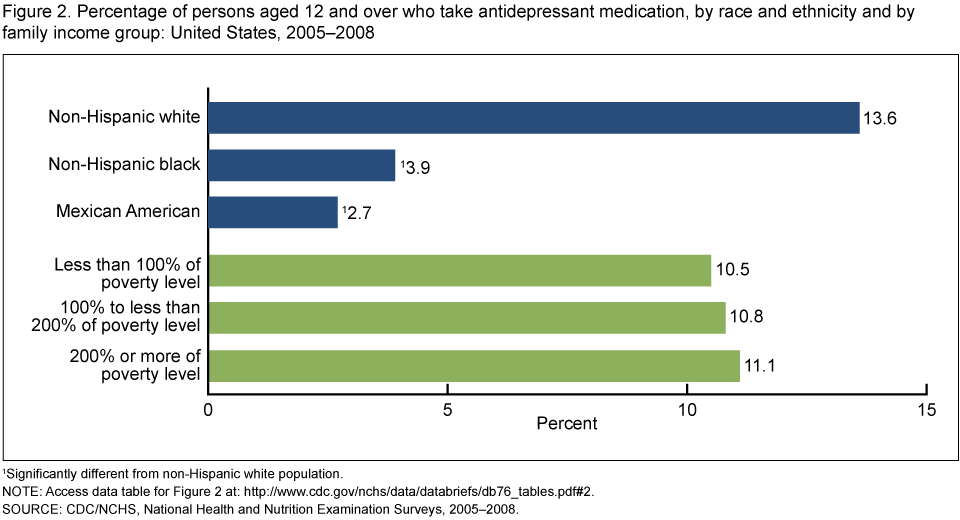
Non-Hispanic white persons are more likely to take antidepressant medication than persons of other races and ethnicities.
1Significantly different from non-Hispanic white population.
NOTE: Access data table for Figure 2 [PDF – 11 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005–2008.
- Fourteen percent of non-Hispanic white persons take antidepressant medications compared with 4% of non-Hispanic black and 3% of Mexican-American persons (Figure 2).
- There is no difference by income in the prevalence of antidepressant usage.
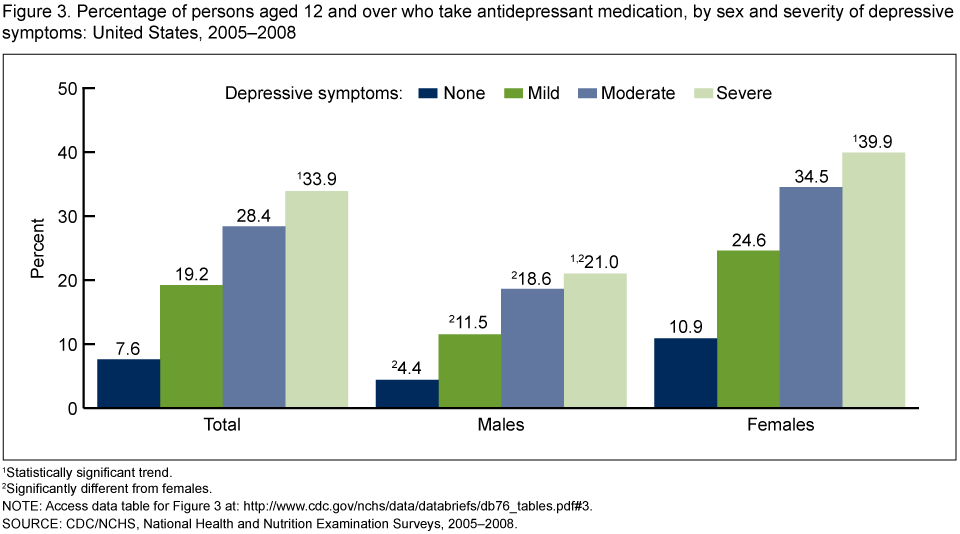
Females are more likely than males to take antidepressant medication at every level of depression severity.
