On August 2, 2011, this report was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr).
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Vital Signs: Hospital Practices to Support Breastfeeding --- United States, 2007 and 2009
Abstract
Background: Childhood obesity is a national epidemic in the United States. Increasing the proportion of mothers who breastfeed is one important public health strategy for preventing childhood obesity. The World Health Organization and United Nations Children's Fund (UNICEF) Baby-Friendly Hospital Initiative specifies Ten Steps to Successful Breastfeeding that delineate evidence-based hospital practices to improve breastfeeding initiation, duration, and exclusivity.
Methods: In 2007 and 2009, CDC conducted a national survey of U.S. obstetric hospitals and birth centers. CDC analyzed these data to describe the prevalence of facilities using maternity care practices consistent with the Ten Steps to Successful Breastfeeding.
Results: In 2009, staff members at most hospitals provide prenatal breastfeeding education (93%) and teach mothers breastfeeding techniques (89%) and feeding cues (82%). However, few hospitals have model breastfeeding policies (14%), limit breastfeeding supplement use (22%), or support mothers postdischarge (27%). From 2007 to 2009, the percentage of hospitals with recommended practices covering at least nine of 10 indicators increased only slightly, from 2.4% to 3.5%. Recommended maternity care practices vary by region and facility size.
Conclusion: Most U.S. hospitals have policies and practices that do not conform to international recommendations for best practices in maternity care and interfere with mothers' abilities to breastfeed.
Implications for Public Health Practice: Hospitals providing maternity care should adopt evidence-based practices to support breastfeeding. Public health agencies can set quality standards for maternity care and help hospitals achieve Baby-Friendly designation. Because nearly all births in the United States occur in hospitals, improvements in hospital policies and practices could increase rates of exclusive and continued breastfeeding nationwide, contributing to improved child health, including lower rates of obesity.
Introduction
Obesity is a national epidemic in the United States, and children are not exempt. Currently, 21% of children aged 2--5 years are at least overweight, and half of those children are obese (1). Obese children and adolescents are more likely to have elevated cholesterol and blood pressure levels, breathing and joint problems, and to become obese adults (2). Substantial epidemiologic evidence now establishes breastfeeding as an important public health strategy for preventing childhood obesity (3). In a meta-analysis, children who were breastfed had reduced odds for obesity at various ages compared with those who were formula fed (4). In a separate meta-analysis, children breastfed for 9 months had a more than 30% reduced odds of becoming overweight compared with children never breastfed, and the two studies that examined exclusive breastfeeding showed a stronger effect (5). Breastfeeding affords infants and mothers additional benefits. When mothers formula feed or discontinue breastfeeding early, the risk for infectious illnesses in their children is increased, as is the mother's risk for developing breast and ovarian cancer (6).
The American Academy of Pediatrics recommends exclusive breastfeeding (breast milk with no solids or other liquids except vitamin/mineral supplements or medications) for about the first 6 months of infancy, and then continued breastfeeding, along with the introduction of iron-rich foods, for at least the first year of an infant's life (7). Although approximately 80% of women in the United States indicate before delivery that they intend to breastfeed (8), and 75% initiate breastfeeding, at 1 week half of women have already given their infant formula, and only 31% are breastfeeding to any extent at 9 months (9).
