|
Key Points |
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Vital Signs: Nonsmokers' Exposure to Secondhand Smoke --- United States, 1999--2008
On September 7, this report was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr).
ABSTRACT
Background: Secondhand exposure to tobacco smoke causes heart disease and lung cancer in nonsmoking adults and sudden infant death syndrome, acute respiratory infections, middle ear disease, exacerbated asthma, respiratory symptoms, and decreased lung function in children.
Methods: National Health and Nutrition Examination Survey data from 1999--2008 were analyzed to determine the proportion of the nonsmoking population with serum cotinine (the primary nicotine metabolite) levels ≥0.05 ng/mL, by age, sex, race/ethnicity, household income level, and to determine whether the household included a person who smoked inside the home.
Results: During 2007--2008, approximately 88 million nonsmokers aged ≥3 years in the United States were exposed to secondhand smoke. The prevalence of serum cotinine levels ≥0.05 ng/mL in the nonsmoking population declined significantly from 52.5% (95% CI = 47.1%--57.9%) during 1999--2000 to 40.1% (95% CI = 35.0%--45.3%) during 2007--2008. The decline was significant for each sex, age, race/ethnicity, and income group studied except non-Hispanic whites. The change was greatest from 1999--2000 to 2001--2002. For every period throughout the study, prevalence was highest among males, non-Hispanic blacks, children (aged 3--11 years) and youths (aged 12--19 years), and those in households below the federal poverty level.
Conclusions: Secondhand smoke exposure has declined in the United States, but 88 million nonsmokers aged ≥3 years are still exposed, progress in reducing exposure has slowed, and disparities in exposure persist, with children being among the most exposed. Nearly all nonsmokers who live with someone who smokes inside their home are exposed to secondhand smoke.
Implications for public health practice: The only way to protect nonsmokers fully is to eliminate smoking in indoor spaces. Continued efforts at smoking cessation and comprehensive statewide laws prohibiting smoking in workplaces and public places are needed to ensure that all nonsmokers are protected from this serious health hazard. Health-care providers should educate patients and parents about the dangers of secondhand smoke and follow clinical care guidelines to help smokers quit.
Secondhand exposure to tobacco smoke causes heart disease and lung cancer in nonsmoking adults and sudden infant death syndrome, acute respiratory infections, middle ear disease, exacerbated asthma, respiratory symptoms, and decreased lung function in children (1). No risk-free level of secondhand smoke exposure exists (1). Levels of secondhand smoke exposure among U.S. nonsmokers have fallen substantially during the past 20 years (2). However, millions of nonsmokers remain exposed to secondhand smoke in homes, workplaces, public places, and vehicles (1). Using data from the National Health and Nutrition Examination Survey (NHANES) for 1999--2008, this report describes recent trends in secondhand smoke exposure among nonsmokers by analyzing levels of serum cotinine, a metabolite of nicotine that reflects recent exposure.
Methods
NHANES produces data for a nationally representative sample of the noninstitutionalized U.S. civilian population every 2 years. NHANES surveys include a home interview, physical examination at a mobile examination center where biologic specimens are collected, and laboratory specimen testing, including serum cotinine analysis for participants aged ≥3 years. Response rates exceeded 75% for all 2-year study cycles.* From the 1999--2000, 2001--2002, 2003--2004, 2005--2006, and 2007--2008 NHANES cycles, 30,451 respondents were determined to be nonsmokers (by cotinine level ≤10 ng/mL and self-reported history for persons aged ≥12 years) and were included in the analysis.
Serum cotinine was analyzed using an isotope dilution liquid chromatography tandem mass spectrometry method (2). Cotinine concentrations below a level known as the limit of detection (LOD) might be estimated inaccurately. The cotinine LOD initially was 0.05 ng/mL and changed to 0.015 ng/mL after improvements to the method. Cotinine levels below the LOD were reported as LOD / √2; this value represents the approximate midpoint of the interval between zero and LOD on a log scale.
Serum cotinine levels >10 ng/mL are associated with active smoking within the past few days (3). Therefore, children aged 3--11 years were assumed to be nonsmokers if their serum cotinine concentration was ≤10 ng/mL. Youths aged 12--19 years were considered nonsmokers if their serum cotinine concentration was ≤10 ng/mL and they did not report smoking within the preceding 30 days or use of any nicotine-containing product within the preceding 5 days at their physical examination. Adults aged ≥20 years were considered nonsmokers if their serum cotinine concentration was ≤10 ng/mL and they did not report being a current smoker during their home interview or report use of any nicotine-containing product within the preceding 5 days at their physical examination.
