Trends in Emergency Department Visits for Ischemic Stroke and Transient Ischemic Attack: United States, 2001–2011
- Key findings
- The total age-adjusted rate of emergency department visits for ischemic stroke or TIA for patients aged 18 and over decreased from 2001 through 2011, with the greatest decrease in visit rates seen in patients aged 55–74.
- From 2004 through 2011, the percentage of emergency department visits for ischemic stroke or TIA in which patients arrived by ambulance decreased 41% for patients under 75.
- The percentage of emergency department visits for ischemic stroke or TIA with a magnetic resonance imaging (MRI) or computed tomography (CT) test ordered or provided increased 39% from 2001 through 2011.
- The percentage of emergency department visits for ischemic stroke or TIA admitted or transferred to another hospital increased 10% from 2001 through 2011.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 194, March 2015
PDF Version (862 KB)
Anjali Talwalkar, M.D., M.P.H.; and Sayeedha Uddin, M.D., M.P.H.
Key findings
Data from the National Hospital Ambulatory Medical Care Survey, 2001–2011
- From 2001 through 2011, the rate of emergency department visits for ischemic stroke or transient ischemic attack (TIA) decreased 35% for patients aged 18 and over and 51% for patients aged 55–74.
- From 2004 through 2011, the percentage of emergency department visits for ischemic stroke or TIA in which the patient arrived by ambulance decreased 41% for patients under 75.
- The percentage of emergency department visits for ischemic stroke or TIA in which a magnetic resonance imaging (MRI) or computed tomography (CT) test was ordered or provided increased 39% from 2001 through 2011.
- The percentage of emergency department visits for ischemic stroke or TIA that resulted in admission or transfer to a hospital increased 10% from 2001 through 2011.
Stroke is the fifth leading cause of death in the United States (1). About 87% of all strokes are ischemic strokes (2). Transient ischemic attacks (TIAs) cause similar symptoms, but the blockage of blood flow to the brain is temporary. However, about one-third of people who have a TIA will have a stroke within 1 year (3). Emergency departments play a critical role in the diagnosis and management of ischemic stroke and TIA. The evaluation of these conditions in the emergency department is similar, so they are combined for this analysis. This report presents recent trends in visits to emergency departments for ischemic stroke or TIA.
Keywords: cerebrovascular disease, health care utilization, National Hospital Ambulatory Medical Care Survey (NHAMCS)
The total age-adjusted rate of emergency department visits for ischemic stroke or TIA for patients aged 18 and over decreased from 2001 through 2011, with the greatest decrease in visit rates seen in patients aged 55–74.
Figure 1. Age-adjusted and age-specific emergency department visit rates for ischemic stroke or transient ischemic attack among patients aged 18 and over: United States, 2001–2011
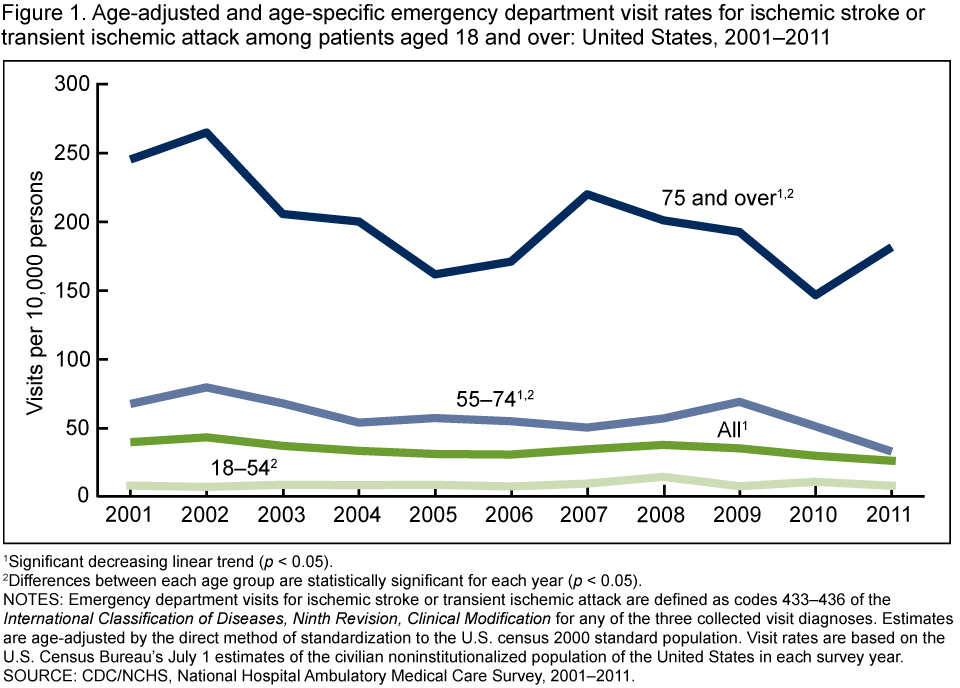
1Significant decreasing linear trend (p < 0.05).
