Role of International Medical Graduates Providing Office-based Medical Care: United States, 2005-2006
NCHS Data Brief No. 13, February 2009
PDF Version (998 KB)
by Esther Hing, M.P.H., and Susan Lin, Dr.P.H.
Key findings
- In 2005-2006, about one-quarter (24.6%) of all visits to office-based physicians were to international medical graduates. Hispanic or Latino and Asian or Pacific Islander patients made more visits to international medical graduates (24.9%) than to U.S. medical graduates (12.4%). International medical graduates also saw a higher percentage of visits made by patients expecting to use Medicaid or State Children’s Health Insurance Program (SCHIP) as their primary payment source (17.6%) compared with U.S. medical graduates (10.2%).
- In 2005-2006, international medical graduates comprised 24.5% of all office-based physicians. International medical graduates were more likely to be of Asian or Pacific Islander (31.6% compared with 4.9% of U.S. medical graduates) and Hispanic or Latino descent (6.7% compared with 1.5% of U.S. medical graduates).
- International medical graduates were more likely to practice in primary care shortage areas outside of metropolitan statistical areas (67.8%) than U.S. medical graduates (39.8%).
Over the past 30 years, the number of international medical graduates in the physician workforce has steadily increased. Many entered the United States on visas that allowed them to stay in the United States if they agreed to work in an underserved area for 3 years following residency (1-3). During the last decade, however, the number of international medical graduates on these visas declined by 47% as use of less-restrictive temporary specialized worker visas increased (4). The declining number of international medical graduates serving in underserved areas has made recruiting physicians in these areas more difficult (4). In order to examine the overall role of international medical graduates in providing office-based medical care, this Data Brief compares patient and physician characteristics for office-based international medical graduates with those of U.S. medical graduates.
Keywords: physician care, international medical graduates
Who are the patients of international medical graduates?
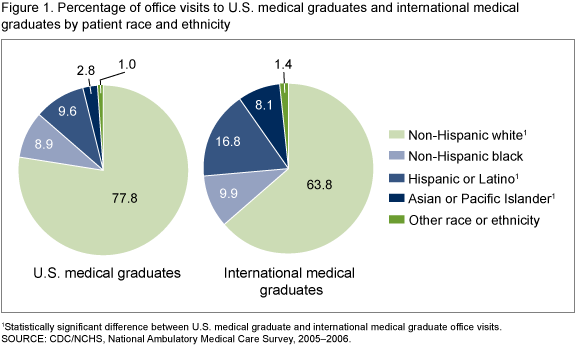
In 2005-2006, patient visits to international medical graduates comprised 24.6% of all visits to office-based physicians. Visits to international medical graduates were less likely to be made by non-Hispanic white patients (63.8% compared with 77.8% for U.S. medical graduates – Figure 1). Instead, visits to international medical graduates were more likely to be made by Hispanic or Latino patients (16.8% compared with 9.6% for U.S. medical graduates) and by patients of Asian or Pacific Islander descent (8.1% compared with 2.8% for U.S. medical graduates).
A higher percentage of visits to international medical graduates were made by patients expecting to use Medicaid (including those dually eligible for Medicare and Medicaid) or SCHIP as their primary payment source (17.6%) compared with U.S. medical graduates (10.2%) (Figure 2). A smaller percentage of visits to international medical graduates were made by patients expecting to use private insurance (46.6%) compared with U.S. medical graduates (55.2%)
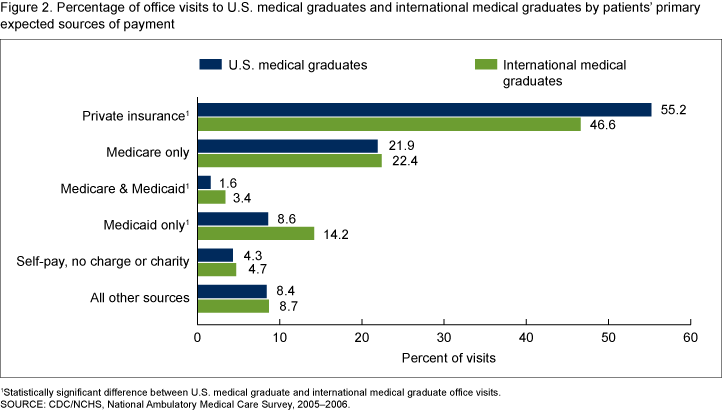
Table 1 presents U.S. Census Bureau demographic data matched to the patients’ ZIP Codes. On average, international medical graduates’ patients were more likely than U.S. medical graduates’ patients to live in neighborhoods with lower median household incomes and a higher percentage of households with incomes below the federal poverty level. International medical graduates’ patients were also more likely than U.S. medical graduates’ patients to live in neighborhoods with higher percentages of individuals who speak little or no English and of foreign-born persons.