For women who plan to breastfeed, experiences and support during the first hours and days after birth influence their later ability to continue breastfeeding. Because nearly all U.S. births occur in hospitals, policies that determine hospital practices can influence the feeding behaviors of more than 11,000 infants born each day.* In 1991, the World Health Organization (WHO) and United Nations Children's Fund (UNICEF) developed the Baby-Friendly Hospital Initiative,† the core of which is the Ten Steps to Successful Breastfeeding. These evidence-based steps outline best practices in hospital settings to help mothers initiate and continue breastfeeding, thus increasing exclusivity and duration of breastfeeding well beyond the hospital stay (10). In one study of women who intended to breastfeed for longer than 2 months, 30% of them stopped breastfeeding early if they experienced none of the Ten Steps to Successful Breastfeeding in the hospital, compared with only 3% who experienced six steps (11). The American Academy of Pediatrics endorsed the Ten Steps to Successful Breastfeeding in 2009 and the White House Task Force on Childhood Obesity Report to the President recommended improving maternity care practices in 2010 (3). This report uses data from the national Maternity Practices in Infant Nutrition and Care (mPINC) survey to describe maternity care practices in the United States.§
Methods
In 2007, CDC began the biennial mPINC survey to characterize U.S. maternity practices related to breastfeeding. The mPINC is a census survey, assessing practices at all facilities in all states, the District of Columbia, and four U.S. territories that provide maternity services. In 2007, a total of 2,690 facilities participated, and 2,672 facilities participated in 2009; the response rate each time was 82%. Because 96% of respondents in both survey years were hospitals, with the remaining respondents being free-standing birth centers, in this report the term "hospital" refers to all respondents. The mPINC survey is mailed to each hospital and completed by a key informant identified in advance via a screening telephone call as the person best able to answer questions about infant feeding routines. Data from 2007 and 2009 were analyzed for 10 indicators consistent with WHO/UNICEF's Ten Steps to Successful Breastfeeding: 1) existence of a model breastfeeding policy,¶ 2) staff competency assessment, 3) prenatal breastfeeding education, 4) early initiation of breastfeeding, 5) teaching breastfeeding techniques, 6) limited supplementation of breastfeeding infants, 7) rooming-in, 8) teaching feeding cues, 9) limited use of pacifiers, and 10) post-discharge support.** The prevalence of hospitals with recommended policies and practices in 2007 and 2009 for each of the 10 indicators were assessed. Data for 2009 were analyzed to describe variations by geographic area and hospital annual number of births. Because the mPINC survey is a census rather than a sample, no statistical tests were conducted.
Results
In 2009, most hospitals reported providing prenatal breastfeeding education (92.8%), teaching women breastfeeding techniques (89.1%), and teaching women how to recognize and respond to infant feeding cues (81.8%) (Table 1). For all other indicators, half or fewer hospitals followed recommended practices. The lowest prevalence of recommended practices related to having a model breastfeeding policy (14.4%); limiting use of formula, water, or glucose supplements for healthy, full-term breastfed infants (21.5%); and providing adequate breastfeeding support to breastfeeding mothers at hospital discharge (26.8%). From 2007 to 2009, the percent of hospitals implementing recommended practices improved at least 1 percentage point for seven indicators, but less than 1 percentage point for three indicators. The majority of hospitals were implementing three to five recommended practices (60.5% in 2007 and 54.3% in 2009), with only 2.4% of hospitals implementing at least nine recommended practices in 2007, and 3.5% in 2009 (Figure). Fewer than 1% of hospitals implemented all 10 policies and practices either year.
The Northeast had the highest prevalence of hospitals with recommended practice for most indicators (Table 2). However, even in the Northeast, the prevalence of recommended practice exceeded 50% for only six indicators, and only 32% of hospitals had a model breastfeeding policy. Although the Mountain Plains and Southwest regions each had the lowest prevalence of recommended practice on each of several indicators, no specific region was consistently the lowest across all indicators.
Larger hospitals were more likely to have model breastfeeding policies. Despite such policies, the largest hospitals (≥5,000 births annually) had the lowest prevalence of recommended practice on each of several indicators, including only 7.9% with limited hospital use of breastfeeding supplements (Table 2). The prevalence of recommended practice on institutional indicators, including having a model policy, assessing staff breastfeeding competency, and providing prenatal breastfeeding education, was lower among smaller hospitals. However, smaller hospitals had a higher prevalence of adherence to recommended practice on other indicators, including early initiation of breastfeeding, limited use of supplements, rooming-in, and providing discharge care.