2Differences between each age group are statistically significant for each year (p < 0.05).
NOTES: Emergency department visits for ischemic stroke or transient ischemic attack are defined as codes 433–436 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the three collected visit diagnoses. Estimates are age-adjusted by the direct method of standardization to the U.S. census 2000 standard population. Visit rates are based on the U.S. Census Bureau’s July 1 estimates of the civilian noninstitutionalized population of the United States in each survey year.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2001–2011.
Among patients aged 18 and over, the rate of emergency department visits for ischemic stroke or TIA decreased 35% from 40 per 10,000 persons in 2001 to 26 per 10,000 persons in 2011 (Figure 1). The emergency department visit rate for ischemic stroke or TIA for patients aged 55–74 decreased 51% from 68 visits per 10,000 persons in 2001 to 33 visits per 10,000 persons in 2011. The emergency department visit rate for ischemic stroke or TIA for patients aged 75 and over decreased 26% from 245 visits per 10,000 persons in 2001 to 182 visits per 10,000 persons in 2011. However, no change in visit rate for this age group was observed from 2006 through 2011. The emergency department visit rate for ischemic stroke or TIA for patients aged 18–54 did not change. Patients aged 75 and over had the highest rate of emergency department visits for ischemic stroke or TIA throughout the period. Patients aged 18–54 had the lowest rate of emergency department visits for ischemic stroke or TIA.
From 2004 through 2011, the percentage of emergency department visits for ischemic stroke or TIA in which patients arrived by ambulance decreased 41% for patients under 75.
For patients under 75, the percentage of emergency department visits for ischemic stroke or TIA in which they arrived by ambulance decreased from 41% in 2004–2005 to 24% in 2010–2011 (Figure 2). For patients aged 75 and over, the percentage of visits for ischemic stroke or TIA in which they arrived by ambulance did not significantly change from 2004 through 2011. Throughout the period, the percentage arriving by ambulance was higher for older patients than for those under 75.
