Trends and Characteristics in Maternal Syphilis Rates During Pregnancy: United States, 2016–2022
NCHS Data Brief No. 496, February 2024
PDF Version (539 KB)
Elizabeth C.W. Gregory, M.P.H., and Danielle M. Ely, Ph.D.
- Key findings
- The rate of maternal syphilis increased from 2016 through 2022.
- Maternal syphilis rates increased for all maternal race and Hispanic-origin groups from 2016 through 2022.
- Maternal syphilis rates increased for all maternal age groups from 2016 through 2022.
- Maternal syphilis rates increased for all prenatal care categories from 2016 through 2022.
- Maternal syphilis rates increased in most states from 2016–2017 to 2021–2022.
Data from the National Vital Statistics System
- The overall rate of syphilis in mothers giving birth in the United States more than tripled from 2016 to 2022, rising from 87.2 to 280.4 per 100,000 births.
- The syphilis rate increased for all maternal race and Hispanic-origin groups from 2016 through 2022; the largest increase was for American Indian and Alaska Native non-Hispanic mothers (from 159.7 to 1,410.5 per 100,000 births).
- The syphilis rate increased for all maternal age groups from 2016 through 2022, with the largest increase for mothers younger than age 20 (from 107.3 to 418.6 per 100,000 births).
- For 2016–2022, the syphilis rate increased for all prenatal care categories.
- The syphilis rate increased from 2016–2017 to 2021–2022 in 47 states and the District of Columbia.
After reaching historic lows in 2000 and 2001, rates of primary and secondary syphilis in the overall U.S. population have increased nearly every year through 2022 (1). For 2017–2022, rates of syphilis for women of reproductive age and congenital syphilis (a disease that occurs when a mother with syphilis passes the infection on to her baby during pregnancy) increased by more than 250% (1,2). Congenital syphilis can cause adverse pregnancy outcomes such as fetal and neonatal death, low birthweight, preterm birth, and brain and nerve disorders (2). This report presents trends in maternal syphilis rates in women giving birth in the United States for 2016–2022 by selected maternal demographic and health factors.
Keywords: STDs, race and Hispanic origin, National Vital Statistics System
The rate of maternal syphilis increased from 2016 through 2022.
- The rate of maternal syphilis increased 222% from 2016 to 2022, from 87.2 to 280.4 per 100,000 births (Figure 1).
- Annual rates increased each year during this period, ranging from 15% from 2017 (101.3) to 2018 (116.7) to 32% from 2021 (212.6) to 2022 (280.4).
Figure 1. Maternal syphilis rate: United States, 2016–2022
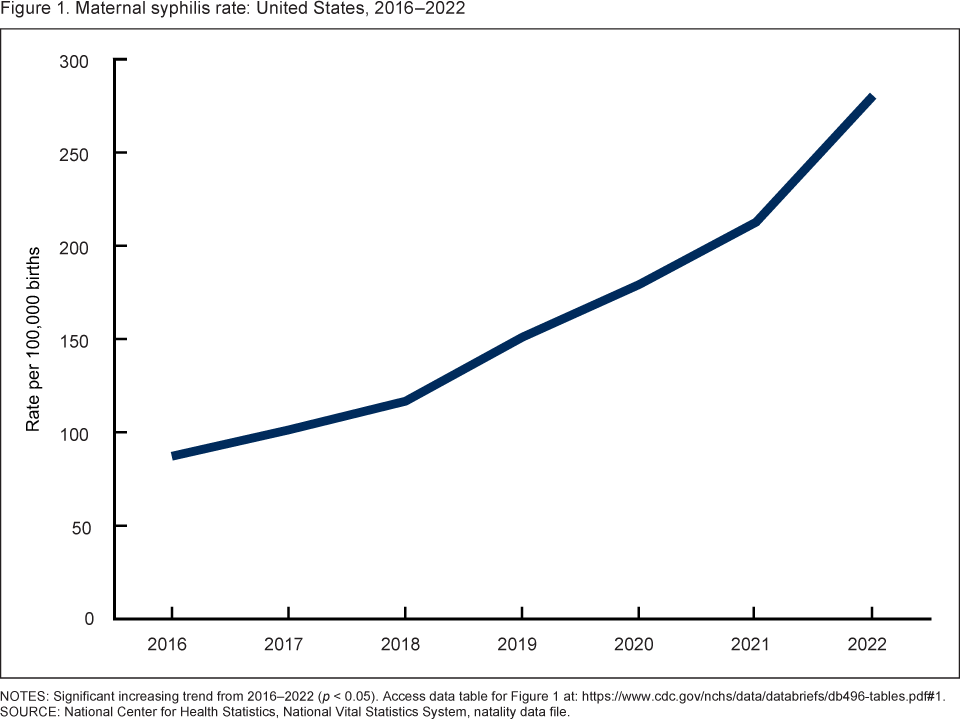
NOTES: Significant increasing trend from 2016–2022 (p < 0.05). Access data table for Figure 1.
