Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Renewed Transmission of Dracunculiasis --- Chad, 2010
Transmission of dracunculiasis (Guinea worm disease), a waterborne, parasitic disease targeted for eradication, was thought to have been interrupted in Chad since 2000, when the last case was reported. However, in 2010, 10 cases were confirmed by the Chad Ministry of Public Health (Ministère de la Santé Publique [MSP]) and the World Health Organization (WHO) during field investigations in which rumored cases were investigated and nearby villages were actively searched for additional cases. Because patients were not prevented from contaminating water sources, new cases were expected in 2011. During January--February 2011, MSP, WHO, and CDC conducted an investigation to gather additional information to guide prevention and response activities before the 2011 transmission season. Seven districts where cases had been confirmed or suspected in 2010 or where dracunculiasis was endemic during 1994--2000 were surveyed. The results of those surveys indicated that residents of 116 (55%) of 210 villages and 13 (87%) of 15 nomad camps consumed water from unsafe sources; 157 (75%) of 209 village key informants (KIs) and five (33%) of 15 nomad camp KIs knew about dracunculiasis. Thirty-one villages had confirmed or suspected cases during 2009--2011 and were classified as at-risk, requiring weekly active surveillance and urgent pre-positioning of materials for the 2011 transmission season. Nomadic populations are at risk for dracunculiasis because of unsafe water consumption and minimal knowledge of the disease. These populations also require targeted surveillance and prevention efforts (e.g., filter distribution, education, and case containment*) to interrupt dracunculiasis transmission (1).
Dracunculiasis is transmitted by drinking unsafe† stagnant water contaminated by copepods (water fleas) that contain Dracunculus medinensis larvae. The copepods are digested in the human gastrointestinal tract and release the larvae, which penetrate the gut wall. The larvae mate, and pregnant female worms mature in connective tissues, growing to 2--3 feet (70--100 centimeters) in length. Approximately 10--14 months after initial ingestion, the female Guinea worm creates a painful burning blister on the patient's skin. When this lesion is bathed in water to ease the symptoms, the worm emerges and ejects larvae into the water, which are ingested by copepods, starting the cycle anew.
To manage the illness, the emerging worm is removed by rolling it around gauze or a stick a few centimeters per day; extraction is painful and can take weeks. Antibiotic ointment may be applied to the lesion to prevent secondary bacterial infections that can result in cellulitis, septic arthritis, joint contractures, and permanent disability. Currently, no effective drug to treat or vaccine to prevent dracunculiasis is available, and persons who contract dracunculiasis do not become immune (2,3). Dracunculiasis can be prevented by 1) educating patients with emerging worms to avoid bathing affected body parts in drinking water sources, 2) filtering potentially contaminated drinking water through cloth or pipe filters, 3) treating potentially contaminated stagnant drinking water with a larvicide such as temephos (e.g., Abate), 4) providing safe drinking water, and 5) detecting cases before the worm emerges to prevent patients with emerging worms from contaminating water supplies (4).
During April--June 2010, two rumored dracunculiasis cases were reported to Chad's National Guinea Worm Eradication Program (NGWEP). Cases were confirmed upon investigation, and extracted worms were further verified as D. medinensis at CDC by polymerase chain reaction (PCR) testing (5). Subsequently, NGWEP initiated an outbreak response with the assistance of WHO, which used house-to-house surveys to search for cases in all villages with confirmed, suspected, or rumored 2010 cases and in villages visited by patients during the 10--14 month incubation period preceding worm emergence. A rumored case was defined as an alleged dracunculiasis case based on any information obtained from any source (6); a suspected case was defined as a rumored case investigated by MSP or the investigation team with a history, reported by the patient or family, consistent with dracunculiasis but without an observed worm; a confirmed case was defined as any case with a history, reported by the patient or family, consistent with dracunculiasis and with a worm observed by MSP or the investigation team. KIs in neighboring villages also were interviewed. Additional house-to-house surveys later were conducted as part of poliomyelitis vaccination campaigns.
By October 2010, surveys, awareness campaigns, and increased surveillance had uncovered eight additional cases, all confirmed by worm collection (three cases were further verified by PCR testing at CDC). The 10 confirmed cases were located in eight different villages in five districts, within four regions of Chad (Figure). Six of the eight villages border the Chari River. Because of late detection, none of the 10 patients were prevented from contaminating drinking water sources; therefore, continued transmission was expected during the 2011 dracunculiasis transmission season, typically the April--October rainy season in Chad, when many villages are not accessible by road from the capital.
