Emergency Department Visits for Chest Pain and Abdominal Pain: United States, 1999-2008
- Key findings
- Are ED visits for chest or abdominal pain increasing?
- Is ambulance use increasing among patients complaining of chest or abdominal pain?
- Are chest or abdominal pain visits triaged as immediate or emergent becoming more common?
- Is the use of advanced medical imaging for chest or abdominal pain visits increasing?
- Are visits to the ED for abdominal or chest pain becoming less serious?
- Are patients with chest or abdominal pain becoming more likely to die in the ED, be admitted to the hospital, or be transferred to another facility over time?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 43, September 2010
PDF Version (709 KB)
Farida A. Bhuiya, M.P.H.; Stephen R. Pitts, M.D., M.P.H., F.A.C.E.P.; and Linda F. McCaig, M.P.H., Division of Health Care Statistics
Key findings
Data from the National Hospital Ambulatory Medical Care Survey: 1999-2008
- The number of noninjury emergency department (ED) visits in which abdominal pain was the primary reason for the visit increased 31.8%.
- The percentage of ED visits for which chest pain was the primary reason decreased 10.0%.
- Use of advanced medical imaging increased strongly for ED visits related to abdominal pain (122.6%) and chest pain (367.6%).
- The percentage of ED visits for chest pain that resulted in a diagnosis of acute coronary syndrome decreased 44.9%.
Chest and abdominal pain are the most common reasons that persons aged 15 years and over visit the emergency department (ED) (1). Because EDs provide both emergency and nonemergency care (2,3), visits for these symptoms may vary in their acuity. Advanced medical imaging is often ordered to assist in both diagnosing and ruling out serious illness associated with these symptoms (4,5). This report describes trends in visits for chest and abdominal pain in adults and the seriousness of illness and use of imaging in these visits. All data shown are for persons aged 18 and over whose visit was not injury related.
Keywords: National Hospital Ambulatory Medical Care Survey, advanced medical imaging, reason for visit
Are ED visits for chest or abdominal pain increasing?
From 1999 through 2008, the percentage of noninjury ED visits due to chest pain decreased, while the percentage of noninjury ED visits due to abdominal pain increased (Figure 1).
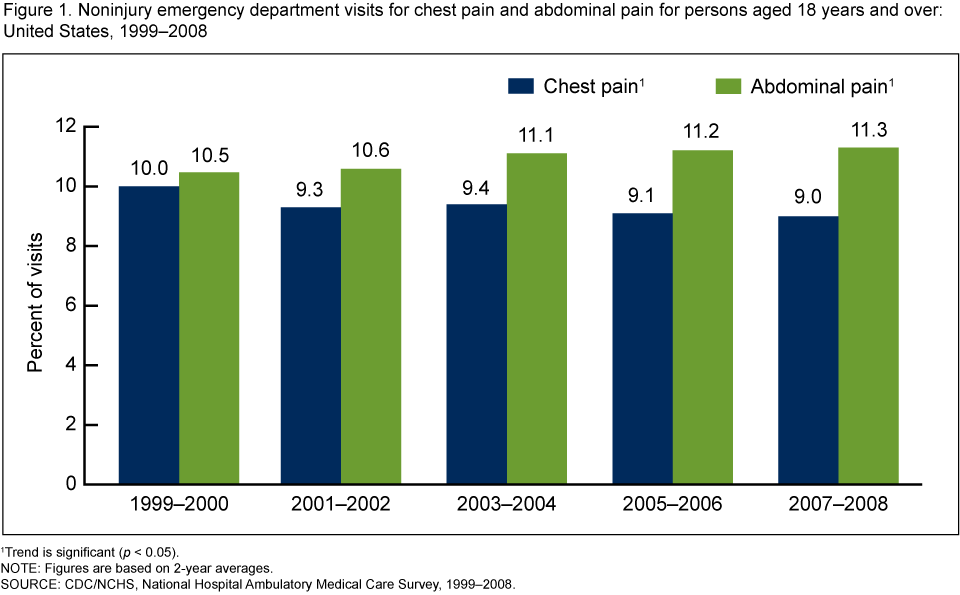
The number of noninjury ED visits rose 22.1%, from 50.5 million in 1999-2000 to 61.7 million in 2007-2008 (not shown).