SOURCE: National Center for Health Statistics, National Vital Statistics System, natality data file.
Maternal syphilis rates increased for all maternal race and Hispanic-origin groups from 2016 through 2022.
- From 2016 through 2022, the rate of maternal syphilis rose for each race and Hispanic-origin group (Figure 2).
- The largest increases occurred for American Indian and Alaska Native non-Hispanic (subsequently, American Indian and Alaska Native) mothers (783%, from 159.7 to 1,410.5 per 100,000 births), followed by White non-Hispanic (subsequently, White) (315%, from 36.8 to 152.8), and Hispanic (243%, from 91.5 to 313.8) mothers.
- Syphilis rates also increased for Black non-Hispanic (subsequently, Black) (149%, from 274.8 to 684.7), Asian non-Hispanic (subsequently, Asian) (92%, from 38.2 to 73.3), and Native Hawaiian or Other Pacific Islander non-Hispanic (subsequently, Native Hawaiian or Other Pacific Islander) (48%, from 482.2 to 713.4) mothers.
- Although patterns by race and Hispanic origin changed over the period, in 2022, the syphilis rate was highest for American Indian and Alaska Native mothers, followed by Native Hawaiian or Other Pacific Islander and Black (difference not statistically significant), Hispanic, White, and Asian mothers.
Figure 2. Maternal syphilis rate, by race and Hispanic origin of mother: United States, 2016–2022
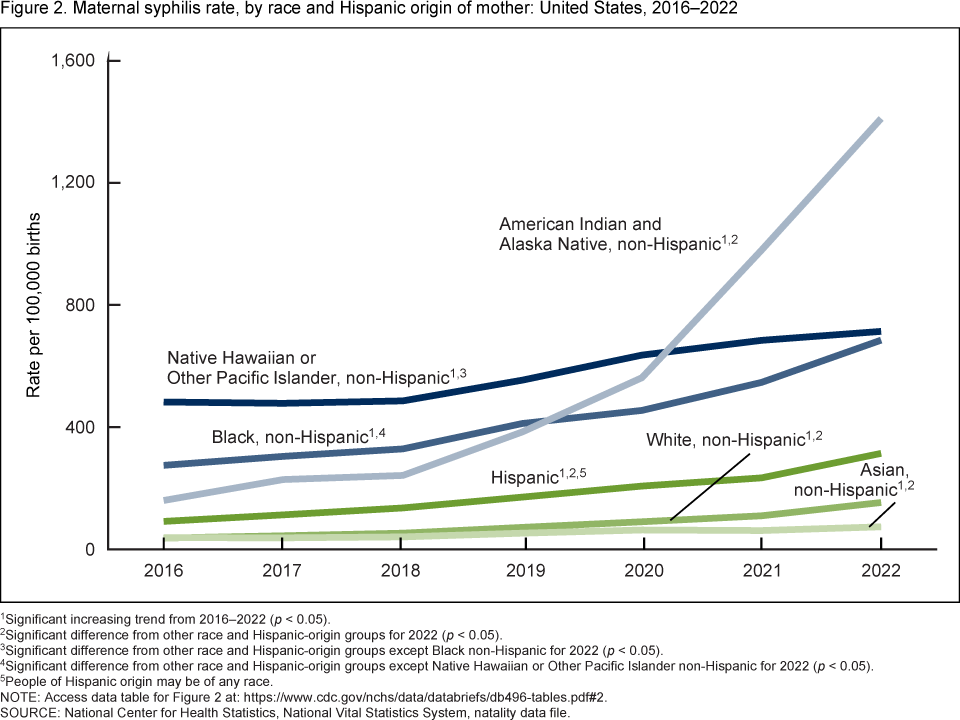
1Significant increasing trend from 2016–2022 (p < 0.05).