Conclusions and Comment
Improving breastfeeding rates is one strategy to address childhood obesity. For women who intend to breastfeed, the hospital experience is critical. These data illustrate the persistent use of practices that are inconsistent with best-practice standards and do not support breastfeeding. To give infants the best start in achieving a healthy life, including reduced obesity, mothers must be supported immediately after birth to establish breastfeeding. Suboptimal breastfeeding in the United States annually results in an estimated $2.2 billion in additional direct medical costs (12). Recognizing the important role of hospitals in helping women begin breastfeeding, Healthy People 2020 added two objectives related to breastfeeding and maternity care: reducing the proportion of breastfed newborns who receive formula supplementation within the first 2 days of life (MICH-23), and increasing the proportion of live births that occur in facilities that provide recommended care for lactating mothers and their babies (MICH-24) (13). Even infants of mothers who choose to feed their infants both breast milk and formula should not be given formula in the hospital unless medically indicated, as hospital supplementation is associated with early discontinuation of breastfeeding (14). Recognizing exclusive breastfeeding as a quality-of-care issue, the Joint Commission, the organization that accredits and certifies U.S. hospitals, added exclusive breast milk feeding in the hospital as a new quality of care measure in 2010 (15).
The Baby-Friendly Hospital Initiative recognizes hospitals with best practices in supporting breastfeeding. To be designated as Baby-Friendly, a hospital must implement the WHO/UNICEF Ten Steps to Successful Breastfeeding and comply with the International Code of Marketing of Breast-milk Substitutes, which requires hospitals to pay fair market value for infant formula and not promote items detrimental to breastfeeding, including discharge bags that contain formula (16). The percent of U.S. infants born at Baby-Friendly hospitals increased from 1.8% in 2007 to 4.5% in 2011 (17).
The mPINC survey assesses the Ten Steps to Successful Breastfeeding using a key informant interview, a methodology that is not directly comparable to the Baby-Friendly designation process, which incorporates direct observation and interviews with mothers. However, reports from the mPINC survey provide all hospitals an opportunity to identify practices that inhibit mothers' abilities to breastfeed. Every hospital that participates in the mPINC survey receives a report of its own results showing how its practices compare with recommended practices and with practices of hospitals around the country. These reports can help hospitals develop and implement a plan to improve care to better support breastfeeding, with the goal of preparing hospitals to move more quickly toward Baby-Friendly designation.
A strong breastfeeding policy is the foundation of quality hospital breastfeeding support and sets standards for the remaining nine steps. These data illustrate that in most states few hospitals have established breastfeeding policies that fully support and encourage mothers to breastfeed. The Northeast had the highest prevalence of having a model policy and also the highest prevalence of recommended practice on many indicators. However, policy does not necessarily indicate practice. To improve practice, hospitals will need to ensure that staff members are sufficiently trained to carry out strong breastfeeding policies, and routinely assess adherence.
Although hospital support is critical for helping mothers establish breastfeeding, it is not the only support needed to help them continue breastfeeding. As documented in the Surgeon General's Call to Action to Support Breastfeeding, families, communities, employers, health-care providers, and government and nonprofit agencies all have critical roles to play (18). Ongoing efforts and initiatives in these areas include the Affordable Care Act, which amended the Fair Labor Standards Act to require employers with more than 50 employees to provide reasonable break time and a private location (other than a bathroom) for breastfeeding mothers to express milk.†† Additionally, the U.S. Department of Agriculture's Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), which supports approximately 50% of all infants born in the United States, recently revised its program to support breastfeeding more effectively by modifying the mother's food package to be more supportive of women who are breastfeeding, and increasing peer counseling support for breastfeeding.§§ CDC produces an annual Breastfeeding Report Card, which provides state-level data on breastfeeding rates and key types of community breastfeeding support, showing where states have been successful and where more work is needed to promote and support breastfeeding.¶¶
The findings in this report are subject to at least two limitations. The survey was completed by one key informant at each hospital and might not accurately reflect actual hospital practices. To ensure data were as valid as possible, CDC requested that the survey be completed by the person most knowledgeable of the hospital's maternity practices, in consultation with other knowledgeable persons, as needed. Second, although more than 80% of hospitals participated in each survey, practices in those that participated and those that did not might differ.
