Prevalence and Management of Pain, by Race and Dementia Among Nursing Home Residents: United States, 2004
- Key findings
- Does pain vary by race? Does pain vary by a diagnosis of dementia?
- Did residents with pain receive appropriate pain management?
- Among residents with pain, does appropriate pain management vary by race or diagnosis of dementia?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 30, March 2010
PDF Version (997 KB)
by Manisha Sengupta, Ph.D.; Anita Bercovitz, M.P.H., Ph.D.; and Lauren D. Harris-Kojetin, Ph.D.
Key findings
Data from the National Nursing Home Survey, 2004
- About one-quarter of all nursing home residents reported or showed signs of pain.
- Nonwhite residents and residents with dementia were less likely to report or show signs of pain compared with white residents and residents without dementia.
- Nonwhite residents with dementia were least likely, and white residents without dementia were most likely to report or show signs of pain.
- Forty-four percent of nursing home residents with pain received neither standing orders for pain medication nor special services for pain management (i.e., appropriate pain management).
- Among residents with dementia and pain, nonwhite residents were more likely than white residents to lack appropriate pain management.
Pain is common among nursing home residents, and effective pain management has an impact on improving quality of life (1,2). Previous research has shown race differences in pain reporting and management in various settings, with racial and ethnic minority groups less likely than white residents to report pain and receive adequate treatment (3–9). Other studies have documented cognitive impairment as a barrier in the detection and self-report of pain, with the underreporting likely resulting in undertreatment (10–15). However, the relationships among race, dementia, and pain reporting and management remain understudied. This report explores the combined impact of race and a diagnosis of dementia on reporting or showing signs of pain and pain management among nursing home residents.
Keywords: Appropriate pain management, pain underreporting, special pain management services, National Nursing Home Survey
Does pain vary by race? Does pain vary by a diagnosis of dementia?
Overall among nursing home residents, 23% reported or showed signs of pain in the 7 days prior to the interview.
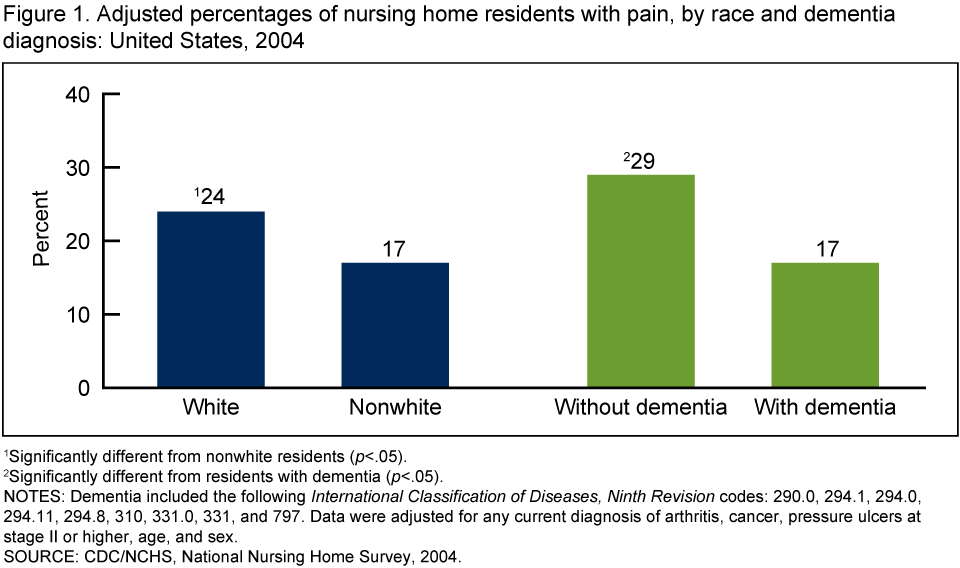
Nonwhite residents were less likely to report or show signs of pain than white residents. Nursing home residents with dementia were also less likely to report or show signs of pain compared with residents who did not have dementia.
Among all residents, 17% of nonwhite residents compared with 24% of white residents reported or showed signs of pain.
Seventeen percent of those with dementia reported or showed signs of pain in the 7 days prior to the interview compared with 29% of those without dementia (Figure 1).
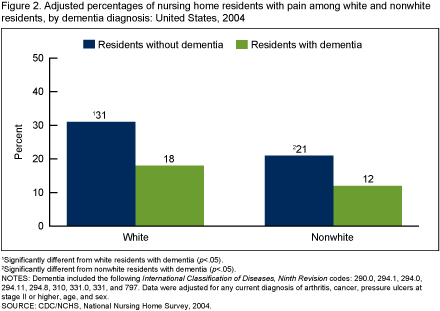
A similar association between dementia status and reporting of pain existed among both white and nonwhite residents, with a significantly greater proportion of residents without dementia reporting or showing signs of pain compared with residents with dementia. Nonwhite residents with dementia (12%) were least likely to report or show signs of pain, and white residents without dementia (31%) were most likely to report or show signs of pain (Figure 2).
