Death Rates Due to Suicide and Homicide Among Persons Aged 10–24: United States, 2000–2017
- Key findings
- After a stable period from 2000 to 2007, suicide rates for persons aged 10–24 increased from 2007 to 2017, while homicide rates increased from 2014 to 2017.
- For persons aged 10–14, suicide rates increased from 2007 to 2017, while homicide rates declined.
- Suicide and homicide death rates for persons aged 15–19 have increased recently during 2000–2017, from 2007 to 2017 for suicide and from 2014 to 2017 for homicide.
- Suicide death rates for persons aged 20–24 increased from 2000 to 2017, and homicide rates increased from 2014 to 2017.
- Summary
- Data sources and methods
- About the authors
- References
- Suggested citation
PDF Version (423 KB)
Sally C. Curtin, M.A., and Melonie Heron, Ph.D.
Key findings
Data from the National Vital Statistics System
- After stable trends from 2000 to 2007, suicide rates for persons aged 10–24 increased from 2007 (6.8 per 100,000 persons) to 2017 (10.6), while homicide rates declined from 2007 to 2014 and then increased through 2017.
- The suicide rate for persons aged 10–14 declined from 2000 (1.5) to 2007 (0.9), and then nearly tripled from 2007 to 2017 (2.5), while the homicide rate declined 18% from 2000 (1.1) to 2017 (0.9).
- For persons aged 15–19 and 20–24, suicide and homicide death rates both increased more recently during the 2000–2017 period, with the increase in suicide rates beginning earlier than for homicide rates.
- For the total age group 10–24 and for persons aged 15–19 and 20–24, suicide rates surpassed homicide rates during the latter part of the
2000–2017 period.
Deaths due to suicide and homicide, often referred to collectively as violent deaths, have consistently been a major cause of premature death to persons aged 10–24 in the United States (1–3). In 2017, suicide was the second leading cause of death for persons aged 10–14, 15–19, and 20–24, and homicide ranked third for persons aged 15–19 and 20–24 and fifth for persons aged 10–14 (4). This report presents trends for 2000–2017 in suicide and homicide death rates for all persons aged 10–24 and for age groups 10–14, 15–19, and 20–24.
Keywords: death certificates, underlying cause of death, National Vital Statistics System
After a stable period from 2000 to 2007, suicide rates for persons aged 10–24 increased from 2007 to 2017, while homicide rates increased from 2014 to 2017.
- The suicide rate among persons aged 10–24 was stable from 2000 to 2007, and then increased 56% between 2007 (6.8 per 100,000) and 2017 (10.6) (Figure 1). The pace of increase for suicide was greater from 2013 to 2017 (7% annually, on average) than from 2007 to 2013 (3% annually).
- After a stable period from 2000 to 2007, the homicide rate among persons aged 10–24 declined 23% from 2007 (9.0) to 2014 (6.7), and then increased 18% through 2017 (7.9).
- In 2000, the homicide rate for persons aged 10–24 (8.7) was higher than the suicide rate (7.2) and remained higher through 2009. From 2011 to 2017, the suicide rate was higher than the homicide rate (10.6 and 7.9, respectively, in 2017).