1 Statistically significant trend.
2 Significantly different from females.
NOTE: Access data table for Figure 3 [PDF – 11 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005–2008.
- Overall, 40% of females and 20% of males with severe depressive symptoms take antidepressant medication (Figure 3).
- More than one-third of females with moderate depressive symptoms, and less than one-fifth of males with moderate depressive symptoms, take antidepressant medication.
- Use of antidepressant medication rises as severity of depressive symptoms increases among both males and females.
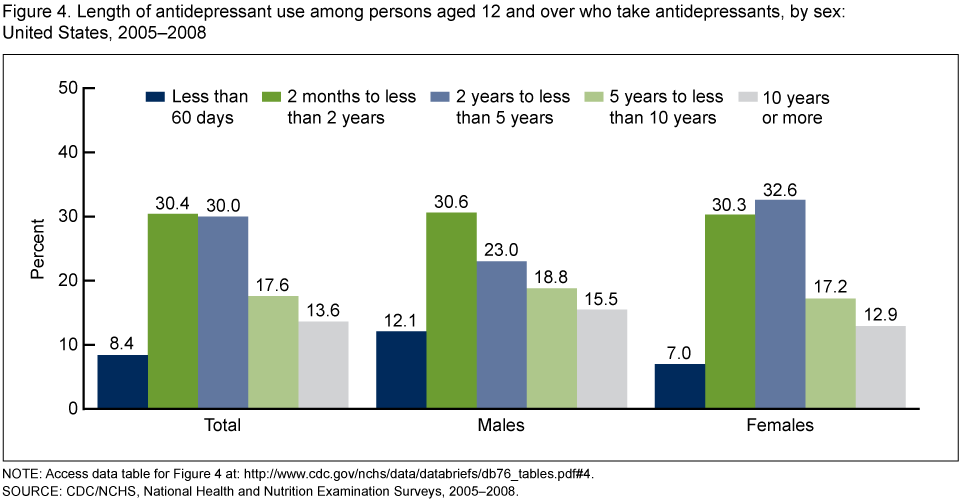
About 14% of Americans taking antidepressant medication have done so for 10 years or longer.
NOTE: Access data table for Figure 4 [PDF – 12 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005–2008.
- More than 60% of Americans taking antidepressant medication have been taking it longer than 2 years (Figure 4).
- In general, there was no significant difference between males and females in length of use of antidepressants.
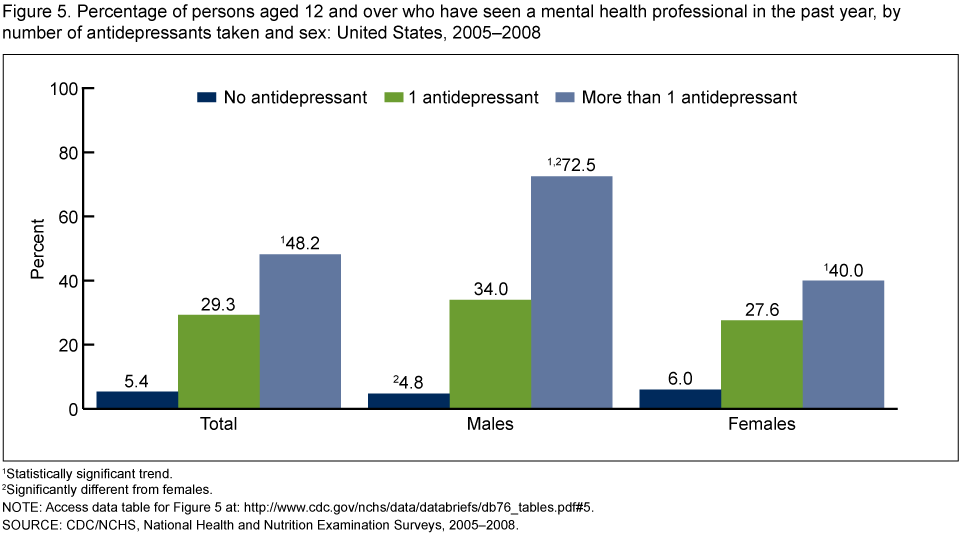
Less than one-third of persons taking a single antidepressant have seen a mental health professional in the past year.