2Significant difference from other race and Hispanic-origin groups for 2022 (p < 0.05).
3Significant difference from other race and Hispanic-origin groups except Black non-Hispanic for 2022 (p < 0.05).
4Significant difference from other race and Hispanic-origin groups except Native Hawaiian or Other Pacific Islander non-Hispanic for 2022 (p < 0.05).
5People of Hispanic origin may be of any race.
NOTE: Access data table for Figure 2.
SOURCE: National Center for Health Statistics, National Vital Statistics System, natality data file.
Maternal syphilis rates increased for all maternal age groups from 2016 through 2022.
- From 2016 through 2022, the rate of maternal syphilis rose for each maternal age group (Figure 3).
- During this period, the largest increases were for mothers younger than age 20 (290%, from 107.3 to 418.6 per 100,000 births), followed by mothers ages 30–34 (277%, from 60.9 to 229.6), mothers ages 25–29 (239%, from 88.9 to 301.6) and mothers ages 20–24 (226%, from 122.3 to 398.1).
- Syphilis rates also increased for mothers ages 35–39 (163%, from 76.5 to 201.5) and mothers ages 40 and older (116%, from 91.1 to 196.7).
- By 2022, the syphilis rate was highest for mothers in age groups younger than age 25 and decreased with increasing maternal age.
Figure 3. Maternal syphilis rate, by age group: United States, 2016–2022
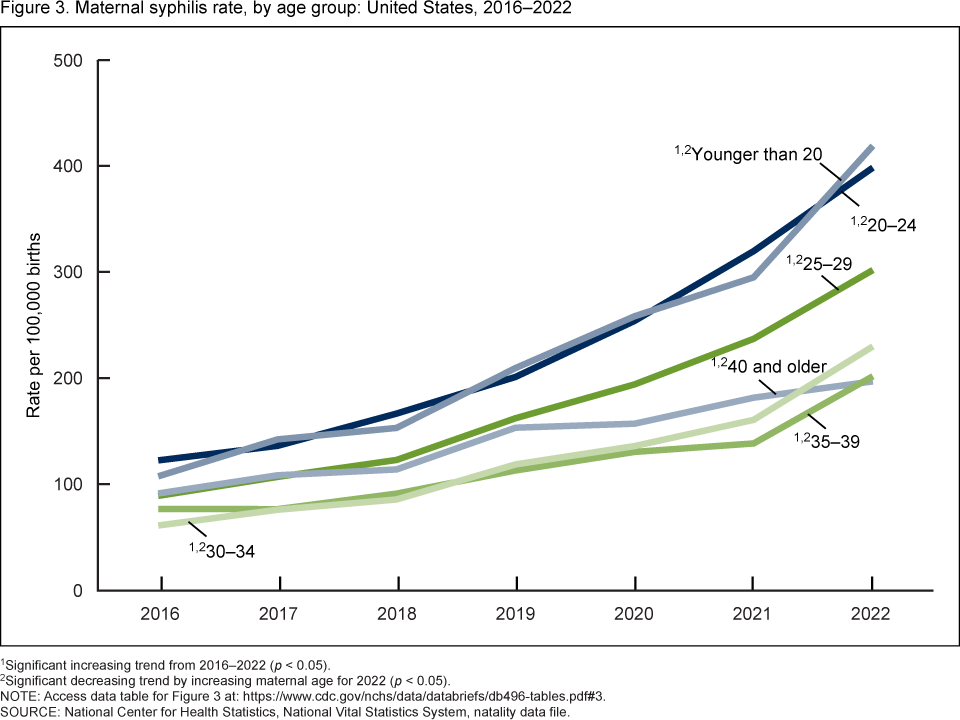
1Significant increasing trend from 2016–2022 (p < 0.05).