Figure 2. Emergency department visits for ischemic stroke or transient ischemic attack with ambulance arrival, by age: United States, 2004–2011
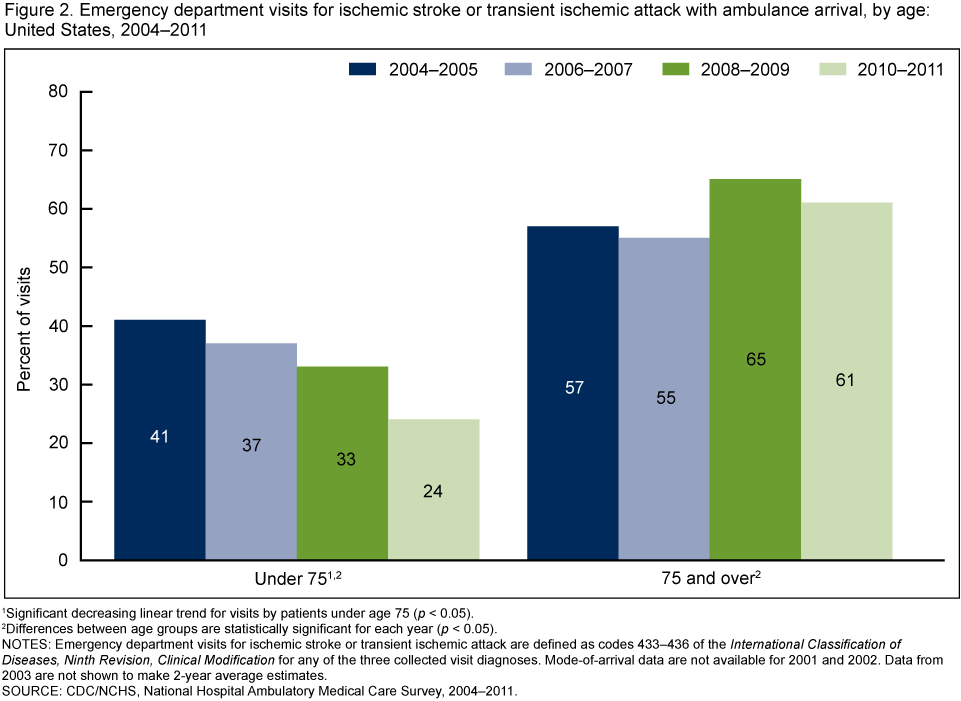
1Significant decreasing linear trend for visits by patients under age 75 (p < 0.05).
2Differences between age groups are statistically significant for each year (p < 0.05).
NOTES: Emergency department visits for ischemic stroke or transient ischemic attack are defined as codes 433–436 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the three collected visit diagnoses. Mode-of-arrival data are not available for 2001 and 2002. Data from 2003 are not shown to make 2-year average estimates.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2004–2011.
The percentage of emergency department visits for ischemic stroke or TIA with a magnetic resonance imaging (MRI) or computed tomography (CT) test ordered or provided increased 39% from 2001 through 2011.
The percentage of visits for ischemic stroke or TIA with an MRI or CT test increased from 66% in 2001 to 92% in 2011 (Figure 3). The percentage of visits for other diagnoses with an MRI or CT test also increased, but the rate of increase for MRI or CT testing was higher for ischemic stroke or TIA visits compared with other visits.
Figure 3. Emergency department visits with magnetic resonance imaging or computed tomography test ordered or provided, by visit diagnosis: United States, 2001–2011
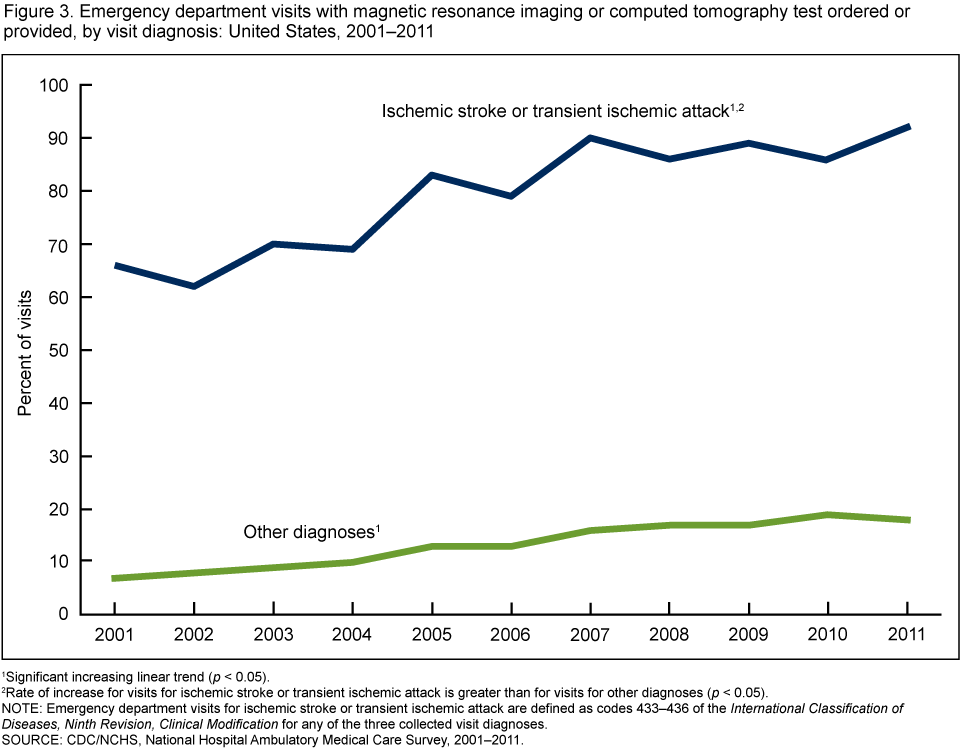
1Significant increasing linear trend (p < 0.05).