Table 1. Characteristics of patient’s neighborhoods
| Characteristic | U.S. medical graduate | International medical graduate |
|---|---|---|
| Median household income | $47,569 | $44,758 |
| Percentage with income below poverty level | 10.6 | 12.6 |
| Percentage foreign born | 9.0 | 14.5 |
| Percentage not speaking English at all or not very well | 3.0 | 5.6 |
NOTES: All differences between U.S. medical graduate and international medical graduate office visits are statistically significant. Estimates exclude cases missing information for international medical graduate status (6.2%) and neighborhood characteristic (6.8%).
SOURCES: CDC/NCHS, National Ambulatory Medical Care Survey, 2005-2006, and U.S. Census Bureau demographic data matched to the patient’s ZIP Code of residence.
Who are international medical graduates?
In 2005-2006, international medical graduates comprised 24.5% of office-based physicians. Compared with U.S. medical graduates, international medical graduates were more likely to be of were of Asian or Pacific Islander (31.6% compared with 4.9% of U.S. medical graduates) and Hispanic or Latino descent (6.7% compared with 1.5 % of U.S. medical graduates). In contrast, 70.7% of U.S. medical graduates were non-Hispanic white compared with 25.8% of international medical graduates. International medical graduates (57.0%) were more likely than U.S. medical graduates (46.2 %) to practice in primary care specialties. International medical graduates were less likely to be board certified (78.0%) in their specialty than were U.S. medical graduates (90.2%) (Table 2).
Table 2. Selected physician characteristics of U.S. medical graduates and international graduates
| Selected characteristic | U.S. medical graduate | International medical graduate |
|---|---|---|
| Percentage of total physicians | 76.5 | 24.5 |
| Percentage non-Hispanic white | 70.7 | 25.8 |
| Percentage Asian or Pacific Islander | 4.9 | 31.6 |
| Percentage Hispanic or Latino | 1.5 | 6.7 |
| Percentage in primary care specialty | 46.2 | 57.0 |
| Percentage board certified | 90.2 | 78.0 |
NOTES: All differences between U.S. medical graduate and international medical graduate characteristics are statistically significant. Estimates exclude cases missing information for international medical graduate status (6.2%).
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey, 2005-2006.
Where do international medical graduates practice?
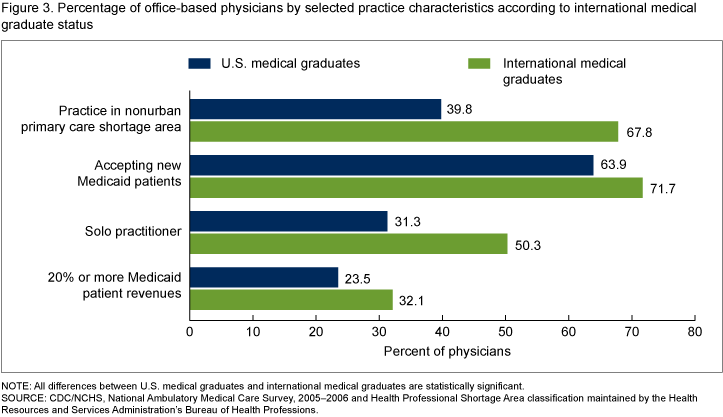
Most physicians (89.2%) practiced in urban metropolitan statistical areas (MSAs). Within MSAs, international medical graduates were just as likely as U.S. medical graduates to practice in primary care shortage areas. In 2005-2006, an estimated 5,700 international medical graduates practiced outside of MSAs; among these, a higher percentage practiced in primary care shortage areas (67.8%) than U.S. medical graduates (39.8%) ( Figure 3). A higher percentage of international medical graduates (32.1%) than U.S. medical graduates (23.5%) reported 20% or more of patient revenues from Medicaid. Consistent with deriving more revenue from Medicaid patients, international medical graduates reported accepting new Medicaid patients (71.7%) more often than U.S. medical graduates (63.9%). International medical graduates were more likely than U.S. medical graduates to be in solo practice (50.3% versus 31.3%).