Hospitals provide care to nearly all women giving birth in the United States; however, in most hospitals, this care falls short of evidence-based best practices that fully support mothers to be able to breastfeed. Systematically improving maternity care practices, including increased adherence to the Ten Steps to Successful Breastfeeding, will help women who intend to breastfeed get the support they need to be able to start and continue breastfeeding, and by so doing, reduce child obesity and improve other aspects of child health.
Reported by
Cria G. Perrine, PhD, Katherine R. Shealy, MPH, Kelley S. Scanlon, PhD, Laurence M. Grummer-Strawn, PhD, Deborah A. Galuska, PhD, Div of Nutrition, Physical Activity, and Obesity; Deborah L. Dee, PhD, Div of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion; CDC. Jennifer H. Cohen, PhD, Battelle Centers for Public Health Research and Evaluation, Seattle, WA. Contributing correspondent: Cria G. Perrine, CDC, 770-488-5183, cperrine@cdc.gov.
Acknowledgments
Hospitals and birth centers that participated in the mPINC survey. Persons involved in developing and implementing the survey.
References
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in U.S. children and adolescents, 2007--2008. JAMA 2010;303:242--9.
- Reilly JJ, Methven E, McDowell ZC, et al. Health consequences of obesity. Arch Dis Child 2003;88:748--52.
- White House Task Force on Childhood Obesity. Solving the problem of childhood obesity within a generation. Washington, DC: The White House; 2010. Available at http://www.letsmove.gov/white-house-task-force-childhood-obesity-report-president. Accessed June 30, 2011.
- Owen CG, Martin RM, Whincup PH, Davey Smith G. Effect of infant feeding on the risk of obesity across the life course: a quantitative review of published evidence. Pediatrics 2005;115:1367--77.
- Harder T, Bergmann R, Kallischnigg G, Plagemann A. Duration of breastfeeding and risk of overweight: a meta-analysis. Am J Epidemiol 2005;162:397--403.
- Ip S, Chung M, Raman G, et al. Breastfeeding and maternal and infant health outcomes in developed countries. Rockville, MD: Agency for Healthcare Research and Quality; 2007.
- Gartner LM, Morton J, Lawrence RA, et al. Breastfeeding and the use of human milk. Pediatrics 2005;115:496--506.
- Declercq ER, Sakala C, Corry MP, Applebaum S. Listening to mothers II: report of the Second National U.S. Survey of Women's Childbearing Experiences. New York, NY: Childbirth Connection; 2006.
- CDC. Breastfeeding among U.S. children born 2000--2008, CDC National Immunization Survey. Atlanta, GA: US Department of Health and Human Services, CDC; 2010. Available at http://www.cdc.gov/breastfeeding/data/NIS_data/index.htm. Accessed July 8, 2011.
- Kramer MS, Chalmers B, Hodnett ED, et al. Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus. JAMA 2001;285:413--20.
- DiGirolamo AM, Grummer-Strawn LM, Fein SB. Effect of maternity-care practices on breastfeeding. Pediatrics 2008;122:s43--9.
- Bartick M, Reinhold A. The burden of suboptimal breastfeeding in the United States: a pediatric cost analysis. Pediatrics 2010;125:e1048--56.
- US Department of Health and Human Services. Healthy People 2020: Maternal, Infant, and Child Health Objectives. Available at http://www.healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicid=26. Accessed May 20, 2011.
- World Health Organization. Evidence for the ten steps to successful breastfeeding. Geneva, Switzerland: World Health Organization; 1998.
- Joint Commission. Specifications manual for Joint Commission National Quality Care Measures: perinatal care. Available at http://manual.jointcommission.org/releases/TJC2011A/PerinatalCare.html. Accessed May 20, 2011.
- World Health Organization. International code of marketing of breast-milk substitutes. Geneva, Switzerland: World Health Organization; 1981.
- CDC. Breastfeeding report card---United States, 2011. Atlanta, GA: US Department of Health and Human Services, CDC; 2011. Available at http://www.cdc.gov/breastfeeding/data/reportcard.htm. Accessed August 1, 2011.