2Rate of increase for visits for ischemic stroke or transient ischemic attack is greater than for visits for other diagnoses (p < 0.05).
NOTE: Emergency department visits for ischemic stroke or transient ischemic attack are defined as codes 433–436 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the three collected visit diagnoses.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2001–2011.
The percentage of emergency department visits for ischemic stroke or TIA admitted or transferred to another hospital increased 10% from 2001 through 2011.
The percentage of emergency department visits for ischemic stroke or TIA that resulted in admission or transfer to another hospital increased from 71% in 2001 to 78% in 2011 (Figure 4). The percentage of visits for other diagnoses that were admitted or transferred did not change.
Figure 4. Emergency department visits admitted or transferred to another hospital, by visit diagnosis: United States, 2001–2011
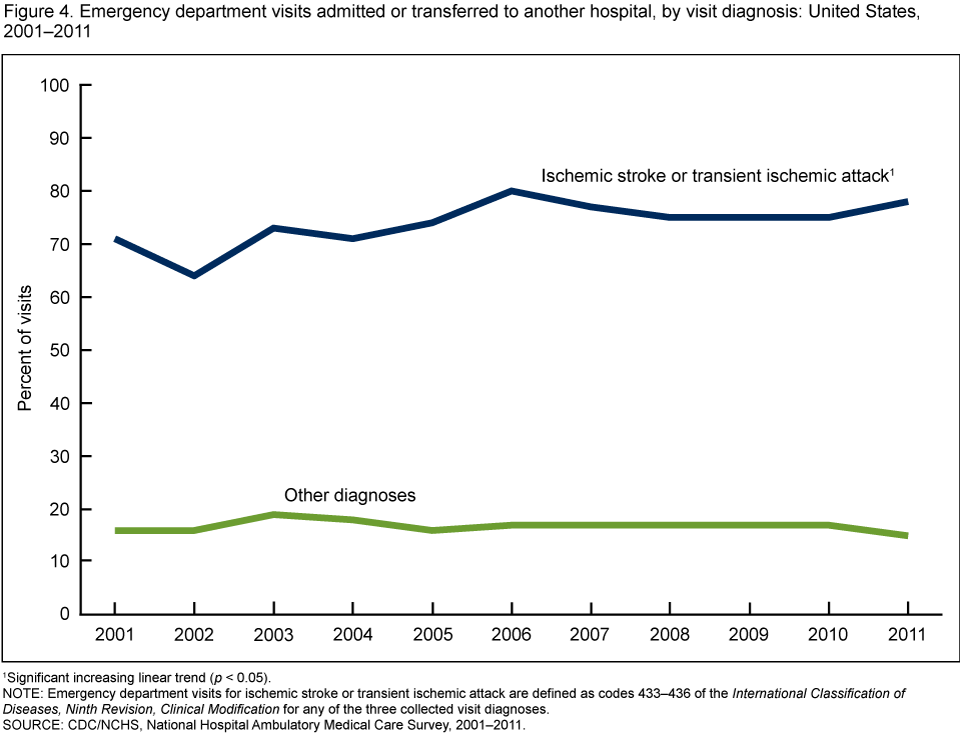
1Significant increasing linear trend (p < 0.05).
NOTE: Emergency department visits for ischemic stroke or transient ischemic attack are defined as codes 433–436 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the three collected visit diagnoses.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2001–2011.