Did residents with pain receive appropriate pain management?
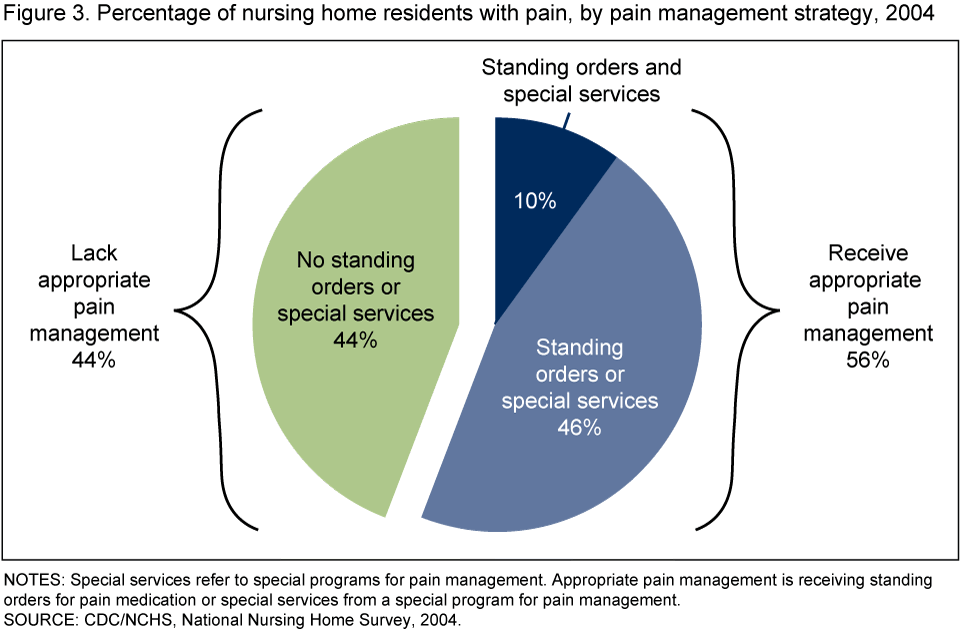
Although the use of medications for pain management may vary by age, sex, and clinical condition, appropriate care for pain is either standing orders for pain medication or receipt of services from a special program for pain management, particularly among nursing home residents with moderate to severe pain (16). Figure 3 gives the overall distribution of pain management strategies used for nursing home residents with pain, without adjusting for age, sex, or clinical diagnosis. Among nursing home residents with pain, 44% neither had standing orders nor received special services for pain management, 46% either had standing orders or received special services, and another 10% had both standing orders and received special services for pain management (Figure 3).
Among residents with pain, does appropriate pain management vary by race or diagnosis of dementia?
There were no statistically significant differences in lack of appropriate pain management by dementia diagnosis (44% of those with dementia and 45% of those without dementia) or race (45% of white residents and 48% of nonwhite residents) (not shown).
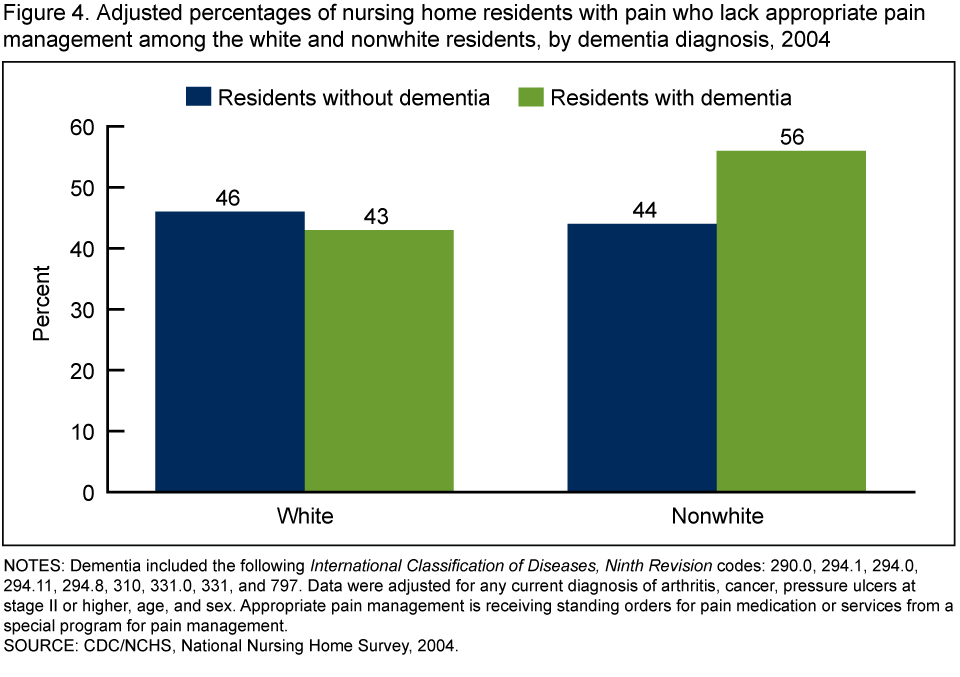
If one considers race and dementia diagnosis simultaneously, a similar percentage of white residents with or without dementia and nonwhite residents without dementia lacked appropriate pain management (43%, 46%, and 44%, respectively) (Figure 4).However, lack of appropriate pain management differed between nonwhite residents with dementia and white residents with dementia; 56% of nonwhite residents with dementia lacked appropriate pain management compared with 43% of white residents with dementia (p<.05).