The percentage of the nonsmoking population with serum cotinine levels ≥0.05 ng/mL, the higher LOD, was calculated by survey cycle, sex, race/ethnicity group, age group, household income level, and whether households contained a person who smoked inside the home; 95% confidence intervals (CIs) were calculated using a log transformation for values >98% and the Wald method otherwise. Sample sizes are insufficient to allow separate reporting for race/ethnicity groups other than non-Hispanic whites, non-Hispanic blacks, and Mexican-Americans, but all race/ethnicity groups are included in the reported values for the total population and the values shown by sex, age group, and household income level. For 2007--2008, the most recently completed NHANES cycle, the number of nonsmokers with serum cotinine ≥0.05 ng/mL was calculated by age group using the midpoint population as the denominator, and the distribution of serum cotinine concentrations was examined separately for nonsmokers who lived with and without someone who smoked inside the home.
Two-sided t-tests were used to assess differences between population group percentages within study cycles and differences within population groups across study cycles; p<0.05 was considered statistically significant. Data analyses accounted for the complex survey design, differential probability of sample selection, nonresponse, and sample noncoverage.
Results
The overall prevalence of serum cotinine concentrations ≥0.05 ng/mL among the nonsmoking population fell from 52.5% (CI = 47.1%--57.9%) during 1999--2000 to 40.1% (CI = 35.0%--45.3%) during 2007--2008 (Table 1). However, the decline occurred only among the subset of the nonsmoking population that did not live with someone who smoked inside the home. The decline was significant for each sex, age, race/ethnicity, and income group studied except non-Hispanic whites. Prevalence fluctuated from cycle to cycle rather than showing a consistent decline; the greatest decline (10.8% percentage points) occurred from 1999--2000 to 2001--2002.
For every survey cycle, a significantly higher prevalence of cotinine concentrations ≥0.05 ng/mL was observed among males than among females, among non-Hispanic blacks than among non-Hispanic whites and Mexican-Americans, among children aged 3--11 years and youths aged 12--19 years than among adults aged ≥20 years, and among those below the federal poverty level than among those at or above the poverty level.
During 2007--2008, approximately 88 million nonsmokers aged ≥3 years in the United States were exposed to secondhand smoke (CI = 76 million--99 million) (Table 2). Of these, 32 million were aged 3--19 years, reflecting the higher prevalence of exposure among children and youths. Similarly, among nonsmoking adults, the prevalence of exposure decreased with age so that there were approximately 21--22 million exposed persons in each of the 20--39 year and 40--59 year age groups and approximately 14 million exposed persons in the ≥60 year age group.
Children and nonsmoking youths were more likely than nonsmoking adults to live with someone who smoked inside the home. During 2007--2008, 18.2% (CI = 11.2%--25.3%) of children aged 3--11 years and 17.1% (CI = 12.7%--21.4%) of youths aged 12--19 years lived with someone who smoked inside the home, compared with 5.4% (CI = 3.8%--7.0%) of adults aged ≥20 years. The majority (96.0%; CI = 93.3%--98.6%) of nonsmokers who lived with someone who smoked inside the home had cotinine levels ≥0.05 ng/mL (Figure). Among nonsmoking children and youths living with someone who smoked inside the home, 98.3% (CI = 95.5%--99.3%) had serum cotinine ≥0.05 ng/mL, compared with 39.9% (CI = 34.3%--45.4%) among those not living with someone who smoked inside the home (p<0.05). For nonsmoking adults, the corresponding prevalences were 93.4% (CI = 89.2%--97.5%) and 33.4% (CI = 29.1%--37.8%), respectively (p<0.05).
Conclusions and Comment
This is the first reported analysis of 2007--2008 cotinine levels among the full U.S. nonsmoking population aged ≥3 years. The results confirm that secondhand smoke exposure in the United States is far less prevalent at 40% than during 1988--1991, when 88% of the nonsmoking population age ≥4 years had serum cotinine levels ≥0.05 ng/mL (2). This decline is attributable to a number of factors, including decreased smoking prevalence, increases in the number of local and state laws prohibiting smoking in indoor workplaces and public places, increases in voluntary smoking restrictions in workplaces and homes, and changes in public attitudes regarding social acceptability of smoking near nonsmokers and children (1). Although prevalence of exposure has dropped for children and non-Hispanic blacks, groups that traditionally have had higher-than-average exposure levels (1--4), disparities remain. Further, this report shows that millions of nonsmokers in the United States remain exposed to secondhand smoke, including nearly all of those who live with someone who smokes inside the home.