Figure 1. Suicide and homicide death rates among persons aged
10–24: United States, 2000–2017
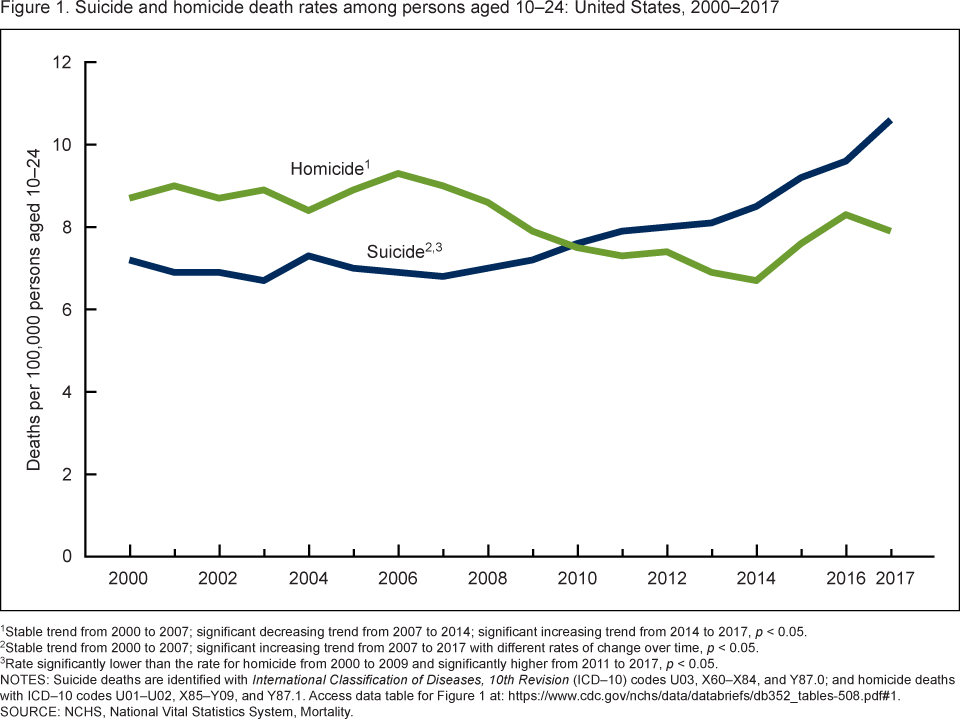
1Stable trend from 2000 to 2007; significant decreasing trend from 2007 to 2014; significant increasing trend from 2014 to 2017, p < 0.05.
2Stable trend from 2000 to 2007; significant increasing trend from 2007 to 2017 with different rates of change over time,
p < 0.05.
3Rate significantly lower than the rate for homicide from 2000 to 2009 and significantly higher from 2011 to 2017, p < 0.05.
NOTES: Suicide deaths are identified with International Classification of Diseases, 10th Revision (ICD–10) codes U03,
X60–X84, and Y87.0; and homicide deaths with ICD–10 codes U01–U02, X85–Y09, and Y87.1.
Access data table for Figure 1.
SOURCE: NCHS, National Vital Statistics System, Mortality.
For persons aged 10–14, suicide rates increased from 2007 to 2017, while homicide rates declined.
- The suicide rate for persons aged 10–14 declined from 2000 (1.5) to 2007 (0.9), and then nearly tripled from 2007 to 2017 (2.5) (Figure 2).
- Homicide rates for persons aged 10–14 declined 18% from 2000 (1.1) to 2017 (0.9).
- The suicide rate for persons aged 10–14 was higher than the homicide rate from 2000 to 2005, not significantly different from 2006 to 2008, and higher again from 2009 to 2017. By 2017, the suicide rate was more than twice the homicide rate (2.5 compared with 0.9).
Figure 2. Suicide and homicide death rates among children and adolescents aged 10–14: United States, 2000–2017
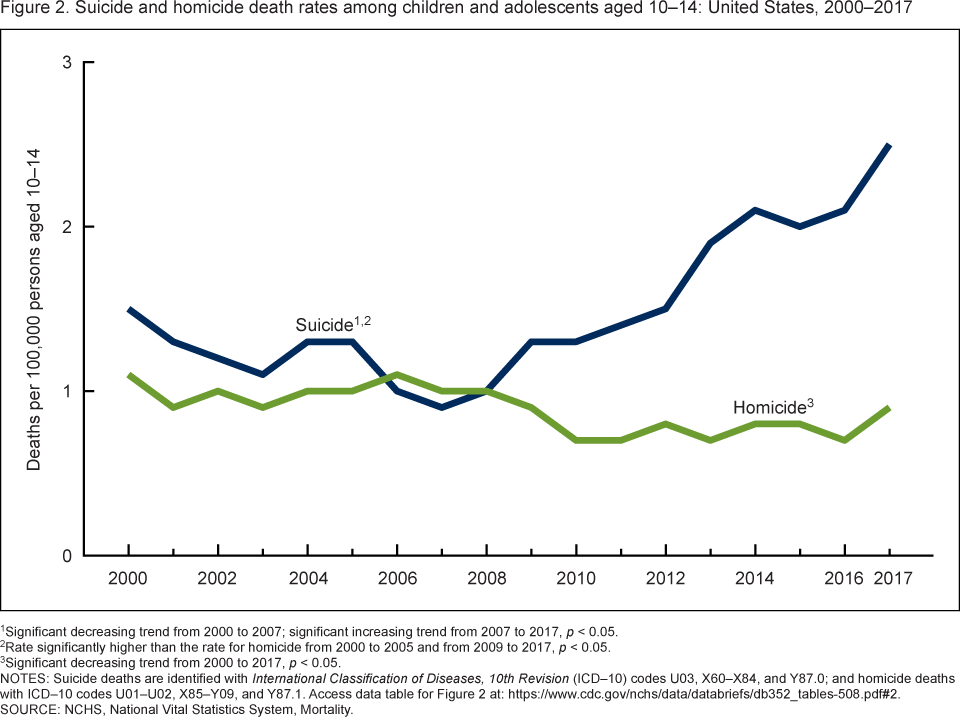
1Significant decreasing trend from 2000 to 2007; significant increasing trend from 2007 to 2017, p < 0.05.
