At a glance
Model & tool development
This interactive tool was developed to support the 2025 measles response. The underlying model is based on the latest information from the literature on parameters that influence transmission of measles and input from CDC subject-matter experts. The model has both been reviewed by internal measles and modeling experts and shared with external experts for their individual input. We will continue to update and improve the tool as more information becomes available, and in support of ongoing response needs.
Versions
- Version 2.0.1 was published on July 13, 2026, on a new platform improving the speed and functionality of the simulator and allows users to alter the number of simulations run and the length of simulations.
- Version 1.0.2 was published on February 20, 2026, incorporating a new baseline immunity calculator feature, reducing the minimum population size, and allowing users to download simulation results.
- Version 1.0.1 was published on July 28, 2025.
Resources
- The code for the tool can be found in our public GitHub repository.
- The key takeaways from the tool can be found in this downloadable summary.
- More detailed methods, results, and takeaways can be found in our Behind the Model - Interactive Measles Outbreak Simulator.
FAQs
The baseline immunity is the overall proportion of the population that has immunity to measles, through either up-to-date MMR vaccination or prior infection, before the simulation starts (i.e. before infection or vaccination that occurs in the simulation). A simple approach to estimating the level of immunity would be to estimate the number of people vaccinated with MMR (1 or 2 doses) or previously infected with measles, then divide this by the total population size. The model will account for the vaccine effectiveness or VE (see VE of MMR for measles) and assume 3% (e.g., 100% - 97%) of those labeled as "immune" at baseline are still susceptible.
However, data on the total number of people with immunity in a community is often not available. For this reason, we have added a Baseline Immunity Calculator in the latest update to the simulator, which can be found in a dropdown below the baseline immunity entry field. This calculator allows users to input data on prior infection and/or MMR coverage values for standard time points (24 months, kindergarten entry, and seventh grade) that are frequently available to public health practitioners, and generates an estimate of the population's overall immunity to measles. If data are not available for all years, users can also estimate coverage using the most recent data available for those age cohorts (e.g. using kindergarten MMR coverage values from the year current 7th graders were entering kindergarten).
The calculator also accounts for the distribution of age groups in the community, which can be found at the state or county level in the census. While the inputs to the baseline immunity calculator are age-stratified in order to get a better estimate of total population immunity, the underlying transmission model is not age-stratified. For more information about the methods we used in this calculator, please see our Behind the Model.
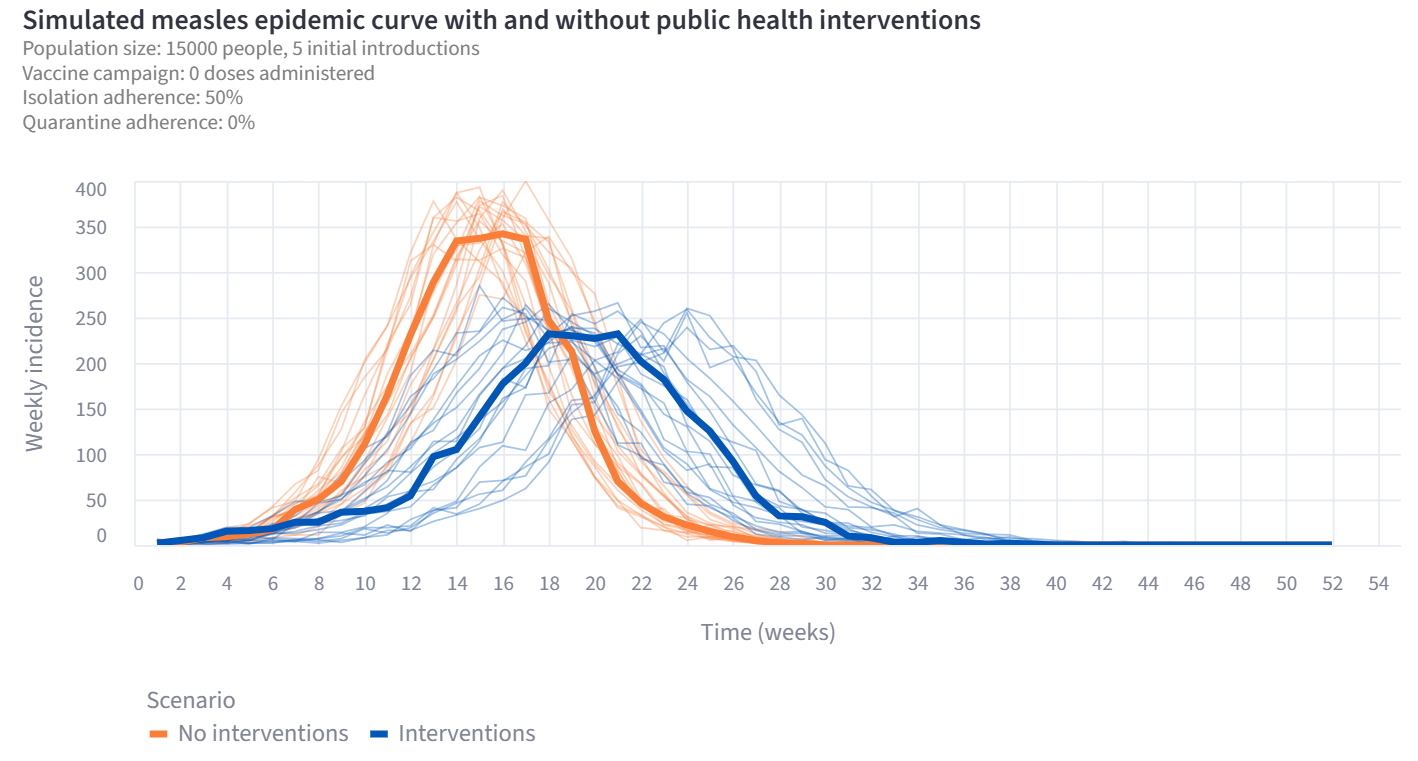
Based on observations from field investigations, if a person is quarantining after a potential exposure, they will also generally isolate upon rash onset. People who do not quarantine still may isolate, so in the model, adherence to isolation is always at least as high as adherence to quarantine, but may be higher.
