Key points
- Giardia is a tiny parasite (germ) that causes diarrhea.
- Giardia can spread easily from one person to another or through water, food, surfaces, or objects.
- A healthcare provider can prescribe medicine to treat illness caused by Giardia.
What it is
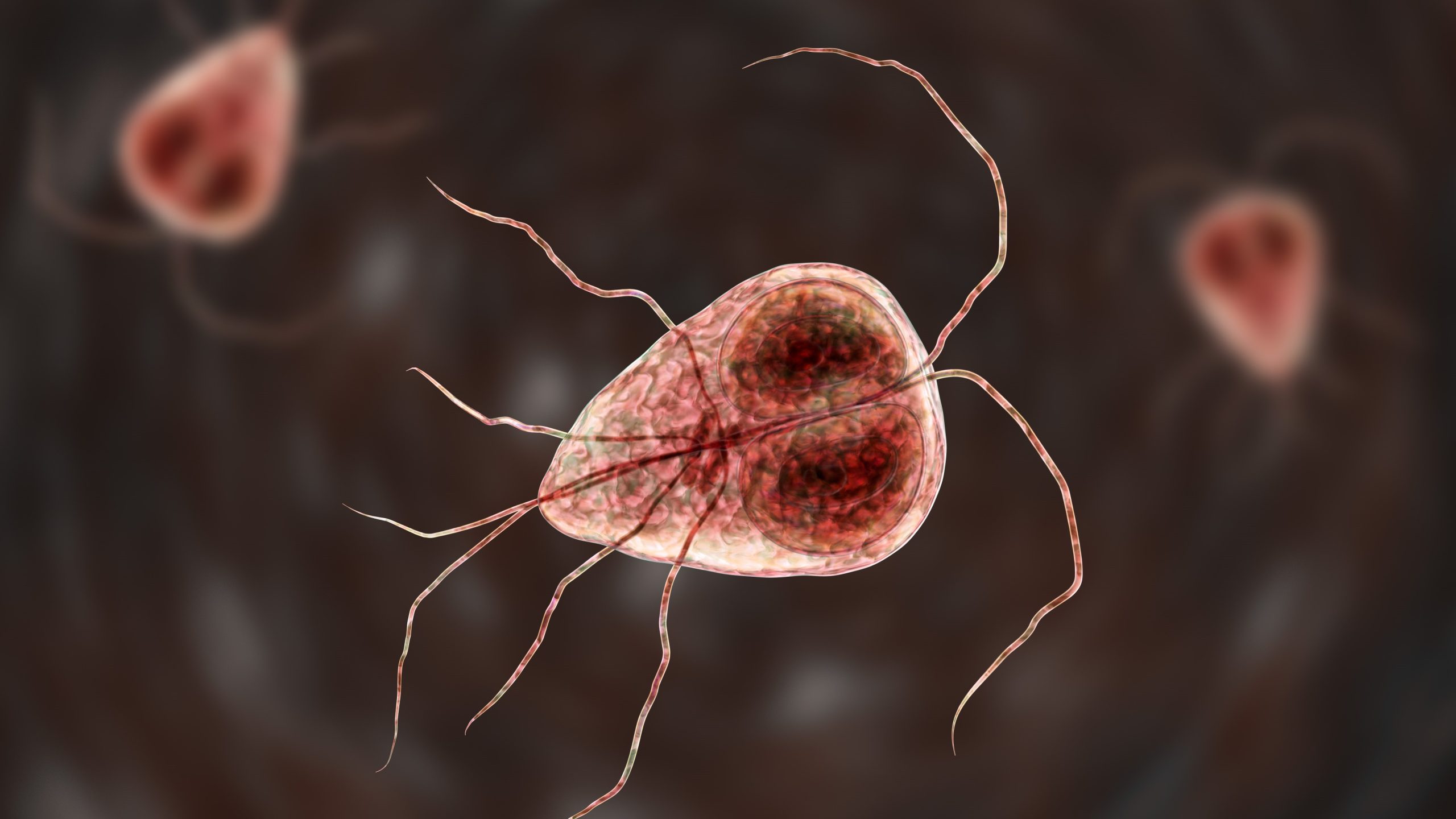
Giardia duodenalis (Giardia for short) is a parasite. Illness caused by Giardia is called giardiasis.
Giardia lives in the gut of infected people and animals and comes out of the body in poop. Giardia can survive for weeks to months outside the body (for example, in soil).
Giardia is found in every region of the United States and around the world.
Giardia in the United States
Symptoms
Symptoms usually begin by having diarrhea 2 to 5 times per day and feeling more and more tired.
Short-term symptoms include:
- Diarrhea
- Gas
- Smelly, greasy poop that can float
- Stomach cramps or pain
- Upset stomach or nausea
- Dehydration (loss of fluids)
Symptoms usually begin 1 to 2 weeks after becoming infected with Giardia and last for 2 to 6 weeks. Occasionally, people have long-term symptoms that can last for years.
Who is at risk
Anyone can get sick from Giardia. However, children are more likely to get sick than adults.
You are more likely to get sick if you:
- Are in close contact with someone who is sick from Giardia, especially in childcare settings
- Are in an area with limited access to safe drinking water
- Drink untreated water from springs, lakes, rivers, or shallow wells
- Swallow water from pools, splash pads, lakes, or rivers (for example, while swimming)
- Have a weakened immune system
- Have contact with poop during sex
- Have contact with infected animals or animal environments contaminated with poop
How it spreads
You can get sick if you swallow Giardia.
Giardia germs are in poop, so anything that gets contaminated by poop can potentially spread the germs. Giardia can spread from one person to another or through contaminated water, food, surfaces, or objects.
Giardia spreads easily; swallowing just a few Giardia germs can make you sick.
Prevention
You can take steps to avoid getting or spreading Giardia:
- Wash your hands with soap and water at key times.
- Avoid swallowing water while swimming.
- Boil or filter water from lakes, springs, or rivers before drinking or preparing food with it.
- Wait to have sex for several weeks after you or your partner no longer have diarrhea.
- Avoid touching animal poop.
- Clean and disinfect areas where a person or pet recently had diarrhea.

Diagnosis
Contact a healthcare provider if you think you may be sick from Giardia. They will ask you to give stool (poop) samples to see if Giardia is making you sick.
Treatment and recovery
Your healthcare provider may prescribe medicine to treat illness caused by Giardia.
If you have diarrhea, drink a lot of water or other fluids to avoid dehydration (loss of fluids).
Animal transmission
Although animals can spread Giardia to people, you are unlikely to get a Giardia infection from dogs or cats. The type of Giardia that makes people sick is usually not the same type that makes dogs and cats sick.