2Rate significantly higher than the rate for homicide from 2000 to 2005 and from 2009 to 2017, p < 0.05.
3Significant decreasing trend from 2000 to 2017, p < 0.05.
NOTES: Suicide deaths are identified with International Classification of Diseases, 10th Revision (ICD–10) codes U03,
X60–X84, and Y87.0; and homicide deaths with ICD–10 codes U01–U02, X85–Y09, and Y87.1.
Access data table for Figure 2.
SOURCE: NCHS, National Vital Statistics System, Mortality.
Suicide and homicide death rates for persons aged 15–19 have increased recently during 2000–2017, from 2007 to 2017 for suicide and from 2014 to 2017 for homicide.
- The suicide rate for persons aged 15–19 was stable from 2000 to 2007, and then increased 76% from 2007 (6.7) to 2017 (11.8) (Figure 3). The pace of increase was greater from 2014 to 2017 (10% annually, on average) than from 2007 to 2014 (3% annually).
- Homicide rates for persons aged 15–19 increased from 2000 to 2007, declined from 2007 to 2014, and then increased 30% from 2014 (6.7) to 2017 (8.7).
- In 2000, the homicide rate for persons aged 15–19 (9.5) was higher than the suicide rate (8.0) and remained higher through 2010. From 2011 to 2017, the suicide rate was higher than the homicide rate (11.8 and 8.7, respectively, in 2017).
Figure 3. Suicide and homicide death rates among adolescents aged 15–19: United States, 2000–2017
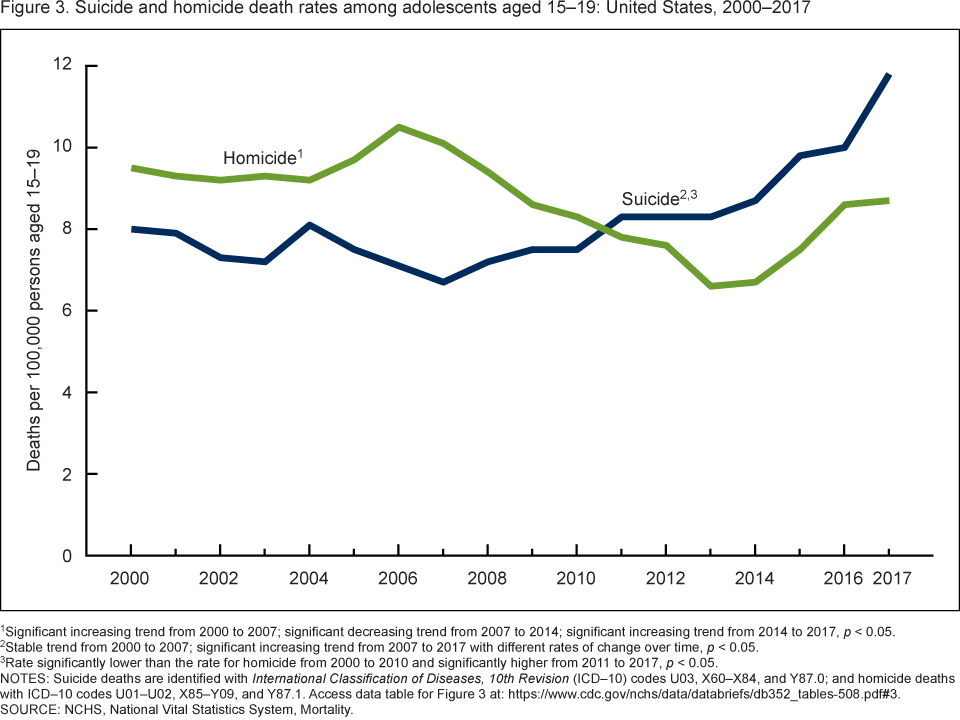
1Significant increasing trend from 2000 to 2007; significant decreasing trend from 2007 to 2014; significant increasing trend from 2014 to 2017, p < 0.05.