2Significant decreasing trend by increasing maternal age for 2022 (p < 0.05).
NOTE: Access data table for Figure 3.
SOURCE: National Center for Health Statistics, National Vital Statistics System, natality data file.
Maternal syphilis rates increased for all prenatal care categories from 2016 through 2022.
- From 2016 through 2022, the rate of maternal syphilis rose for all mothers regardless of timing or lack of prenatal care (Figure 4).
- The largest increases occurred for mothers with no prenatal care (298%, from 262.5 to 1,044.0 per 100,000 births), followed by mothers who began care in the third trimester (244%, from 167.4 to 576.1), and mothers who began care in the second trimester (240%, from 134.3 to 456.9).
- The syphilis rate also increased for mothers who began care in the first trimester (197%, from 67.9 to 201.8).
- Throughout the period, the syphilis rate was highest for those not receiving prenatal care and decreased with earlier prenatal care initiation.
Figure 4. Maternal syphilis rate, by trimester prenatal care began: United States, 2016–2022
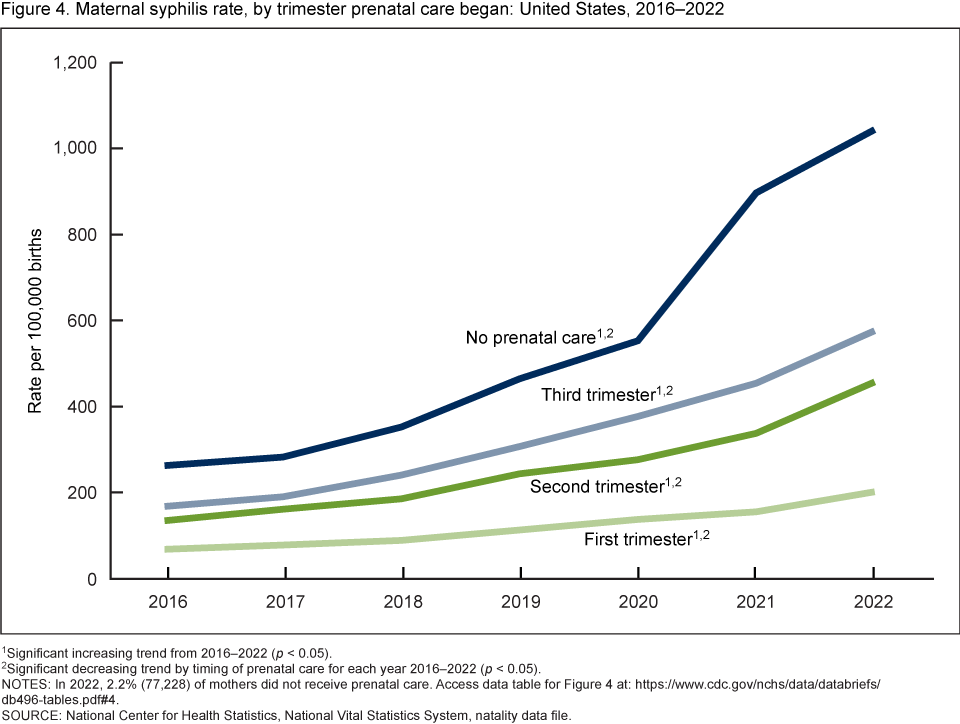
1Significant increasing trend from 2016–2022 (p < 0.05).
2Significant decreasing trend by timing of prenatal care for each year 2016–2022 (p < 0.05).
NOTES: In 2022, 2.2% (77,228) of mothers did not receive prenatal care. Access data table for Figure 4.