1 Statistically significant trend.
2 Significantly different from females.
NOTE: Access data table for Figure 5 [PDF – 11 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Surveys, 2005–2008.
- Among persons taking antidepressants, approximately 14% take more than one antidepressant; the percentage was similar for males and females (data not shown).
- Less than one-half of persons taking multiple antidepressants have seen a mental health professional in the past year (Figure 5).
- Among those taking multiple antidepressants, males are more likely than females to have seen a mental health professional in the past year.
- The likelihood of having seen a mental health professional increases as the number of antidepressants taken increases.
Summary
In 2005–2008, 11% of Americans aged 12 and over took antidepressant medication. There were significant differences in antidepressant medication usage rates between groups. Females were 2½ times as likely as males to take antidepressants. Antidepressant use was higher in persons aged 40 and over than in those aged 12–39. Non-Hispanic white persons were more likely to take antidepressants than other race and ethnicity groups. Other studies have shown similar age, gender, and race and ethnicity patterns (2,3). There was no variation in antidepressant use by income group. Among persons taking antidepressants overall, there was no significant difference in length of use between males and females. Among persons taking antidepressants, males were more likely than females to have seen a mental health professional in the past year.
About 8% of persons aged 12 and over with no current depressive symptoms took antidepressant medication. This group may include persons taking antidepressants for reasons other than depression and persons taking antidepressants for depression who are being treated successfully and do not currently have depressive symptoms.
Slightly over one-third of persons aged 12 and over with current severe depressive symptoms were taking antidepressants. According to American Psychiatric Association guidelines, medications are the preferred treatment for moderate to severe depressive symptomatology (4). The public health importance of increasing treatment rates for depression is reflected in Healthy People 2020, which includes national objectives to increase treatment for depression in adults and treatment for mental health problems in children (5).
Definitions
Prescription drug use: National Health and Nutrition Examination Survey (NHANES) participants were asked if they had taken a prescription drug in the past month. Those who answered “yes” were asked to show the interviewer the medication containers of all prescription drugs. For each drug reported, the interviewer recorded the product’s complete name from the container.
Antidepressant medication: Prescription drugs were classified based on the three-level nested therapeutic classification scheme of Cerner Multum’s Lexicon (6). Antidepressants were identified using the second level of drug categorical codes, specifically code 249.
Income group: Defined by dividing family income by a poverty threshold based on the size of the family. Income groups included less than 100% of the poverty level, 100% to less than 200% of the poverty level, and 200% or more of the poverty level.
Severity of depressive symptoms: Measured in NHANES using the Patient Health Questionnaire (PHQ–9), a nine-item screener that asks questions about the frequency of symptoms of depression over the past 2 weeks (7). PHQ–9 is based on the diagnostic criteria for a major depressive episode in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (8). Major depression includes mood symptoms such as feelings of sadness or irritability, loss of interest in usual activities, inability to experience pleasure, feelings of guilt or worthlessness, and thoughts of death or suicide; cognitive symptoms such as inability to concentrate and difficulty making decisions; and physical symptoms such as fatigue, lack of energy, feeling restless or slowed down, and changes in sleep, appetite, and activity levels.
In PHQ–9, the response categories “not at all,” “several days,” “more than half the days,” and “nearly every day” are given a score ranging from 0 (not at all) to 3 (nearly every day). A total score is calculated ranging from 0 to 27. The following four categories of depressive symptom severity are based on the total score from the PHQ–9 screening instrument (7):
- None or minimal: 0–4
- Mild: 5–9
- Moderate: 10–14
- Severe: 15 or more
Length of use of antidepressants: Evaluated by asking participants how long they had been taking the medication. Among persons taking more than one antidepressant, the one they had taken the longest was used for Figure 4.
