Global Rapid Response Team Expands Scope to U.S. Response
February 8, 2021
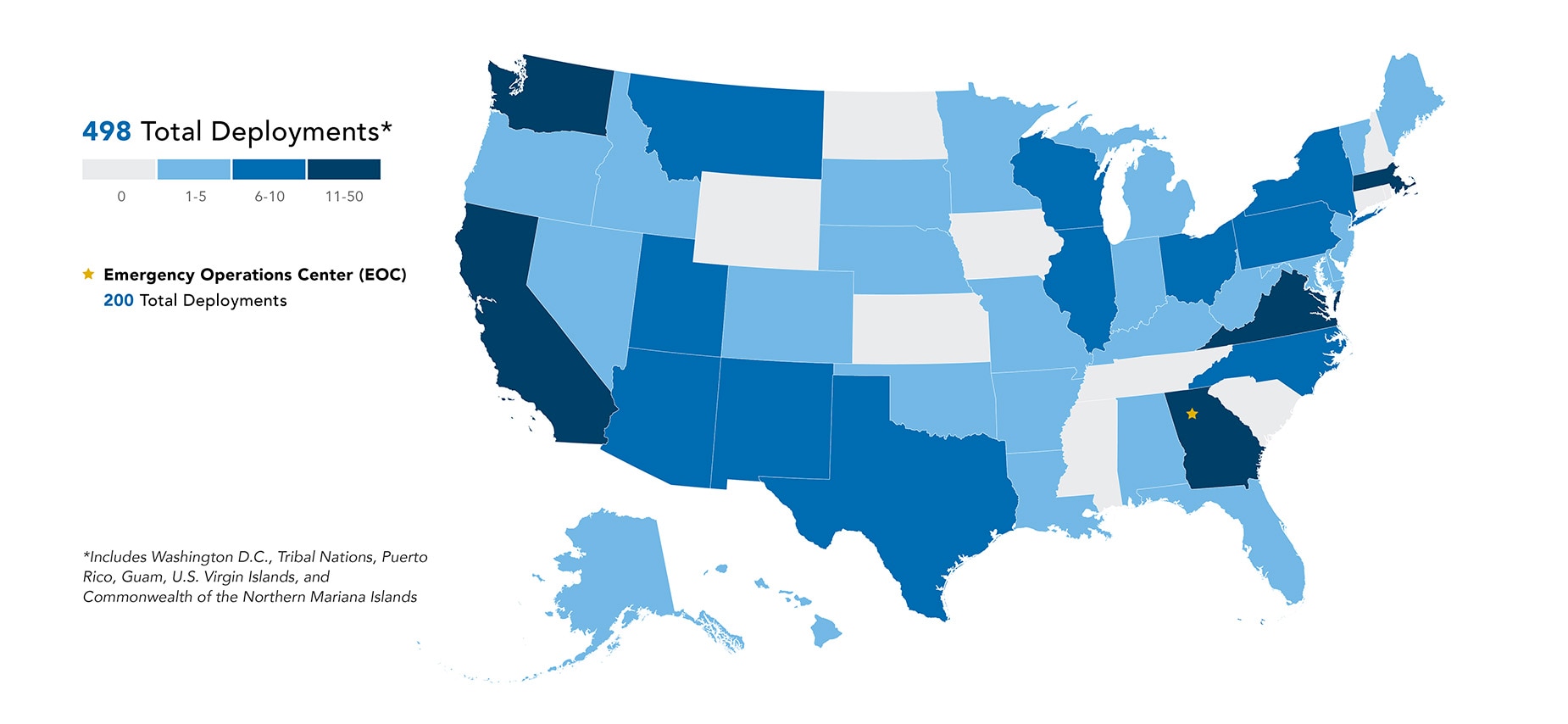
| Number of Deployments | States, Territories, Tribal Nations, and Washington, D.C. |
| 0 | Connecticut, Iowa, Kansas, Mississippi, New Hampshire, North Dakota, Rhode Island, South Carolina, Tennessee, Wyoming |
| 1-5 | Alabama, Alaska, Arkansas, Colorado, Commonwealth of the Northern Mariana Islands, Delaware, Florida, Guam, Hawaii, Idaho, Indiana, Kentucky, Louisiana, Maine, Maryland, Michigan, Minnesota, Missouri, Nebraska, Nevada, New Jersey, Oklahoma, Oregon, South Dakota, Vermont, West Virginia |
| 6-10 | Arizona, Illinois, Montana, New Mexico, New York, North Carolina, Ohio, Pennsylvania, Puerto Rico, Texas, Utah, U.S. Virgin Islands, Wisconsin |
| 11-50 | California, Georgia, Massachusetts, Tribal Nations, Virginia, Washington, and Washington D.C. |
To improve global health security and respond to public health crises, every country needs a dedicated team of trained emergency responders who can quickly mobilize and strengthen their emergency response capacity. In June 2015, during the height of the 2014-2016 Ebola epidemic in West Africa, CDC established the Global Rapid Response Team (GRRT) to support the agency’s response to international emergencies. GRRT brings together well-trained CDC subject matter experts who stand ready to strengthen emergency response capacity whenever and wherever needed and can deploy anywhere in the world within 72 hours. Due to the increased number and gravity of domestic public health emergencies, CDC expanded GRRT’s scope in 2016 to include emergency responses in the United States (U.S.). Since then, GRRT has responded to several domestic public health emergencies including Hurricane Maria in Puerto Rico, Hepatitis A in Appalachia, and the ongoing COVID-19 pandemic. Since 2015, 554 GRRT members have been deployed over 1,300 times for 50,000+ person-days to support 54 countries, including the U.S., during public health emergencies.