On December 22, 2010, MSP and WHO requested CDC assistance in conducting a dracunculiasis outbreak investigation. Objectives included 1) conducting active searches among sedentary and nomadic populations, 2) identifying ways to strengthen dracunculiasis surveillance, 3) evaluating general dracunculiasis knowledge, 4) sensitizing and educating persons about dracunculiasis, and 5) identifying at-risk localities in which to pre-position prevention and treatment supplies for the 2011 transmission season.
A cross-sectional survey among sedentary and nomadic populations was conducted. Seven districts were selected from among 16 districts in two overlapping categories: districts that were formerly endemic for dracunculiasis during 1994--2000 and districts that were not endemic during 1994--2000 but that had confirmed or suspected cases reported during 2010. Within selected districts, villages that were endemic for dracunculiasis during 1994--2000 or where rumored, suspected, or confirmed cases were reported during 2009--2011 were surveyed. Nomad camps were selected by convenience, based on recommendations from the Ministry of Livestock and Animal Resources and local veterinarians or nomad representatives in selected districts.
One KI in each selected village and nomad camp was interviewed using a questionnaire. In villages, the KI was a village chief or his representative; in nomad camps the KI was any adult representative available at the time of the visit. The KI was shown a photograph of an emerging Guinea worm and asked about awareness of or having ever seen dracunculiasis, recent rumors, and community water consumption practices. Village KIs also were asked about their knowledge of dracunculiasis transmission and prevention and about general indicators of health and development in their villages, whereas nomad KIs were asked about migration patterns and potential interactions with sedentary populations. In addition, assembled villagers were shown a photograph of an emerging worm and asked about awareness of or having ever seen dracunculiasis, including the village and year of the rumored case. Rumored cases occurring in 2007 or later were then investigated by interviewing the person reporting the rumor and by interviewing and examining the affected person, when possible. Each investigated rumor was then classified as a suspected case, a confirmed case, or as not dracunculiasis.
A total of 210 villages in seven districts were surveyed (Table); 138 (66%) had a safe water source, but residents of 116 (55%) villages consumed unsafe water (including residents in some villages with a safe water source). Among village KIs, 75% were aware of dracunculiasis, 55% knew how to prevent the disease, 59% knew how it is transmitted, 63% had seen someone with dracunculiasis, and 6% had seen someone with dracunculiasis during 2007--2011. Only 21% had heard about the monetary reward system for reporting a dracunculiasis case (Table). In 10 (5%) villages, at least one villager among those assembled reported that one or more rumored cases were seen during 2007--2011. Twenty rumored cases were reported in these 10 villages and subsequently were investigated. Of these 20 rumored cases, seven were found to have a history consistent with dracunculiasis and were classified as suspected cases.
Fifteen nomad camps in five districts were visited (Table). Eighty-seven percent of nomad KIs reported camp residents consumed unsafe water sometime during the year. These populations interact regularly with sedentary populations, either to share water sources or to attend weekly markets. No nomad KI had seen a case during 2007--2011 or knew about the monetary reward system.
Since the investigation, the first two 2011 cases were confirmed in Chad. The two cases increased the total number of at-risk villages to 36, including the two patients' villages of residence and three additional villages visited by one of the patients during the 10--14 months preceding worm emergence (7).
Reported by
Mathias R. Djidina, MD, Div of Communicable and Non-Communicable Disease Prevention; Hassan Guialoungou, Baba Brahim Dono, Neloumta Ngarhor, Miyara Padjaïna, Chad National Guinea Worm Eradication Program, Chad Ministry of Public Health. Gautam Biswas, MD, Dieudonné Sankara, MD, Alouseini Maiga, MD, Honoré Djimrassengar, MD, World Health Organization. WHO Collaborating Center for Research Training and Eradication of Dracunculiasis, Div of Parasitic Diseases and Malaria, Center for Global Health; Sharon L. Roy, MD, Div of Foodborne, Waterborne, and Environmental Diseases, National Center for Emerging and Zoonotic Infectious Diseases; Charbel El Bcheraoui, PhD, Jenny A. Walldorf, MD, EIS officers, CDC. Corresponding contributor: Jenny A. Walldorf, CDC, jwalldorf@cdc.gov, 404-639-8102.