Summary
While stroke remains a leading cause of death and disability in the United States, mortality from stroke has been declining. This report demonstrates that the age-adjusted emergency department visit rate for stroke or TIA has also been declining. Among specific age groups, visit rates for ischemic stroke or TIA decreased for patients aged 55 and over, with the largest decline seen for patients aged 55–74. While visit rates also declined for patients aged 75 and over from 2001 through 2011, no significant decline was seen after 2006. Rates for patients aged 75 and over also remained the highest. No change in visit rates for patients aged 18–54 was seen.
Changes in the resources used in the acute management of ischemic stroke and TIA have also occurred. Advanced imaging and admission or transfer to a hospital both increased at emergency department visits for ischemic stroke or TIA from 2001 through 2011. However, from 2004 through 2011, a decline in the percentage of visits in which patients under 75 arrived by ambulance was observed. Monitoring visits to emergency departments will continue to be important to assess the impact of public health campaigns to promote rapid emergency care of stroke and TIA and to describe the burden of these conditions on the U.S. health care system.
Definitions
Ischemic stroke: Occurs when a blood vessel that carries oxygen and nutrients to the brain is blocked by an obstruction such as a blood clot. When that happens, part of the brain cannot get the oxygen it needs, so the brain cells die (3).
Transient ischemic attack: Similar to an ischemic stroke, but the blockage of blood flow to the brain is temporary. There is usually no permanent injury to the brain cells (3).
Emergency department visit for ischemic stroke or transient ischemic attack: A visit to a hospital emergency department with ischemic stroke or transient ischemic attack documented as any one of three diagnoses collected for that visit.
Data source and methods
Data from the 2001–2011 National Hospital Ambulatory Medical Care Survey (NHAMCS) were analyzed. NHAMCS is an annual nationally representative survey of visits to nonfederal hospital-based outpatient departments, emergency departments, and ambulatory surgery centers. The survey uses a multistage probability sample design. A sample weight that takes all stages of design into account is computed for each sample visit. The survey data are weighted to produce unbiased national annual estimates of hospital-based ambulatory visits (4).
Analyses included visits from the emergency department component of NHAMCS by patients aged 18 and over. Up to three visit diagnoses are collected for each sampled visit. A visit for ischemic stroke or TIA was defined as a visit with any listed diagnosis codes 433–436 based on the International Classification of Diseases, Ninth Revision, Clinical Modification.
Data analyses were performed using the statistical packages SAS version 9.3 (SAS Institute, Cary, N.C.), SUDAAN version 10.0 (RTI International, Research Triangle Park, N.C.), and Stata version 12.0 (StataCorp, College Station, T.X.). Age-adjusted rates were calculated using the direct method and the 2000 U.S. census projected population for age groups 18–39, 40–59, 60–79, and 80 and over (5). A weighted least-squares regression analysis was used to determine the significance of trends at the 0.05 level. Differences between rates of change for trends and between subgroups were evaluated with two-tailed t tests and a significance level of 0.05.
About the authors
Anjali Talwalkar and Sayeedha Uddin are with CDC’s National Center for Health Statistics, Division of Health Care Statistics.
References
- Kochanek KD, Murphy SL, Xu JQ, Arias E. Mortality in the United States, 2013. NCHS data brief, no 178. Hyattsville, MD: National Center for Health Statistics. 2014.
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 129(3):e28–e292. 2014.
- American Heart Association/American Stroke Association. Types of stroke.
- NCHS. Public use data file documentation 2001–2011 National Hospital Ambulatory Medical Care Survey. Hyattsville, MD: National Center for Health Statistics.
- Klein RJ, Schoenborn CA. Age adjustment using the 2000 projected U.S. population. Healthy People Statistical Notes, no. 20. Hyattsville, MD: National Center for Health Statistics. 2001.
Suggested citation
Talwalkar A, Uddin S. Trends in emergency department visits for ischemic stroke and transient ischemic attack: United States, 2001–2011. NCHS data brief, no 194. Hyattsville, MD: National Center for Health Statistics. 2015.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Nathaniel Schenker, Ph.D., Deputy Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director