The number of noninjury ED visits for which abdominal pain was the primary reason increased 31.8%, from 5.3 million in 1999-2000 to 7.0 million in 2007-2008 (not shown). The percentage of ED visits for abdominal pain rose 7.6% during this time.
The number of noninjury ED visits in which chest pain was the primary reason was 5.0 million in 1999-2000 and 5.5 million in 2007-2008, a difference that is not statistically significant. The percentage of ED visits for chest pain decreased 10.0% during this time, from 10.0% to 9.0%.
Is ambulance use increasing among patients complaining of chest or abdominal pain?
The percentage of noninjury ED visits in which patients with abdominal pain arrived by ambulance was 26.9% higher in 2007-2008 than in 1999-2000. No significant difference was observed when comparing percentages of visits for chest pain and arrival by ambulance for the same years (Figure 2).
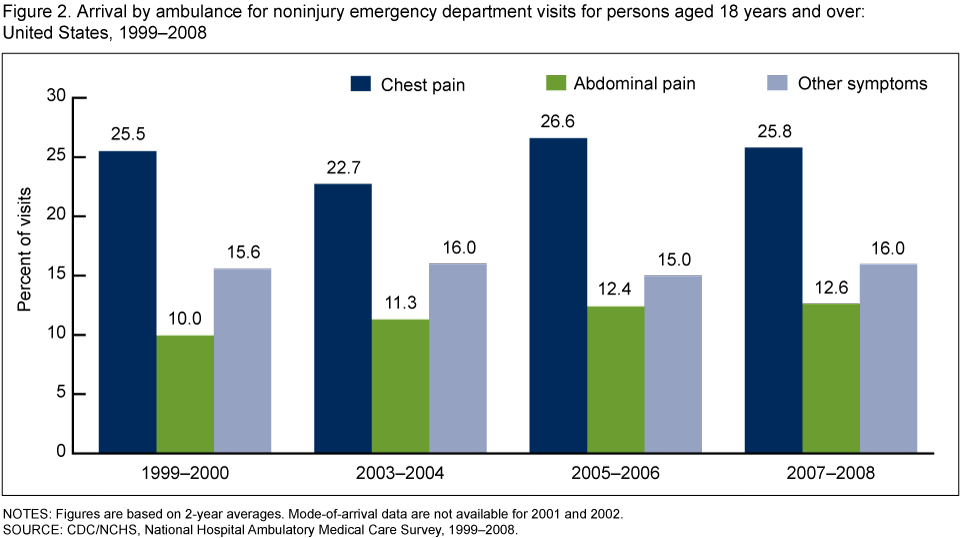
In each time period studied, patients with chest pain were more likely to arrive by ambulance compared with patients having other symptoms. Conversely, patients with abdominal pain were less likely to arrive by ambulance compared with patients having other symptoms.
Are chest or abdominal pain visits triaged as immediate or emergent becoming more common?
Triage level indicates the seriousness of the visit from the perspective of the triage nurse.
From 1999-2000 through 2007-2008, the percentage of chest pain visits triaged as immediate or emergent (i.e., should be seen within 14 minutes) decreased by 12.4%.
The percentage of noninjury ED visits for symptoms other than chest pain or abdominal pain that were triaged as immediate or emergent also decreased, by 6.4% (Figure 3).