Summary
This study confirmed the important contributions of office-based international medical graduates to the U.S. health care system, particularly in serving underserved populations and practicing in primary care shortage areas outside of MSAs (5-9). Compared with patient visits to U.S. medical graduates, visits to international medical graduates were more likely to be made by patients of Hispanic or Latino and Asian or Pacific Islander descent, by patients relying on Medicaid or SCHIP for payment, by patients living in poverty areas, and by patients living in areas with more immigrants. The study finding that a higher percentage of office-based international medical graduates were in primary care specialties than U.S. medical graduates is consistent with previous studies that found higher numbers of international medical graduates filling vacant residency positions in family medicine, psychiatry, and pediatrics than U.S. medical graduates (10,11). Compared with U.S. medical graduates, a greater proportion of international medical graduates practiced in nonurban primary care physician shortage areas, and derived a higher percentage of patient revenues from Medicaid.
Most previous studies on international medical graduates are based on the American Medical Association (AMA) physician or residency matching program databases, which do not include patient information. Although this report presents selected physician characteristics from the AMA and the American Osteopathic Association (AOA) masterfiles, physician characteristics presented here were updated in personal interviews with the physician, and visit characteristics were based on information found in medical records.
The study may help to inform health professional organizations and policy makers on the current characteristics of international medical graduates’ practices. The study findings suggest that the U.S. health care system continues to rely on international medical graduates to address primary care physician shortage outside of MSAs. The U.S. health care system may face challenges if the future supply and use of international medical graduates are affected by changes in visa policy and other programs affecting physician supply.
About the authors
Esther Hing is with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health Care Statistics. Susan Lin is with the Center for Family and Community Medicine at Columbia University.
Definitions
International medical graduates: Physicians working in the United States who graduated from medical schools outside of the United States.
U.S. medical graduates: Physicians working in the United States who graduated from U.S. medical schools
Data source and methods
Estimates are based on data from the 2005 and 2006 National Ambulatory Medical Care Survey or NAMCS. NAMCS is an annual nationally representative cross-sectional sample survey of visits to nonfederal office-based physicians providing patient care, as classified by the AMA or the AOA, excluding anesthesiologists, radiologists, and pathologists. In 2006, NAMCS included dual frame samples of community health center (CHC) physicians: from the AMA/AOA sample, and from a sample of CHCs. In this report, the 2006 AMA and AOA sample data were combined with 2005 NAMCS data for comparability (12).
NAMCS is a complex sample survey involving a selection of area based primary sampling units (PSUs), a sample of physicians within PSUs, and a sample of visits within physicians’ practice. Physician estimates are based on face-to-face interviews with the physician. In 2005-2006, 4,054 (63.8 percent) of 6,350 sampled physicians were found to be eligible for the survey; of these, 2,592 physicians participated in the Physician Induction Interview, for an unweighted response rate of 63.9 percent. Physician interviews were conducted prior to collecting information from a sample of patient visits during a random week of the year.
Estimates presented in this report are based on 2,390 physicians with information on international medical graduate or U.S. medical graduate status; 6.2 percent of in-scope physicians missing this information were excluded. Visit characteristics are based on 47,023 sampled visits. Weights that take into account all sample stages, with adjustments for nonresponse were used to produce average annual national estimates of physicians and office visits. Differences in physician and visit characteristics for international medical graduate and U.S. medical graduate physicians were analyzed using Chi-square tests.