If turned on, quarantine reduces transmission rates by 60% among infectious individuals who are adhering in the first half of their infectious periods, before they have symptoms of measles. Similarly, isolation reduces transmission rates to zero among infectious individuals who are adhering later in their infectious period, after they are symptomatic.
The vaccine is assumed to be “all or nothing”, meaning that it either confers perfect immunity or no immunity. The proportion with immunity is determined by the VE parameter.
The model calculates the rate of doses administered as the number of people expected to be vaccinated (given eligibility and the percent of eligible population who get vaccinated) divided by the duration of the vaccine campaign. If the user defines a campaign scheduled to end after the end of the simulation, then the campaign ends early (on the last day, day 365).
For example, a campaign to vaccinate 100% of eligible people in a population of 100,000 people and 95% baseline immunity would theoretically vaccinate 4,999 people. However, if this campaign is planned to start on day 180 in the model and last for 365 days, only approximately half (2,534) of those people will actually receive the vaccine during the simulation.
The model used in this simulator is not set up to represent outbreaks in congregate settings, such as schools and day cares. This tool is designed for communities of size 1000-100,000 and assumes a well-mixed population. These assumptions often do not apply to congregate settings, which are typically smaller and/or have more complex mixing patterns. However, other tools have been developed by CDC partners that focus specifically on outbreaks in school settings. Two interactive simulators of measles outbreaks in schools have been developed recently, one by researchers at UT Austin and one by the Utah DHHS and the ForeSITE group. Modeling was also used to support the response to a measles outbreak in a shelter in Chicago in 2024.
The simulator results show the total number of infections in the modeled population, not the total number of reported cases, which means that the results do not account for incomplete reporting. Reporting rates vary depending on the context of each outbreak and should be accounted for separately when considering measles outbreak data.
The default baseline immunity value was chosen to highlight the impact of combining interventions when baseline immunity to measles is particularly low. However, all population parameters are modifiable by the user, so the default parameters should be considered place holders for the true values in the community of interest. The baseline immunity calculator can also be used to help estimate this value for your community.
Cost-benefit analyses of measles interventions are highly context dependent. In a review of the costs associated with measles outbreaks in the United States between 2004 and 2017, the median cost per measles outbreak was $181,823 (ranging from $11,773 to $1.3 million), and the median cost per measles case was $39,1621. Costs can rise rapidly when outbreaks are large, such as the 2019 outbreak in New York City, which had 149 cases, costing $10.6 million2, or considering costs beyond response and containment, such direct medical costs and productivity losses, such as in the 2019 outbreak in Washington State, which had 72 cases, costing $4.3 million3. The simulator estimates the benefits in terms of avoided number of hospitalizations that occur in scenarios with interventions compared to scenarios without interventions. When considering the overall impact of measles outbreak interventions, it is also important to consider other outcomes of measles infections avoided due to the intervention, such as death and productivity losses due to isolation or quarantine. All costs are converted to 2025 US dollars.
- Pike J, Leidner AJ, Gastañaduy PA. A Review of Measles Outbreak Cost Estimates From the United States in the Postelimination Era (2004-2017): Estimates by Perspective and Cost Type. Clin Infect Dis. 2020;71(6):1568-1576. doi:10.1093/cid/ciaa070
- Pike J, Melnick A, Gastañaduy PA, et al. Societal Costs of a Measles Outbreak. Pediatrics. 2021;147(4):e2020027037. doi:10.1542/peds.2020-027037
- Zucker JR, Rosen JB, Iwamoto M, et al. Consequences of Undervaccination - Measles Outbreak, New York City, 2018-2019. N Engl J Med. 2020;382(11):1009-1017. doi:10.1056/NEJMoa1912514