Contact with a mental health professional: Defined by the question: “During the past 12 months, have you seen or talked to a mental health professional such as a psychologist, psychiatrist, psychiatric nurse, or clinical social worker about your health?”
The data do not indicate whether persons who contacted a mental health professional actually began treatment for depression. The question also does not ask about mental health treatment received from primary care providers.
Data sources and methods
NHANES is a continuous survey conducted to assess the health and nutrition of Americans. The survey is designed to be nationally representative of the U.S. civilian noninstitutionalized population. Survey participants complete a household interview and visit a mobile examination center (MEC) for a physical examination and private interview. The annual interview and examination sample includes approximately 5,000 persons of all ages. In 2005–2006, non-Hispanic black persons, Mexican-American persons, adults aged 60 and over, and low-income persons were oversampled to improve the statistical reliability of the estimates for these groups. In 2007–2008, the same groups were oversampled with one exception: Rather than oversampling only the Mexican-American population, all Hispanic persons were oversampled.
This report is based on the analysis of data from interviews in the household and in the MEC. The questions on prescription drug use were asked in the household interview, and the questions on depression were asked in the MEC. Questions were administered in English and Spanish.
Of the 13,897 persons aged 12 and over who participated in the NHANES medical examination, analyses for this data brief included 12,637 persons with information on medication usage and depression severity. Estimates by income group were based on 11,827 persons who also reported their family income.
NHANES sample examination weights, which account for the differential probabilities of selection, nonresponse, and noncoverage, were used for all analyses. Standard errors of the percentages were estimated using Taylor series linearization, a method that incorporates the sample design and weights.
Overall differences between groups were evaluated using the chi square statistic. In cases where the chi square test was significant, differences between subgroups were evaluated using the univariate t statistic. A test for trends was done to evaluate changes in the estimates by depression severity in Figure 3 and by number of antidepressants taken in Figure 5. All significance tests were two-sided using p < 0.05 as the level of significance, with no adjustment for multiple comparisons. All comparisons reported are statistically significant unless otherwise indicated. Data analyses were performed using SAS version 9.2 (SAS Institute, Cary, N.C.) and SUDAAN version 9.0 (RTI International, Research Triangle Park, N.C.).
About the authors
Laura A. Pratt is with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Office of Analysis and Epidemiology. Debra J. Brody and Qiuping Gu are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health and Nutrition Examination Surveys.
References
- National Center for Health Statistics. Health, United States, 2010: With special feature on death and dying. Table 95. Hyattsville, MD. 2011.
- Olfson M, Marcus SC. National patterns in antidepressant medication treatment. Arch Gen Psychiatry 66(8):848–56. 2009.
- Paulose-Ram R, Safran MA, Jonas BS, Gu Q, Orwig D. Trends in psychotropic medication use among U.S. adults. Pharmacoepidemiol Drug Saf 16(5):560–70. 2007.
- American Psychiatric Association. Practice guideline for treatment of patients with major depressive disorder, third edition. Washington, DC. 2010.
- U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020 summary of objectives: Mental health and mental disorders.
- Multum Lexicon database. In: National Health and Nutrition Examination Survey—1988–2008 data documentation, codebook, and frequencies. 2010.
- Kroenke K, Spitzer RL, Williams JB. The PHQ–9: Validity of a brief depression severity measure. J Gen Intern Med 16(9):606–13. 2001.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, fourth edition. Washington, DC. 2000.
Suggested citation
Pratt LA, Brody DJ, Gu Q. Antidepressant use in persons aged 12 and over: United States, 2005–2008. NCHS data brief, no 76. Hyattsville, MD: National Center for Health Statistics. 2011.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemiology
Diane M. Makuc, Dr.P.H., Acting Director
Division of Health and Nutrition Examination Surveys
Clifford L. Johnson, M.S.P.H., Director