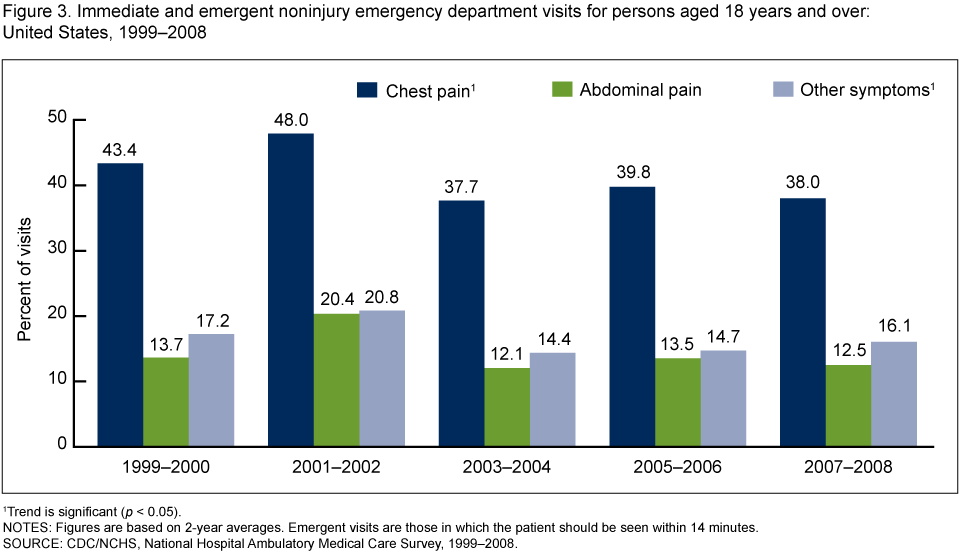
No trend was found for abdominal pain visits triaged as immediate or emergent.
The percentage of chest pain visits that were immediate or emergent was two to three times higher than the percentage of visits for abdominal pain or visits for other symptoms.
Is the use of advanced medical imaging for chest or abdominal pain visits increasing?
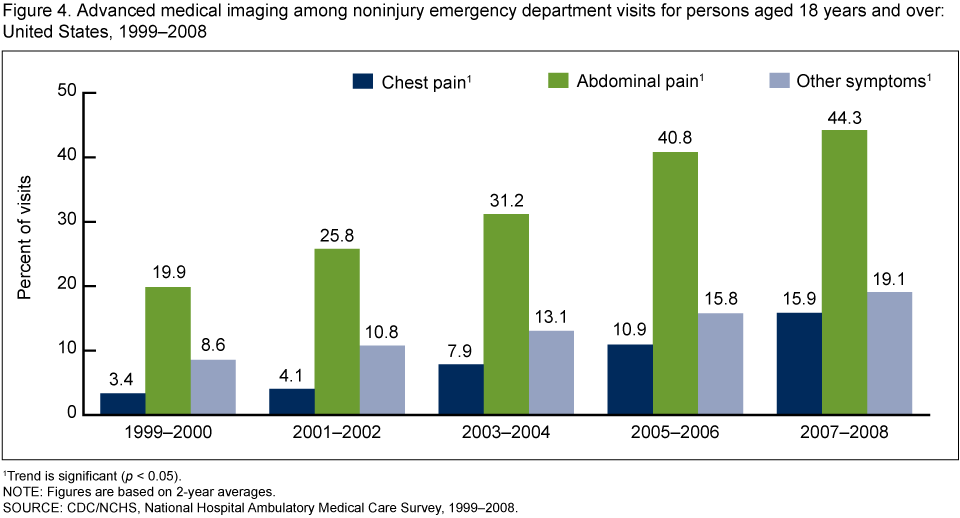
Ordering advanced medical imaging for diagnosis of illness indicates the physician’s perception of the visit’s seriousness.
A trend toward increased use of advanced medical imaging during noninjury ED visits was observed from 1999-2000 through 2007-2008 for chest pain visits (up 367.6%, from 3.4% to 15.9%), abdominal pain visits (up 122.6%, from 19.9% to 44.3%), and all other visits (up 122.1%, from 8.6% to 19.1%) (Figure 4).