Selected physician characteristics (physician age, gender, specialty, board certification, and international medical graduate status) are from the AMA or AOA Masterfiles, while other practice characteristics (practice size, ownership, whether new patients were accepted, and percentage of Medicaid revenue) were collected during the physician interview. Physician specialty reported in the Masterfiles was updated during the interview. Information on primary care shortage areas is based on the Health Professional Shortage Areas classification (whole or part county) maintained by the Health Resources and Services Administration’s Bureau of Health Professions on its Area Resource File, and was merged with the NAMCS physician file. Two types of patient characteristics were examined: characteristics of the patient collected from medical records and characteristics of the patients’ neighborhood based on Census Bureau income and demographic characteristics matched by patients’ ZIP Codes.
It should be noted that in computing selected mean characteristics of the patients’ neighborhood, Table 1 excludes cases with missing data. Other patient characteristics analyzed in this report include imputed values for missing data (physician practice size (1.4%), patient race or ethnicity (30.4%), and primary expected payment source (2.4%)). It should be noted that patient race and ethnicity were imputed using new procedures in 2006 (13). Selected percentages by physician characteristics are conservative in that missing data are included in the denominator (physician race or ethnicity (21.6%), whether physician accepts new Medicaid patients (5.8%), and percentage of patient revenue from Medicaid (12.1%). Although nearly one in five physicians was missing information on his or her race or ethnicity, the percentage missing this information was not statistically different between international medical graduates (23.1%) and U.S. medical graduates (19.7%).
References
- Akl EA, Mustafa R, Bdair F, Schunemann HJ. The United States physician workforce and international medical graduates: trends and characteristics. J Gen Intern Med 22(2):264-8. 2007.
- Hart LG, Skillman SM, Fordyce M, Thompson M, Hagopian A, Konrad TR. International medical graduate physicians in the United States: changes since 1981. Health Aff (Millwood) 26 (4):1159-69. 2007.
- Salsberg ES, Forte GJ. Trends in the physician workforce, 1980-2000. Health Aff (Millwood) 21(5): 165-73. 2002.
- Croasdale M. Jinx of the J-1 visa: IMGs finding other paths to residency. AMNews: March 10, 2008. [online]. [cited 2008 Aug 15].
- Cohen, JJ. The role and contributions of international medical graduates: a U.S. perspective. Acad Med, 81(12 Suppl), S17-21. 2006.
- Baer LD, Ricketts TC, Konrad TR, Mick SS. Do international medical graduates reduce rural physician shortages? Med Care 36(11):1534-44. 1998.
- Fink KS, Phillips RL, Fryer GE, Koehn N. International medical graduates and the primary care workforce for rural underserved areas. Health Aff (Millwood) 22(2): 255-62. 2003.
- Mick SS, Lee SY. International and U.S. medical graduates in U.S. cities. J Urban Health 76(4): 481-96. 1999.
- Mullan F, Politzer RM, Davis CH. Medical migration and the physician workforce. International medical graduates and American medicine. JAMA 273(19): 1521-7. 1995.
- Rao NR. Recent trends in psychiatry residency workforce with special reference to international medical graduates. Acad Psychiatry 27(4): 269-76. 2003.
- Koehn NN, Fryer Jr GE, Phillips RL, Miller JB, Green LA. The increase in international medical graduates in family practice residency programs. Fam Med 34(6): 429-35. 2002.
- Hing E, Burt CW. Characteristics of office-based physicians and their practices: United States, 2005-2006. Vital Health Stat 13(166). 2008.
- Cherry DK, Hing E, Woodwell DA, Rechtsteiner EA. National Ambulatory Medical Care Survey: 2006 summary. National health statistics reports; no 3. Hyattsville, MD: National Center for Health Statistics. 2008.
Suggested Citation
Hing E, Lin S. Role of international medical school graduates in providing office-based medical care: United States, 2005-2006. NCHS data brief no 13. Hyattsville, MD: National Center for Health Statistics. 2009.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Director
Edward J. Sondik, Ph.D.
Acting Co-Deputy Directors
Jennifer H. Madans, Ph.D.
Michael H. Sadagursky