About
In alignment with CDC’s Division of Viral Hepatitis 2025 Strategic Plan, the Viral Hepatitis National Progress Report provides information on progress toward 2025 goals for new viral hepatitis infections and viral hepatitis-related deaths, overall and for key populations.
Progress
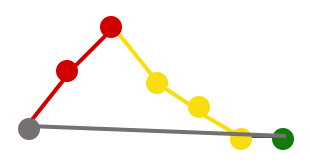
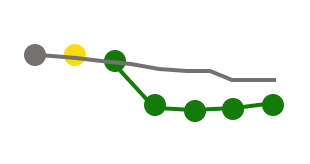
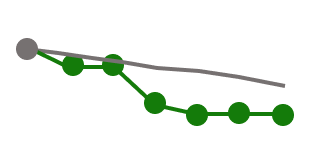
Ten objective indicators assess progress toward achieving key viral hepatitis goals.

Met or exceeded current annual target

Moving toward annual target, but annual target was not fully met

Has moved away from annual target or has not changed





Related content
See the 2023 Viral Hepatitis Surveillance Report, published by CDC’s Viral Hepatitis Program
See list of all viral hepatitis surveillance reports, surveillance guidelines, and national progress
Explore the CDC’s 2025 goals and strategies to reduce hepatitis infections, viral hepatitis-related.
Content Source:
Division of Viral Hepatitis
- Klevens RM, Liu S, Roberts H, et al. Estimating acute viral hepatitis infections from nationally reported cases. Am J Public Health 2014;104:482. PMC3953761.