SOURCE: National Center for Health Statistics, National Vital Statistics System, natality data file.
Maternal syphilis rates increased in most states from 2016–2017 to 2021–2022.
- The rate of maternal syphilis increased from 2016–2017 to 2021–2022 in 48 of the 51 reporting areas (47 states and the District of Columbia) (Figure 5).
- Compared with 2016–2017, syphilis rates for 2021–2022 were at least 100% higher for 40 states and the District of Columbia; rates rose by more than 400% for 6 states (New Mexico, Colorado, Mississippi, South Dakota, Montana, and Alaska).
- Increases of less than 100% in syphilis rates were seen for seven states (Louisiana, New Jersey, New York, Ohio, Virginia, Idaho, and Utah). There was no significant change for three states (Maine, Vermont, and Wyoming).
- For combined years 2021–2022, the syphilis rate ranged from 45.8 per 100,000 births in Maine to 762.6 in South Dakota.
Figure 5. Maternal syphilis rate, by state for 2021–2022 combined, and change in rate from 2016–2017 combined to 2021–2022: Each state and the District of Columbia
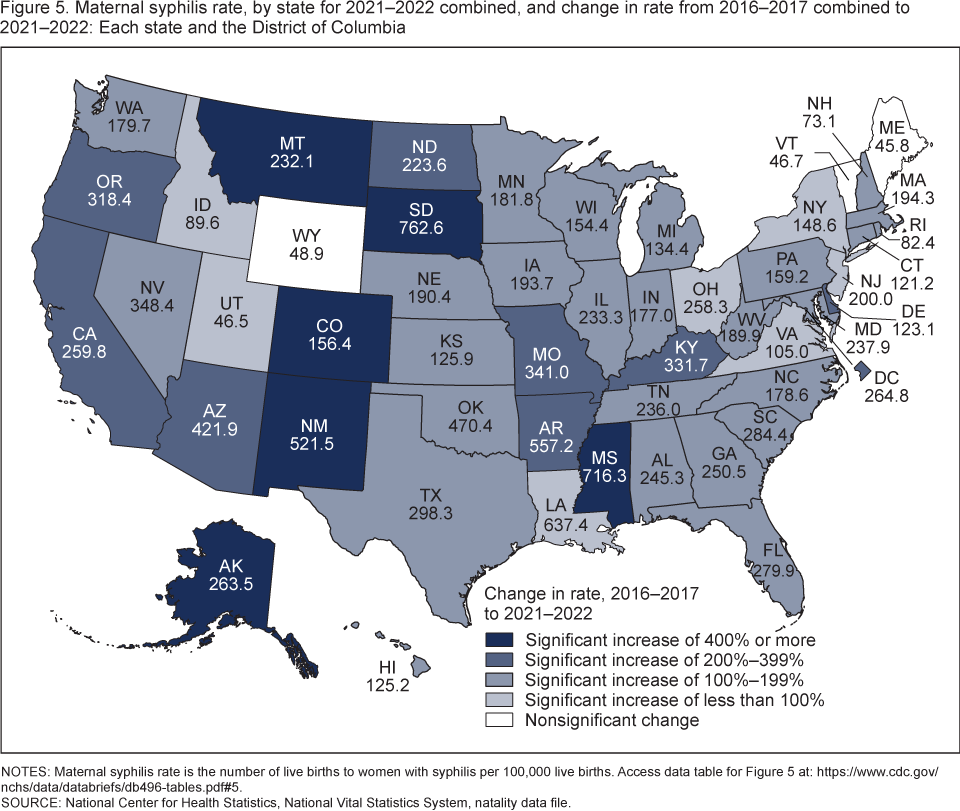
NOTES: Maternal syphilis rate is the number of live births to women with syphilis per 100,000 live births. Access data table for Figure 5.
SOURCE: National Center for Health Statistics, National Vital Statistics System, natality data file.