Editorial Note
Occurring more than 10 years after the most recent case reported in the country, the dracunculiasis outbreak in Chad serves as a reminder that, until global eradication of dracunculiasis is achieved, adequate surveillance in areas where dracunculiasis was formerly endemic is essential. Following initial reports of two suspected dracunculiasis cases, three 2010--2011 investigations identified 31 at-risk villages§ based on the presence of confirmed or suspected cases. Subsequently, two additional cases have been confirmed, and the total number of at-risk villages has increased to 36. These villages represent areas of greatest risk for Guinea worm emergence and disease transmission in 2011. No outbreak point source was identified; no common epidemiologic factor apart from a history of drinking unsafe water linked all confirmed cases. Although 36 villages have now been targeted, the risk for continued transmission and further dracunculiasis spread is high throughout the investigation area. Many residents of villages and nomad camps in Chad consume unsafe water despite the presence of safe water sources in many villages. Villagers and nomads have limited knowledge about dracunculiasis prevention and transmission, and dracunculiasis surveillance is inadequate.
The resurgence of dracunculiasis transmission in Chad is a public health emergency of international concern and a setback for the global Guinea Worm Eradication Program. Urgent action is needed before and during the 2011 transmission season to contain the outbreak (Box). Ideally, active daily surveillance should be conducted in all villages within districts containing one or more at-risk villages; however, resources currently available in Chad are not likely to achieve this coverage immediately. Therefore, active surveillance and accompanying prevention measures should initially be focused on the 36 at-risk villages. As resources become available, these activities should be expanded to include all villages in districts with at-risk villages, all districts where dracunculiasis was endemic during 1994--2000, and all districts where confirmed or suspected cases occurring during 2009--2011 have been identified.
The seasonal migration of persons and livestock might have influenced transmission: 80% of confirmed 2010 cases and 86% of suspected cases identified during this investigation were located along the Chari River, which might have served as a conduit for infected persons. This river is a main transportation route across southern Chad, supports a fishing industry, and is crossed regularly by nomads who travel through Chad and sometimes to neighboring countries, interacting frequently with sedentary populations and sharing water sources. No conclusion could be made as to whether this outbreak resulted from cross-border importation or continued undetected domestic transmission during 2000--2010.
Because population movement across Africa will continue, the only measures against continued dracunculiasis transmission are sensitive ongoing surveillance, prompt investigation and case containment, and efficient communication. With <1,800 dracunculiasis cases reported worldwide in 2010(6), the global community must to support the four remaining countries (Ethiopia, Ghana, Mali, and Sudan) where dracunculiasis is endemic and all African countries where the disease was formerly endemic (including Chad). The renewed transmission of dracunculiasis in Chad illustrates a critical lesson for other global disease elimination programs regarding the importance of postintervention surveillance to ensure that disease transmission does not resume after programs have stopped.
Acknowledgments
Ministry of Public Health, Ministry of Agriculture, Ministry of Livestock and Animal Resources, Ministry of Environment and Water, Chad. Food and Agriculture Organization of the United Nations; United Nations Children's Fund (UNICEF), New York, New York. Ernesto Ruiz-Tiben, PhD, Donald R. Hopkins, MD, Carter Center, Atlanta, Georgia. Saidou P. Barry, MD, World Health Organization (WHO) Chad, Adiele Onyeze, MD, WHO African Region; Junerlyn Agua, Guinea Worm Eradication Team, WHO, Geneva, Switzerland. Mark L. Eberhard, PhD, Anthony Fiore, MD, Monica E. Parise, MD, Div of Parasitic Diseases and Malaria, Center for Global Health; Michael Wellman, Geospatial Research, Analysis, and Services Program, Agency for Toxic Substances and Disease Registry, CDC.
References
- World Health Organization. Dracunculiasis eradication: case definition, surveillance and performance indicators. Wkly Epidemiol Rec 2003;37:323--8.
- Imtiaz R, Hopkins DR, Ruiz-Tiben E. Permanent disability from dracunculiasis. Lancet 1990;336:630.