Workplaces and homes usually are the most important sources of secondhand smoke exposure among adults because these are the settings where they typically spend the most time (1). The number of state, local, and voluntary smoke-free policies has greatly increased in recent years and has helped to protect nonsmokers from the toxicants in secondhand smoke. Nonetheless, currently only 24 states and the District of Columbia have comprehensive smoke-free laws covering workplaces, restaurants, and bars†; complete statewide bans are needed in the remaining 26 states because only 47% of the national population is covered by comprehensive state or local laws.§ Smoke-free policies have been shown to greatly reduce the probability and amount of exposure to secondhand smoke in workplaces and public places, as well as adverse health events.¶ Workplace smoking restrictions lead to smoking reductions and cessation among workers.** However, smoke-free policies do not eliminate secondhand smoke exposure from all sources. As workplaces and public places increasingly are made smoke-free, private settings such as homes and vehicles are becoming relatively larger sources of overall exposure (1).
The home is the major source of secondhand smoke exposure for children (1). During 1988--1994, fewer than 1% of children aged 4--16 years living with persons who smoked inside the home had cotinine levels <0.05 ng/mL (5). The findings in this report demonstrate that currently approximately 1.7% of nonsmoking children and youths (aged 3--19 years) living with someone who smoked inside the home had cotinine levels <0.05 ng/mL. Thus, among children living with persons who smoked inside the home, the likelihood of exposure has not changed appreciably during the past 20 years. The stall in the decline of adult smoking prevalence and the persistence of smoking in homes likely are impeding progress toward full protection of children and other nonsmokers from secondhand smoke exposure. Based on evidence that providing parents with information about the harms of secondhand smoke reduces children's exposure, the American Academy of Pediatrics and the U.S. Public Health Service recommend that clinicians ask parents about their smoking, advise them about the harms of secondhand smoke, and offer encouragement and help in quitting according to clinical care guidelines (6,7).
Previous studies have noted that non-Hispanic black nonsmokers tend to have higher cotinine levels than nonsmokers of other race/ethnicity groups (1,2). The reasons for this difference are not known, but some evidence suggests that slower metabolism or clearance of cotinine might result in blacks having higher cotinine levels for a given amount of exposure (8). Other possible reasons relate to levels of protection from exposure at home, in vehicles, and in public places or workplaces.
The findings in this report are subject to at least two limitations. First, nonsmoking status was defined based on self-report and cotinine levels. Self-reports might be inaccurate; similarly, any cotinine cutpoint might misclassify some persons. The optimal cotinine cutpoint might vary by race/ethnicity and age group, and is dependent upon background levels of secondhand smoke (1,8). This analysis used the 10 ng/mL cutpoint to be consistent with previous analyses (1--4). Using self-report and cotinine levels in combination should have minimized misclassification. Second, the sample size was insufficient to allow calculation of trends for all race/ethnicity groups. Smoking prevalence varies widely across and within race/ethnicity groups (9) and by region (10); secondhand smoke exposure rates are similarly variable (1). Also, variability in secondhand smoke exposure across population subgroups might have contributed to the observed fluctuation in prevalence during the study period because NHANES is not designed to have the same regional distribution in every cycle.
Healthy People 2010 objective 27-10 is to reduce the percentage of the nonsmoking population exposed to secondhand smoke (i.e., those with serum cotinine levels ≥0.05 ng/mL) to ≤56%.†† This target has been met, but disparities in exposure persist. Nonsmokers who live and work in places lacking smoke-free laws or policies continue to be exposed to secondhand smoke (1). The only way to protect nonsmokers fully is to eliminate smoking in indoor spaces (1).
Several federal government initiatives are currently addressing this issue. For example, in 2010, funds from the American Recovery and Reinvestment Act were made available to all 50 states, the District of Columbia, seven U.S. territories, and 21 communities to address tobacco control. As part of this Communities Putting Prevention to Work Initiative, grantees that do not already have comprehensive smoke-free policies covering workplaces and public places are working toward adopting such policies. The U.S. Department of Housing and Urban Development issued a notice§§ encouraging public housing authorities to implement no-smoking policies in 2009. The U.S. Environmental Protection Agency conducts a national campaign that educates and encourages parents to make their homes smoke-free to protect their children's health.¶¶ Continued efforts to reduce secondhand smoke exposure in all settings are needed to ensure that all nonsmokers are protected from this hazard.
Reported by
RB Kaufmann, PhD, S Babb, MPH, A O'Halloran, MSPH, K Asman, MSPH, E Bishop, MS, M Tynan, RS Caraballo, PhD, TF Pechacek, PhD, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion; JT Bernert, PhD, B Blount, PhD, Div of Laboratory Sciences, National Center for Environmental Health, CDC.