2Stable trend from 2000 to 2007; significant increasing trend from 2007 to 2017 with different rates of change over time,
p < 0.05.
3Rate significantly lower than the rate for homicide from 2000 to 2010 and significantly higher from 2011 to 2017, p < 0.05.
NOTES: Suicide deaths are identified with International Classification of Diseases, 10th Revision (ICD–10) codes U03,
X60–X84, and Y87.0; and homicide deaths with ICD–10 codes U01–U02, X85–Y09, and Y87.1.
Access data table for Figure 3.
SOURCE: NCHS, National Vital Statistics System, Mortality.
Suicide death rates for persons aged 20–24 increased from 2000 to 2017, and homicide rates increased from 2014 to 2017.
- The suicide rate increased 36% from 2000 (12.5) to 2017 (17.0), with a greater pace of increase from 2013 to 2017 (6% annually, on average) than from 2000 to 2013 (1% annually) (Figure 4).
- The homicide rate declined 24% from 2000 (16.0) to 2014 (12.1), and then increased 15% through 2017 (13.9).
- In 2000, the homicide rate for persons aged 20–24 (16.0) was 28% higher than the suicide rate (12.5); the rates converged in 2010, were essentially the same from 2010 to 2012, and then the suicide rate was higher than the homicide rate from 2013 to 2017 (17.0 and 13.9, respectively, in 2017).
Figure 4. Suicide and homicide death rates among young adults aged 20–24: United States, 2000–2017
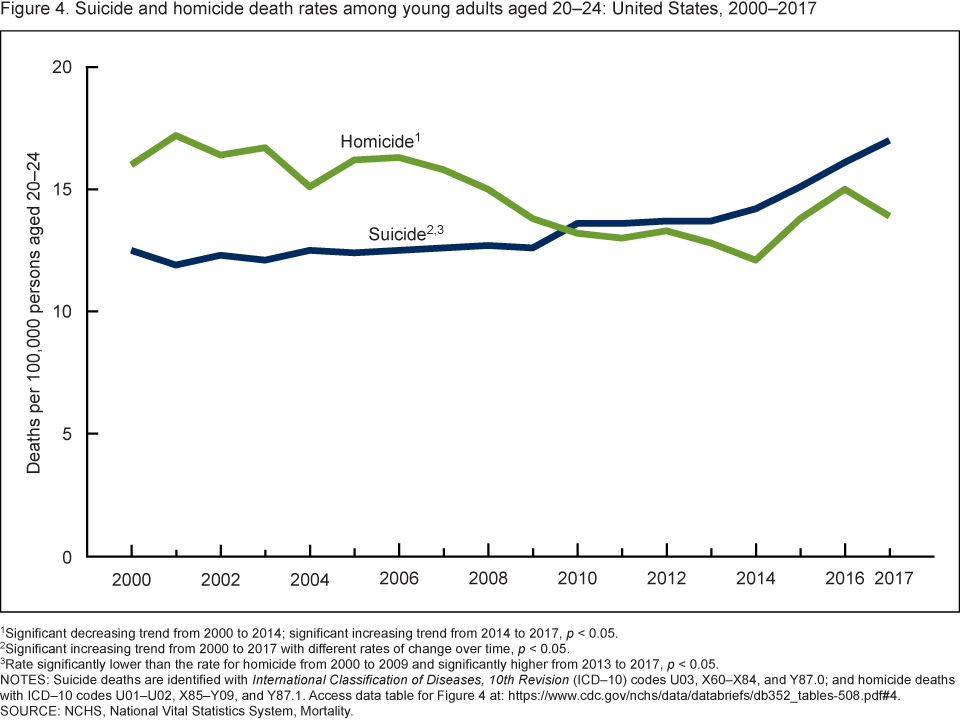
1Significant decreasing trend from 2000 to 2014; significant increasing trend from 2014 to 2017, p < 0.05.