- US Department of Health and Human Services. The Surgeon General's call to action to support breastfeeding. Washington, DC: US Department of Health and Human Services, Office of the Surgeon General; 2011.
* National Vital Statistics System birth data available at http://www.cdc.gov/nchs/births.htm.
† Additional information available at http://www.babyfriendlyusa.org/eng/03.html.
§ Additional information available at http://www.cdc.gov/breastfeeding/data/mpinc/index.htm.
¶ A model breastfeeding policy includes all of the following elements: 1) in-service training, 2) prenatal breastfeeding classes, 3) asking about mothers' feeding plans, 4) initiating breastfeeding within 1 hour of uncomplicated vaginal birth, 5) initiating breastfeeding after recovery for uncomplicated cesarean deliveries and/or showing mothers how to express milk and maintain lactation if separated from infant, 6) giving only breast milk to breastfed infants, 7) rooming-in 24 hours/day, 8) breastfeeding on demand, 9) no pacifier use by breastfed infants, and 10) referral of mothers with breastfeeding problems and/or referral of mothers to appropriate breastfeeding resources at discharge. Inclusion of these elements was derived from the Academy of Breastfeeding Medicine's Model Breastfeeding Policy. Additional information available at http://www.bfmed.org/Media/Files/Protocols/English%20Protocol%207%20Model%20Hospital%20Policy.pdf.
** Strategies include home visit and hospital postpartum follow-up visit (physical contact); follow-up telephone call after discharge (reaching out); and hospital telephone number to call, hospital-based support group, other breastfeeding support group, lactation consultant, etc. (referrals).
†† Patient Protection and Affordable Care Act (as amended through May 1, 2010). Pub, L, No. 114--48. Available at http://docs.house.gov/energycommerce/ppacacon.pdf.
§§ Additional information available at http://www.fns.usda.gov/wic/breastfeeding/mainpage.htm.
¶¶ Additional information available at http://www.cdc.gov/breastfeeding/data/reportcard.htm.
|
Key Points |
|
FIGURE. Percentage of hospitals that implemented recommended maternity care practices related to breastfeeding* --- Maternity Practices in Infant Nutrition and Care Survey (mPINC), United States, 2007 and 2009
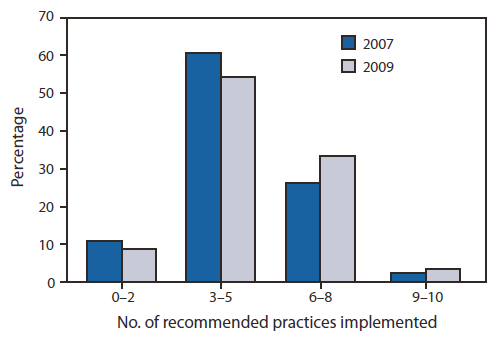
* Recommended maternity care practices are indicators of the Ten Steps to Successful Breastfeeding (available at http://www.babyfriendlyusa.org/eng/10steps.html), as measured in the mPINC survey.
Alternate Text: The figure above shows the percentage of U.S. hospitals that implemented recommended maternity care practices related to breastfeeding in 2007 and 2009, based on results from the Maternity Practices in Infant Nutrition and Care Survey (mPINC). From 2007 to 2009, the percent of hospitals implementing recommended practices improved at least 1 percentage point for seven indicators, but less than 1 percentage point for three indicators. The majority of hospitals were implementing three to five recommended practices (60.5% in 2007 and 54.3% in 2009), with only 2.4% of hospitals implementing at least nine recommended practices in 2007, and 3.5% in 2009.