- Ruiz-Tiben E, Hopkins DR. Dracunculiasis. In: Guerrant RL, Walker DH, Weller PF, eds. Tropical infectious diseases: principles, pathogens, and practice. 2nd ed. New York, NY: Elsevier; 2006:1204--7.
- Ruiz-Tiben E, Hopkins DR. Dracunculiasis (Guinea worm disease) eradication. Adv Parasitol 2006;61:275--309.
- Bimi L, Freeman AR, Eberhard ML, Ruiz-Tiben E, Pieniazek NJ. Differentiating Dracunculus medinensis from D. insignis, by the sequence analysis of the 18S rRNA gene. Annals Trop Med Parasitol 2005;99:511--7.
- World Health Organization Collaborating Center for Research, Training and Eradication of Dracunculiasis. Guinea worm wrap-up no. 203. Atlanta, GA: US Department of Health and Human Services, CDC; 2011. Available at http://cartercenter.org/resources/pdfs/news/health_publications/guinea_worm/wrap-up/203.pdf. Accessed June 6, 2011.
- World Health Organization Collaborating Center for Research, Training and Eradication of Dracunculiasis. Guinea worm wrap-up no. 204. Atlanta, GA: US Department of Health and Human Services, CDC; 2011. Available at http://cartercenter.org/resources/pdfs/news/health_publications/guinea_worm/wrap-up/204.pdf. Accessed June 6, 2011.
* A dracunculiasis case is contained if all of the following conditions are met: 1) the patient is detected within 24 hours of worm emergence; 2) the patient has not entered any water source since worm emergence; 3) the village health worker has properly managed the case by cleaning and bandaging until the worm is fully removed and by giving health education to discourage the patient from contaminating any water source; and 4) the containment process, including verification of diagnosis, is validated by a supervisor within 7 days of worm emergence.
† Unsafe stagnant water sources included ponds, pools in drying riverbeds, and shallow, uncovered wells. Safe water sources were those protected from possible Guinea worm contamination, including flowing rivers, covered hand-dug wells, or borehole wells.
§ An at-risk village is any village 1) with at least one confirmed or suspected case during 2009--2011 or 2) to which any confirmed dracunculiasis patient traveled during the 10--14 months preceding worm emergence. Nomad groups meeting these criteria or camping in proximity to a village meeting these criteria are also at risk.
FIGURE. Villages (N = 31) with confirmed or suspected cases or villages otherwise at risk during dracunculiasis outbreak --- Chad, 2010--2011
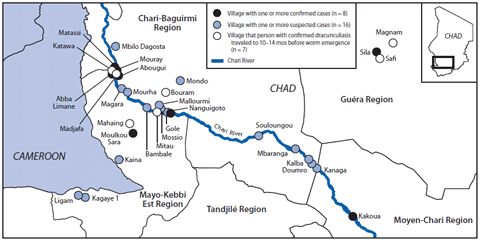
Alternate Text: The figure above shows villages with confirmed or suspected cases and villages at risk for dracunculiasis outbreak in Chad, during 2009–2011. The 10 confirmed cases were located in eight different villages in five districts, but six of the eight are along the Chari River.
What is already known on this topic?
Dracunculiasis (Guinea worm disease) is a waterborne, parasitic disease targeted for eradication. Transmission is prevented by filtering water from unsafe sources, preventing persons with emerging worms from entering drinking water sources, treating contaminated water with a larvicide, and providing safe drinking water sources in communities where dracunculiasis is endemic. Dracunculiasis transmission was thought to have been interrupted in Chad since 2000.
What is added by this report?
Ten new dracunculiasis cases were confirmed in Chad in 2010; because patients were not prevented from contaminating drinking water sources, new cases were expected in 2011. Surveys in 210 villages and 15 nomad camps identified 31 at-risk villages with confirmed or suspected cases during 2009--2011. Two additional cases were later confirmed in 2011, and the total number of at-risk villages was increased to 36.
What are the implications for public health practice?
The resurgence of dracunculiasis transmission in Chad is a public health emergency of international concern. At-risk villages require weekly active surveillance and urgent pre-positioning of materials before the April--October 2011 transmission season. Both sedentary and nomadic populations should be targeted for education, prevention, and surveillance activities.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.