Summary
About one-quarter of nursing home residents reported or showed signs of pain. Prevalence of pain among residents varied by race and dementia diagnosis. Consistent with previous research, these nationally representative results suggest that nonwhite residents were less likely to report or show signs of pain than white residents, and residents with dementia were less likely to report or show signs of pain than residents without dementia. As a group, white residents without dementia appear at one end of the spectrum with the highest likelihood of reporting or showing signs of pain. At the other end of the spectrum are nonwhite residents with dementia, who are least likely to report or show signs of pain.
Over 40% of all nursing home residents with pain received neither standing orders for pain medication nor special services for pain management. Among residents with dementia and pain, there were differences in appropriate pain management between nonwhite and white residents, with nonwhite residents being more likely than white residents to lack appropriate pain management. Because questions about pain management were asked only if a resident reported or showed signs of pain, residents whose pain was controlled were not included in this analysis. Therefore, residents without reported or noted pain because it was controlled, may have received pain management, and the estimates of receipt of pain management approaches presented in this report may be underestimated. In light of national goals to reduce racial disparities in health care quality, these findings contribute to the literature by exploring the complex associations among race, dementia, and pain management.
Definitions
Dementia: Nursing home providers were asked if the sampled resident had any diagnosis of dementia that included the following International Classification of Diseases, Ninth Revision codes: 290.0, 294.1, 294.0, 294.11, 294.8, 310, 331.0, 331, and 797, in any of 16 current diagnoses.
Pain: Nursing home providers were asked if the sampled resident had reported or showed any signs of pain in the past 7 days prior to the interview. The question read, “Since admission/In the past 7 days, that is, since {PAST 7 DAYS}, has sampled person/resident {SP} reported or shown evidence of pain? Please include grimacing or other non-verbal signs that suggest pain.” Throughout this report, “reported or showed signs of pain” and “with pain” are used interchangeably.
PRN: A medication ordered by a medical practitioner to be administered on an “as needed” basis. Only nursing home residents who reported or showed signs of pain were asked if they received PRN pain medication.
Standing order: A protocol of medication administration allowing a registered nurse to administer medication without a prior prescription. Only nursing home residents who reported or showed signs of pain were asked if they received standing orders for pain medication.
Special services for pain management: Nursing home providers were asked if the sampled resident was currently receiving services from a special program for pain management. Responses were categorized to indicate whether the resident was using special services, the resident was not using special services, or the nursing home did not have any specialty programs for pain management.
Data source and methods
The data used for this analysis come from the resident module of the 2004 National Nursing Home Survey (NNHS). NNHS is a periodic nationally representative cross-sectional survey of nursing homes in the United States. The survey provides a plethora of information on nursing home characteristics, the services they provide, the staffs they employ, and the residents they serve.
The 2004 survey used a stratified, multistage probability sample from a frame of nursing homes based on strata defined by bed size and metropolitan statistical area status. The first stage involved the selection of facilities followed by the selection of residents in the second stage. Using systematic sampling with probability proportional to bed size, 1,545 nursing homes were sampled. In the second stage, residents were randomly selected from a list provided at the time of the interview of residents as of midnight the day before the survey. A selection of up to 12 residents per facility resulted in a total sample of 14,017 current residents. The survey was administered using a computer-assisted personal interview (CAPI) system. Data for the survey were obtained through personal interviews with facility administrators and designated staff who used administrative records to answer questions about the facilities, staff, services and programs, and medical records to answer questions about the residents.