GRRT’s Response to COVID-19
At the onset of the COVID-19 pandemic, GRRT members deployed to support surveillance activities in China, repatriation flights from Japan, as well as preparedness and response activities in Asia and Africa. As COVID-19 cases and deaths increased in the U.S., GRRT pivoted from international efforts to support domestic efforts. GRRT COVID-19 responses included
- screening incoming travelers at U.S. quarantine stations,
- conducting outbreak investigations at long-term healthcare facilities, food packing plants, and correctional facilities, and
- providing technical assistance to state health departments and tribal nations.
Since CDC activated its emergency operations center (EOC) to respond to COVID-19 on January 6, 2020, GRRT has deployed over 250 responders on 498 deployments for more than 19,000 person-days to 40 states, Washington D.C., tribal nations, and four territories, as well as CDC’s EOC in Atlanta, Georgia.
GRRT Supports Health Departments in Latinx Communities

Former GRRT responder Jonny Andia (left) and current responder Edgar Monterosso (right) in Richmond, VA, where they conducted contract tracing and determined the current level of COVID knowledge and prevention within Latinx communities (June 2020). Photo: CDC GRRT
As the number of COVID-19 cases continued to rise within the U.S., some communities were unable to bear the burden. CDC identified these disparities and provided community-oriented solutions to reduce illness and death. One example from Virginia involves the Chesterfield County and City of Richmond Health Departments, which noticed many new COVID-19 cases in the Latinx community. To address this public health challenge, GRRT deployed six bilingual emergency responders to support Virginia’s state and local health departments. In Richmond, responders identified economic pressure put people in situations that increased their infection risk. A large portion of the Latinx community worked in service or domestic industries, where they were exposed to other people for long time periods; many lacked health insurance or paid sick leave and feared missing work. To improve health outcomes, GRRT responders helped expand testing and shared health protection and prevention resources in Spanish. GRRT also partnered with local community leaders and associations, providing masks and resources to help those testing positive recover without spreading COVID-19.
“Before COVID-19, I spent 15 years, more than half of my public health career, doing international work… it was COVID-19 that brought all of my international years to bear… [leading me to] investigate COVID-19 transmission dynamics in Latino/Hispanic communities across the USA. My international work and GRRT deployments helped me develop the sensitivities and awareness [needed] to approach affected [domestic] communities. For me, a valuable lesson has been to once again realize that all public health is local; responses and action start at the local level in the U.S. and wherever we may be asked to respond.” – Dr. Edgar Monterroso, MD MPH
Value and Future Directions of GRRT
Today, as COVID-19 and other public health crises continue to emerge and strain even the most established public health systems, GRRT’s capacity to rapidly mobilize and pivot from international to domestic response exponentially increases its value to global health security. Moving forward, GRRT’s priorities for the 2021-2022 calendar year include increasing GRRT’s surge roster of as-needed responders by 50%, and continuing to provide expertise in epidemiology, community engagement, laboratory, logistics, and more to address health disparities worldwide and ensure a safer, more equitable future for all.
“The broad skillset and flexibility of GRRT staff is one of CDC’s biggest assets in response to both international and domestic outbreaks,” said Dr. Henry Walke, COVID-19 Incident Manager and former Ebola Virus Disease Incident Manager. “GRRT responders never hesitate to deploy at short notice… I appreciate their dedication and enthusiasm to protecting public health domestically and internationally.”