Acknowledgments
This report is based, in part, on contributions by M Eischen, D Homa, PhD, A MacNeil, MPH, G Promoff, MA, D Shelton, MPH, A Trosclair, MS, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC.
References
- US Department of Health and Human Services. The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, CDC; 2006. Available at http://www.surgeongeneral.gov/library/secondhandsmoke/report/fullreport.pdf.
- Pirkle JL, Bernert JT, Caudill SP, Sosnoff CS, Pechacek TF. Trends in the exposure of nonsmokers in the U.S. population to secondhand smoke: 1988--2002. Environ Health Perspect 2006;114:853--8.
- CDC. Fourth national report on human exposure to environmental chemicals. Atlanta, GA: US Department of Health and Human Services, CDC; 2009. Available at http://www.cdc.gov/exposurereport.
- Max W, Sung H-Y, Shi Y. Who is exposed to secondhand smoke? Self-reported and serum cotinine measured exposure in the U.S., 1999--2006.
- Mannino DM, Caraballo R, Benowitz N, Repace J. Predictors of cotinine levels in US children: data from the Third National Health and Nutrition Examination Survey. Chest 2001;120:718--24.
- Fiore MC, Jaen CR, Baker TB, et al. Clinical practice guideline. Treating tobacco use and dependence: 2008 update. Rockville, MD: US Department of Health and Human Services, Public Health Service; 2008. Available at http://www.surgeongeneral.gov/tobacco/treating_tobacco_use08.pdf.
- Committee on Environmental Health, Committee on Substance Abuse, Committee on Adolescence, Committee on Native American Child Health. Tobacco use: a pediatric disease. Pediatrics 2009;124:1474--84.
- Benowitz NL, Bernert JT, Caraballo RS, Holiday DB, Wang J. Optimal serum cotinine levels for distinguishing cigarette smokers and nonsmokers within different racial/ethnic groups in the United States between 1999 and 2004. Am J Epidmiol 2009;169:236--48.
- Caraballo RS, Yee SL, Gfroerer J, Mizra SA. Adult tobacco use among racial and ethnic groups living in the United States, 2002--2005. Prev Chronic Dis 2008;5:1--9.
- CDC. Vital Signs: current cigarette smoking among adults aged ≥18 years---United States, 2009. MMWR 2010;59(35).
* Additional information available at http://www.cdc.gov/nchs/nhanes/response_rates_cps.htm.
† Additional information available at http://apps.nccd.cdc.gov/statesystem.
§ Additional information available at http://www.no-smoke.org/pdf/SummaryUSPopList.pdf.
¶ Additional information available at http://www.iom.edu/reports/2009/secondhand-smoke-exposure-and-cardiovascular-effects-making-sense-of-the-evidence.aspx.
** Additional information available at http://www.iarc.fr/en/publications/pdfs-online/prev/handbook13/handbook13.pdf.
†† Additional information available at http://wonder.cdc.gov/data2010.
§§ Available at http://www.hud.gov/offices/pih/publications/notices/09/pih2009-21.pdf.
¶¶ Additional information available at http://www.epa.gov/smokefree.
FIGURE. Serum cotinine levels among nonsmoking persons aged ≥3 years --- National Health and Nutrition Examination Survey, United States, 2007--2008
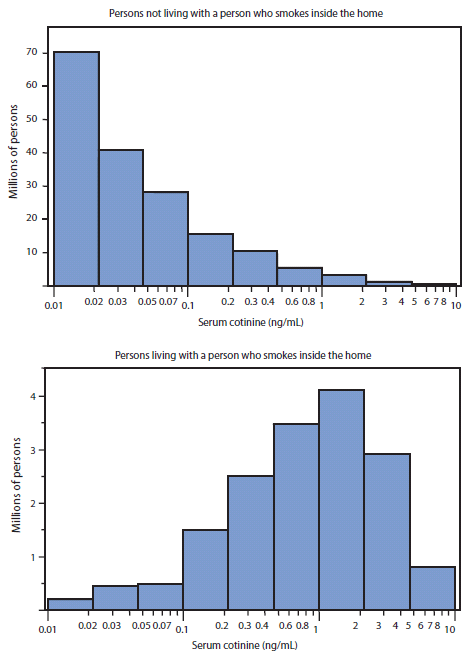
Alternate Text: The figure above shows serum cotinine levels among nonsmoking persons aged ≥3 years in the United States during 2007-2008, based on data from the National Health and Nutrition Examination Survey.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