Although residents with characteristics associated with pain may well vary across nursing homes, estimates of pain reporting and appropriate pain management by race and dementia status in Figures 1, 2, and 4 were adjusted for age, sex, and a set of conditions that are associated with pain. The adjusted percentages reported in Figures 1, 2, and 4 are the predicted marginal probabilities estimated for the average person in a given dementia status and racial group after adjusting for all other variables noted in the figure. Adjusted and unadjusted results were similar. The marginal probabilities, their associated contrasts, and tests for statistical significance were estimated using general estimating equations to construct logistic regression models in SAS-callable SUDAAN. Figure 3 shows the overall distribution of pain management strategies used for nursing home residents in pain, irrespective of age, sex, or clinical diagnosis, and therefore does not control for these factors. Severity of pain, duration of pain, and the resident’s ability to ask for medication are not addressed in this report, and may affect the observed relationships among race, dementia, and pain reporting and management.
The analysis of differences in pain management strategies (standing order, special services) was limited to nursing home residents who reported or showed signs of pain. A resulting caveat is that there may be some underestimation of residents receiving standing orders or using services from special pain management programs, if these residents did not report or show any residual pain after receiving appropriate pain management.
About the authors
Manisha Sengupta, Anita Bercovitz, and Lauren D. Harris-Kojetin are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health Care Statistics, Long-Term Care Statistics Branch.
References
- Ferrell BA, Ferrell BR, Rivera L. Pain in cognitively impaired nursing home patients. J Pain Symptom Manage; 10(8):591-8. 1995.
- Katz N. The impact of pain management on quality of life. J Pain Symptom Manage; 24(1):S38-S47. 2002.
- Council of Ethical and Judicial Affairs. Black-White disparities in health care. JAMA; 263:2344-6. 1990.
- Green CR, Anderson KO, Baker TA, Campbell LC, et al. The Unequal Burden of Pain: Confronting Racial and Ethnic Disparities in Pain. Pain Med; 4(3):277-94. 2003.
- Green CR, Baker TA, Sato Y, Washington TL, Smith, EM. Race and chronic pain: A comparative study of young black and white Americans. J Pain; 4(4):176-83. 2003.
- Bonham VL. Race, Ethnicity, and Pain Treatment: Striving to Understand the Causes and Solutions to the Disparities in Pain Treatment. J Law Med Ethics; 29:52-68. 2001.
- Cleeland CS, Gonin R, Baez L, Loehrer P, Oandya KJ. Pain and treatment of pain in minority patients with cancer. The Eastern Cooperative Oncology Group Minority Outpatient Pain Study. Ann Intern Med; 127(9):813-8. 1997.
- Johnson-Umezulike JM. A comparison of pain perception of elderly African Americans and Caucasians. Nursingconnections; 12:5-12. 1999.
- Bernabei R, Gambassu G, Lapane K, landi F, et al. Management of Pain in Elderly Patients With Cancer. JAMA; 279(23):1877-82. 1998.
- Horgas AL, Elliott AF. Pain assessment and management in persons with dementia. Nurs Clin North Am; 39:593-606. 2004.
- Reynolds KS, Hanson LC, DeVellis RF, Henderson M, Steinhauser KE. Disparities in pain management between cognitively intact and cognitively impaired nursing home residents. J Pain Symptom Manage; 35(4):388-96. 2008.
- Martin R, Williams J, Hadjistavropoulos T, Hadjistavropoulos HD, MacLean M. A qualitative investigation of seniors’ and caregivers’ views on pain assessment and management. Can J Nurs Res; 37(2):142-64. 2005.
- Fisher SE, Burgio LD, Thorn BE, Hardin JM. Obtaining self-report data from cognitively impaired elders: methodological issues and clinical implications for nursing home pain assessment. Gerontologist; 46:81-8. 2006.
- Stolee P, Hillier LM, Esbaugh J, Bol N, McKellar L, Gauthier N. Instruments for the assessment of pain in older persons with cognitive impairment. J Am Geriatr Soc 53(2):319-26. 2005.
- Horgas AL, Tsai PF. Analgesic drug prescription and use in cognitively impaired nursing home residents. Nurs Res; 47(4):235-42. 1998.
- Agency for Healthcare Research and Quality (AHRQ). 2007 National Healthcare Quality Report. Rockville, MD: U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, AHRQ Pub No. 08-0040. 2008.
Suggested citation
Sengupta M, Bercovitz A, Harris-Kojetin LD. Prevalence and management of pain, by race and dementia among nursing home residents: United States, 2004. NCHS data brief, no 30. Hyattsville, MD: National Center for Health Statistics. 2010.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Jane E. Sisk, Ph.D., Director