Summary
From 2016 to 2022, the rate of maternal syphilis rose 222% in the United States, reaching 280.4 per 100,000 births in 2022. Increases in syphilis rates were widespread, rising for all maternal race and Hispanic-origin and age groups, prenatal care categories, and nearly all reporting areas. In 2022, variations in rates were observed across the characteristics studied. Syphilis rates were highest in mothers who were American Indian and Alaska Native, younger than age 25, and had no prenatal care. For 2021–2022, the rate ranged from 45.8 in Maine to 762.6 per 100,000 births in South Dakota.
Definitions
Maternal syphilis: A syphilis infection present at the start of pregnancy or a confirmed diagnosis during pregnancy with or without documentation of treatment (3). Documentation of treatment during this pregnancy is adequate if a definitive diagnosis is not present in the available medical records (3).
Maternal syphilis rate: Number of live births to women with syphilis per 100,000 live births. Although this analysis describes the prevalence of maternal syphilis, the unit of analysis is births.
Trimester prenatal care began: The month prenatal care began is derived from the “Date of first prenatal visit” entry (the item also includes a checkbox for “No prenatal care”) and the gestational age of the newborn based on the obstetric estimate of gestation (4). This item includes a recode for the trimester when prenatal care began. Categories are defined as: first trimester (first to third month), second trimester (fourth to sixth month), third trimester (seventh to final month), and no prenatal care.
Data source and methods
This report uses data from the National Vital Statistics System’s natality data file. The natality file is based on information derived from birth certificates and includes information for all births occurring in the United States (4).
Information on maternal syphilis is recommended to be collected from the mother’s medical records, with the prenatal care record as the preferred source (4). The diagnostic information from the medical records used to report maternal syphilis on the birth certificate is not standardized and may differ from what other data systems use to report syphilis. In 2022, 0.5% of birth records were missing data on maternal syphilis. National information on maternal syphilis became available from the birth certificate for the first time in 2016. The race and Hispanic-origin groups shown follow the 1997 Office of Management and Budget standards (5).
The differences between any rates noted in the text are statistically significant at the 0.05 level unless otherwise noted. References to the decreasing trend for prenatal care categories for each year during 2016–2022 and the decreasing trend for 2022 maternal age categories were statistically significant at the 0.05 level and were assessed using the Cochran–Armitage test for trends, a modified chi-squared test.
References to trends in rates over time were evaluated using the Joinpoint Regression Program (6). A maximum of one joinpoint was allowed during the 2016–2022 period, which is the default setting. The default settings were also selected for the other parameters of the analysis. For details, see reference 7.
Because of the small number of maternal syphilis cases annually by state, data are combined for the years 2016–2017 and 2021–2022 to calculate more reliable state-specific rates.
About the authors
Elizabeth C.W. Gregory and Danielle M. Ely are with the National Center for Health Statistics, Division of Vital Statistics.
References
- Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2022. 2024.
- Centers for Disease Control and Prevention. Congenital syphilis—CDC fact sheet. 2023.
- National Center for Health Statistics. Facility worksheet for the live birth certificate. 2016.
- National Center for Health Statistics. User guide to the 2022 natality public use file. 2023.
- Office of Management and Budget. Revisions to the standards for the classification of federal data on race and ethnicity. Fed Regist 62(210):58782–90. 1997.
- National Cancer Institute. Joinpoint Regression Program (Version 5.0.2) [computer software]. 2023.
- Ingram DD, Malec DJ, Makuc DM, Kruszon-Moran D, Gindi RM, Albert M, et al. National Center for Health Statistics guidelines for analysis of trends. National Center for Health Statistics. Vital Health Stat 2(179). 2018.
Suggested citation
Gregory ECW, Ely DM. Trends and characteristics in maternal syphilis rates during pregnancy: United States, 2016–2022. NCHS Data Brief, no 496. Hyattsville, MD: National Center for Health Statistics. 2024. DOI: https://dx.doi.org/10.15620/cdc:145590.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Brian C. Moyer, Ph.D., Director
Amy M. Branum, Ph.D., Associate Director for Science
Division of Vital Statistics
Paul D. Sutton, Ph.D., Acting Director
Andrés A. Berruti, Ph.D., M.A., Associate Director for Science