|
TABLE 2. Percentage of hospitals that had implemented recommended practices on indicators consistent with the Ten Steps to Successful Breastfeeding,* by region and hospital annual births --- Maternity Practices in Infant Nutrition and Care (mPINC) Survey, United States, 2009 |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
Steps implemented |
||||||||||
|
Hospital location/births |
Participants (%) |
1. Model breastfeeding policy (%) |
2. Staff competency assessment (%) |
3. Prenatal breastfeeding education (%) |
4. Early initiation of breastfeeding (%) |
5. Teach breastfeeding technique (%) |
6. Limited use of breastfeeding supplements (%) |
7. Rooming-in (%) |
8. Teach feeding cues (%) |
9. Limited use of pacifiers (%) |
10. Post-discharge support (%) |
|
Region† |
|||||||||||
|
Western |
16.4 |
15.7 |
49.4 |
90.4 |
59.1 |
87.4 |
26.8 |
67.9 |
81.7 |
42.8 |
26.7 |
|
Southwest |
13.0 |
11.9 |
48.0 |
82.4 |
39.1 |
84.9 |
17.5 |
40.1 |
77.9 |
29.2 |
20.4 |
|
Southeast |
16.6 |
10.3 |
55.1 |
93.6 |
42.6 |
89.0 |
12.7 |
26.8 |
80.3 |
23.3 |
21.7 |
|
Northeast |
9.2 |
31.8 |
64.8 |
97.6 |
58.5 |
93.1 |
27.3 |
23.7 |
91.1 |
51.2 |
34.0 |
|
Mountain Plains |
14.9 |
8.1 |
38.1 |
92.6 |
55.6 |
87.3 |
23.4 |
28.5 |
75.8 |
18.2 |
31.7 |
|
Midwest |
20.2 |
15.4 |
45.6 |
97.7 |
51.7 |
91.4 |
22.6 |
20.3 |
84.3 |
24.4 |
31.2 |
|
Mid-Atlantic |
9.8 |
13.0 |
54.7 |
94.1 |
50.6 |
92.3 |
21.7 |
19.5 |
84.9 |
32.1 |
20.8 |
|
Annual births |
|||||||||||
|
<250 |
22.5 |
7.0 |
33.2 |
83.7 |
61.6 |
85.7 |
38.7 |
47.0 |
77.9 |
40.7 |
34.6 |
|
250--499 |
17.2 |
11.6 |
41.8 |
90.4 |
54.1 |
89.4 |
21.1 |
27.2 |
83.0 |
23.4 |
27.5 |
|
500--999 |
20.8 |
11.8 |
51.6 |
95.4 |
49.2 |
88.8 |
17.5 |
29.9 |
79.8 |
25.0 |
23.8 |
|
1,000--1,999 |
19.9 |
19.2 |
61.6 |
97.5 |
49.1 |
91.5 |
16.7 |
27.1 |
86.3 |
26.7 |
27.3 |
|
2,000--4,999 |
17.4 |
22.7 |
60.8 |
97.2 |
39.7 |
90.7 |
11.5 |
32.7 |
83.1 |
31.9 |
20.3 |
|
≥5,000 |
2.4 |
25.0 |
63.5 |
100.0 |
38.7 |
90.5 |
7.9 |
30.7 |
82.5 |
41.3 |
17.5 |
|
* Recommended maternity care practices are indicators of the Ten Steps to Successful Breastfeeding (available at http://www.babyfriendlyusa.org/eng/10steps.html), as measured in the mPINC survey. † Western = Alaska, American Samoa, Arizona, California, Guam, Hawaii, Idaho, Nevada, Oregon, Washington; Southwest = Arkansas, Louisiana, New Mexico, Oklahoma, Texas; Southeast = Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, Tennessee; Northeast = Connecticut, Maine, Massachusetts, New Hampshire, New York, Rhode Island, Vermont; Mountain Plains = Colorado, Iowa, Kansas, Missouri, Montana, Nebraska, North Dakota, South Dakota, Utah, Wyoming; Midwest = Illinois, Indiana, Michigan, Minnesota, Ohio, Wisconsin; Mid-Atlantic = Delaware, District of Columbia, Maryland, New Jersey, Pennsylvania, Puerto Rico, Virginia, U.S. Virgin Islands, West Virginia. |
|||||||||||
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