2Significant increasing trend from 2000 to 2017 with different rates of change over time, p < 0.05.
3Rate significantly lower than the rate for homicide from 2000 to 2009 and significantly higher from 2013 to 2017, p < 0.05.
NOTES: Suicide deaths are identified with International Classification of Diseases, 10th Revision (ICD–10) codes U03,
X60–X84, and Y87.0; and homicide deaths with ICD–10 codes U01–U02, X85–Y09, and Y87.1.
Access data table for Figure 4.
SOURCE: NCHS, National Vital Statistics System, Mortality.
Summary
In 2017, suicide and homicide were the second and third leading causes of death for persons aged 15–19 and 20–24 and ranked second and fifth among persons aged 10–14 (4). After a stable period from 2000 to 2007, suicide and homicide death rates for persons aged 10–24 increased recently during the time period, since 2007 for suicide, and since 2014 for homicide. For persons aged 10–14, suicide rates began increasing in 2010, whereas the homicide rate declined during the 2000–2017 period. In contrast, recent increases were observed for both suicide and homicide death rates among persons aged 15–19 and 20–24, with the increases for suicide rates beginning earlier than for homicide rates. In addition, for persons aged 15–19 and 20–24, suicide rates surpassed homicide rates during the latter part of the period.
Data sources and methods
Mortality and population data are from the National Center for Health Statistics’ 2000–2017 multiple cause-of-death mortality files (5). These data are compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. Population data for 2000 and 2010 are April 1 bridged-race census counts, for 2001–2009 they are July 1 intercensal estimates, and for 2011–2017 they are July 1 postcensal estimates based on the 2010 census. Deaths to persons aged 10–24 that were assigned an International Classification of Diseases, 10th Revision underlying cause-of-death code for homicide (U01–U02, X85–Y09, and Y87.1) and suicide (U03, X60–X84, and Y87.0) (6) were selected. Numbers of deaths for suicide and homicide for the age groups 10–14, 15–19, and 20–24 are shown in corresponding data tables for each figure.
Figures 1–4 were evaluated using the Joinpoint Regression Program (7). The Joinpoint software was used to fit weighted least-squares regression models to the estimated proportions on the logarithmic scale. The default settings allowed for as few as three observed time points in the beginning, ending, and middle line segments, including the joinpoints. Using these settings, a maximum of two joinpoints were searched for using the grid search algorithm and permutation test and an overall alpha level of 0.05.
Pairwise comparisons between suicide and homicide rates were tested using the z test statistic at the 0.05 level of significance.
About the authors
Sally C. Curtin and Melonie Heron are with the National Center for Health Statistics, Division of Vital Statistics.
References
- Johnston BD, Ebel BE. Child injury control: Trends, themes, and controversies. Acad Pediatr 13(6):499–507. 2013.
- David-Ferdon C, Simon TR. Preventing youth violence: Opportunities for action. National Center for Injury Prevention and Control. 2014.
- Sumner SA, Mercy JA, Dahlberg LL, Hillis SD, Klevens J, Houry D. Violence in the United States: Status, challenges, and opportunities. JAMA 314(5):478–88. 2015.
- Heron M. Deaths: Leading causes for 2017. National Vital Statistics Reports; vol 68 no 6. Hyattsville, MD: National Center for Health Statistics. 2019.
- National Center for Health Statistics. CDC WONDER. Underlying cause of death, 1999–2017. 2018.
- World Health Organization. International statistical classification of diseases and related health problems, 10th revision (ICD–10). 2008 ed. Geneva, Switzerland. 2009.
- National Cancer Institute. Joinpoint Regression Program (Version 4.4.0.0) [computer software]. 2017.
Suggested citation
Curtin SC, Heron M. Death rates due to suicide and homicide among persons aged 10–24: United States, 2000–2017. NCHS Data Brief, no 352. Hyattsville, MD: National Center for Health Statistics. 2019.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Jennifer H. Madans, Ph.D., Acting Director
Amy M. Branum, Ph.D., Acting Associate Director for Science
Division of Vital Statistics
Steven Schwartz, Ph.D., Director
Hanyu Ni, Ph.D., M.P.H., Associate Director for Science