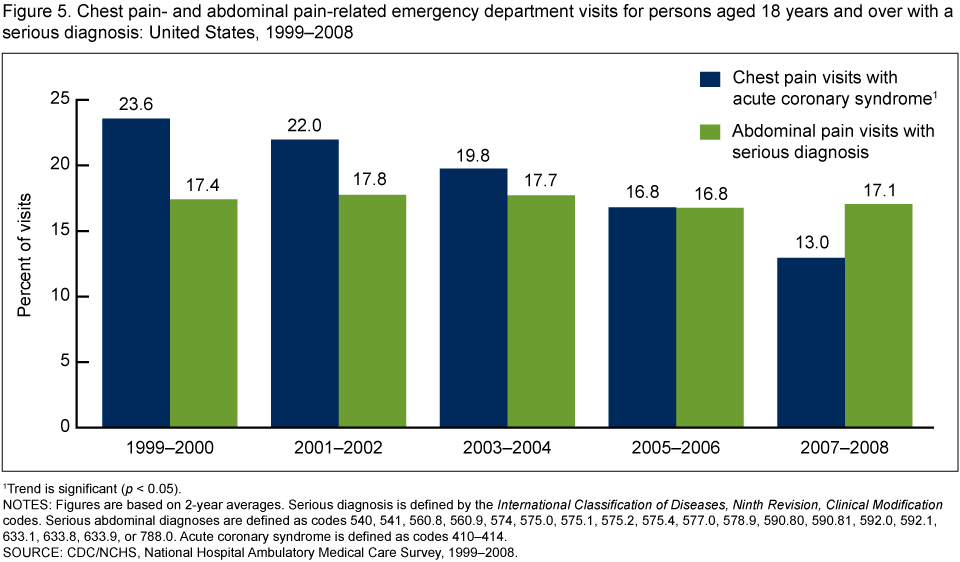
Are visits to the ED for abdominal or chest pain becoming less serious?
The percentage of ED visits for chest pain that resulted in a diagnosis of acute coronary syndrome (ACS) decreased 44.9%, from 23.6% in 1999-2000 to 13.0% in 2007-2008.
During the same time period, no significant change was observed in the percentage of ED visits for abdominal pain that resulted in a serious diagnosis (Figure 5).
Are patients with chest or abdominal pain becoming more likely to die in the ED, be admitted to the hospital, or be transferred to another facility over time?
In each time period studied, patients with chest pain were more likely to die, be admitted to the hospital, or be transferred to another facility compared with visits for abdominal pain or other symptoms (Figure 6).

The percentage of visits for chest pain that resulted in admission, transfer, or death declined 17.2% from 1999-2000 through 2007-2008.
No trend was observed in visits for abdominal pain resulting in admission, transfer, or death during this time.
Summary
The number of noninjury ED visits made by persons aged 18 and over complaining of chest pain or abdominal pain rose from 1999 through 2008, but the proportion of those visits with a serious diagnosis did not increase. In fact, the percentage of visits for chest pain resulting in a diagnosis of ACS decreased, consistent with reported declines in hospitalizations for acute myocardial infarction (4). However, not all indicators of acuity follow the same pattern. Arrival by ambulance increased for abdominal pain visits, while the proportion of visits triaged as immediate or emergent declined for chest pain visits as well as for visits with other symptoms. The proportion of visits in which the patient was admitted to the hospital, transferred to another facility, or died decreased for chest pain visits but remained constant for abdominal pain visits. In contrast, the use of advanced medical imaging increased dramatically for these visits. Advanced imaging may increase the amount of time that a patient spends in the ED, thereby slowing throughput and contributing to ED crowding and its adverse consequences (5–7). However, advanced imaging may help a physician to rule out conditions, thereby avoiding further unnecessary or risky diagnosis and therapy, and it may help confirm certain conditions, thereby leading to more effective and efficient therapy (7,8). Targeted research is needed to clarify the extent to which medical imaging for ED visits for chest or abdominal pain is improving the diagnosis and treatment of serious conditions.
Definitions
Emergency department (ED): A hospital facility that provides unscheduled outpatient services to patients whose conditions require immediate care, which is staffed 24 hours a day. On- and off-site EDs that are open fewer than 24 hours are included if staffed by the hospital.
Emergency department visit: A direct, in-person exchange between a patient seeking ED care and a health care provider.
Patient’s principal reason for visit: Main complaint, symptom, or reason the patient came to the ED, coded according to A Reason for Visit Classification for Ambulatory Care (RVC) (9). Abdominal pain symptoms were defined as stomach and abdominal pain, cramps and spasms (RVC code 1545). Chest pain symptoms were defined as chest pain and related symptoms (RVC code 1050).
Serious diagnosis: Up to three diagnoses coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) (10). Serious abdominal diagnosis was defined as ICD-9-CM codes 540, 541, 560.8, 560.9, 574, 575.0, 575.1, 575.2, 575.4, 577.0, 578.9, 590.80, 590.81, 592.0, 592.1, 633.1, 633.8, 633.9, and 788.0. Acute coronary syndrome was defined as ICD-9-CM codes 410-414.
Advanced medical imaging: Includes computerized tomography or CT scan, magnetic resonance imaging or MRI, and ultrasound technology.
Data source and methods
Data from the 1999-2008 National Hospital Ambulatory Medical Care Survey (NHAMCS) were used for this analysis. NHAMCS is an annual national probability sample survey of nonfederal, general, and short-stay hospitals. It is designed to produce national estimates of visits to EDs and outpatient departments, including statistics on patient demographic characteristics, reasons for visit, diagnoses, services, medications, and disposition.
The ED component of NHAMCS has a multistage design that involves sampling geographic primary sampling units (PSUs), hospitals that have EDs within PSUs, and patient visits within emergency service areas (ESAs). Types of ESAs included general, adult, pediatric, fast track, psychiatric, and trauma. During the study period, approximately 480 hospitals were selected each year, of which about 415 had eligible EDs. Each year, data are collected on about 35,000 ED visits. Data were combined for 2-year periods to provide more reliable estimates. The study excluded injury-related visits.
Data analyses were performed using the statistical packages SAS version 9.2 (SAS Institute, Cary, N.C.) and SUDAAN version 9.0 (Research Triangle Institute, Research Triangle Park, N.C.) A weighted least squares regression analysis was used to determine the significance of trends at the 0.05 level. Terms relating to differences such as “greater than” or “less than” indicate that the difference is statistically significant. A lack of comment regarding the difference does not mean that the difference was tested and found not significant.
About the authors
Farida Bhuiya and Linda McCaig are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health Care Statistics, Ambulatory and Hospital Care Statistics Branch. Stephen Pitts is with Emory University School of Medicine, Department of Emergency Medicine.
References
- Pitts SR, Niska RW, Xu J, Burt CW. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. National health statistics reports; no 7. Hyattsville, MD: National Center for Health Statistics. 2008.
- Institute of Medicine of the National Academies. Future of emergency care: Hospital-based emergency care at the breaking point. Washington, DC: National Academies Press. 2007.
- Northington WE, Brice JH, Zou B. Use of an emergency department by nonurgent patients. Am J Emerg Med 23(2):131-7. 2005.
- Fang J, Alderman MH, Keenan NL, Ayala C. Acute myocardial infarction hospitalization in the United States, 1979 to 2005. Am J Med 123(3):259-66. 2010.
- Gardner RL, Sarkar U, Maselli JH, Gonzales R. Factors associated with longer ED lengths of stay. Am J Emerg Med 25(6):643-50. 2007.
- Pines JM, Pollack CV Jr, Diercks DB, Chang AM, Shofer FS, Hollander JE. The association between emergency department crowding and adverse cardiovascular outcomes in patients with chest pain. Acad Emerg Med 16(7):617-25. 2009.
- Pines JM. Trends in the rates of radiography use and important diagnoses in emergency department patients with abdominal pain. Med Care 47(7):782-6. 2009.
- Gerhardt RT, Nelson BK, Keenan S, Kernan L, MacKersie A, Lane MS. Derivation of a clinical guideline for the assessment of nonspecific abdominal pain: The guideline for abdominal pain in the ED setting (GAPEDS) phase 1 study. Am J Emerg Med 23(6):709-17. 2005.
- Schneider D, Appleton L, McLemore T. A reason for visit classification for ambulatory care. National Center for Health Statistics. Vital Health Stat 2(78). 1979.
- CDC, National Center for Health Statistics and Centers for Medicare & Medicaid Services. International Classification of Diseases, Ninth Revision, Clinical Modification, Sixth Edition. DHHS Pub No. (PHS) 06-1260. 2006.
Suggested citation
Bhuiya F, Pitts SR, McCaig LF. Emergency department visits for chest pain and abdominal pain: United States, 1999-2008. NCHS data brief, no 43. Hyattsville, MD: National Center for Health Statistics. 2010.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Jane E. Sisk, Ph.D., Director