NSSP Update – July 2019

- Community of Practice
- Workgroup and Committee Updates
- NSSP Community of Practice Call
- Implementation Guide for Syndromic Surveillance
- CDC Funding Recipients and Partnerships
- Arizona Monitors Transfer of Patients with Suspected RMSF
- Data-sharing Workshops Strengthen Public Health Jurisdictions
- ESSENCE Queries

- Free-text Coding in NSSP– ESSENCE
- Data Quality Corner
- Questions and Tips
- Spotlight Article: Harnessing Data Science to Improve Population Health and Public Health Surveillance

People
Community of Practice
Workgroup and Committee Updates
-
Data Quality Committee (DQC): Volunteers needed! The DQC is looking for one or two volunteers to help determine the contents for electronic health record (EHR) vendor and product drop-down lists for the Master Facility Tool (MFT). The MFT contains all necessary information for processing data. MFT fields ensure data are mapped correctly on the journey from facility to BioSense Platform and are easily identifiable when data are queried. Interested? Please e-mail Elyse at elyse.kadokura@doh.wa.gov or MisChele at MisChele.Vickers@adph.state.al.us.
-
Overdose Surveillance Committee (ODSC): At the 2019 Council of State and Territorial Epidemiologists (CSTE) Annual Conference, the NSSP Community of Practice (CoP) ODSC held a roundtable discussion at the conclusion of the Substance Use and Mental Health pre-conference workshop “Flying High Taking Substance Use and Mental Health Surveillance to the Next Level.” During this roundtable, we discussed some of the different surveillance systems used for overdose and the key components in responding to outbreaks.Most participants who work with syndromic surveillance either use the national NSSP–ESSENCE (BioSense Platform) or use local variants and typically defined alerts somewhat like those statistical alerts within ESSENCE. Some participants discussed the timeliness of data and difficulties in gaining access to rapid data (specifically, police seizure and drug testing data). In addition to our roundtable focus on data, a major discussion topic that emerged was the importance of having communication plans in place when outbreaks occur. Specifically, the plan should describe who needs to be part of the response (e.g., Public Health, Public Safety, local hospitals); what does the plan look like; and when the plan should be activated. From the overall perspective of the roundtable participants, there is a (1) significant need to identify and access rapid data for overdose coupled with (2) multi-leveled response plans, depending on the severity and issue scope.Also, the ODSC co-chairs participated in other conference roundtable discussions, such as injury prevention and occupational health, to build connections with community partners and make them aware of ODSC activities and the expertise and perspective we can provide.

NSSP Community of Practice Call
Please join the monthly NSSP CoP call. This call is powered by community members who share guidance, resources, and technical assistance. The call includes a forum for discussion and questions. The next call will be held on (note date change) July 30, 2019, 3:00–4:30 PM ET. The discussion topic is Preparing for Disaster Surveillance.
New member? Syndrome? Success? Email NSSP!
There’s no need to wait until Fall 2019 when a new cooperative agreement is in place to get involved in the NSSP Community of Practice (CoP). If you’re interested in participating, please email nssp@cdc.gov and give your name, contact information, and request to be part of the NSSP CoP. If you want to be part of a specific committee or workgroup, we will forward your email to that group’s chair and co-chair.
If you have a syndrome to share, success story to showcase, or resources to post on the Knowledge Repository, email nssp@cdc.gov. We will forward your request to the appropriate NSSP CoP committee or workgroup to review before posting.
Look to the Portal for Community of Practice Updates

We want to thank everyone who updated their profile and gave permission for their CoP membership to be transferred to CDC. Your continued interest in the NSSP CoP and, importantly, your support of the work it does to strengthen syndromic surveillance through the Steering Committee, workgroups, and committees is greatly appreciated.
If you’re wondering how to access NSSP CoP trainings, videos, and webinars, here’s where to find resources:
- NSSP CoP Syndromic Surveillance Portal (https://www.syndromicsurveillance.org/index.html): From the portal, you can go to one site and get updates on the transition and quickly access state website content on syndromic surveillance. You can sign-on to the BioSense Platform; access the Knowledge Repository and NSSP Resource Center; see calendar entries for workgroup, committee, and monthly NSSP CoP meetings; and check out the latest issue of NSSP Update.
- Knowledge Repository (KR): The URL for the KR has not changed, so if you’ve bookmarked the location, you’re all set. Still, we encourage you to go to the NSSP CoP Syndromic Surveillance Portal because it is a one-stop shop for transition updates. The KR still offers broad access to resources, though menu selections to access community groups or upload successes and syndromes are not available.
- Monthly NSSP CoP Call: During the NSSP CoP transition from one cooperative agreement to another, the call-in information will be emailed to CoP members. Topics will be added to the Portal calendar.
Again, thanks for your support of the NSSP CoP. Syndromic surveillance is an essential part of CDC’s Strategic Surveillance Strategy, and NSSP will continue to support the NSSP CoP throughout the transition and beyond.
Implementation Guide for Syndromic Surveillance
| HL7 2.5.1 Implementation Guide Milestones* | |
|---|---|
| Time Frame | Activity |
| 2015 | Completed Version 2.0 Final RELEASE** |
| 2016 | Released Erratum and Clarification Documents for Version 2.0 |
| 2017 Summer | Released Version 2.2 Working Draft for Community Comment and Consensus |
| 2017 Winter | Released Version 2.3 for Review and Community Comment |
| 2018 March | Released Version .09 |
| 2018 Spring | Submitted DRAFT HL7 Guide for Balloting: Implementation Guide for Syndromic Surveillance Release 1.0 Standard for Trial Use (STU) HL7 Version 2.5.1 |
| 2018 Fall (October–December) |
|
| 2018 November– 2019 March |
|
| 2019 January | Provided Final Resolution for 33 Comments (Pending) |
| 2019 February |
|
| 2019 March–May |
|
| 2019 June 20–27 | Hand-off to HL7 Public Health Workgroup for 2-week review |
| 2019 July |
|
| 2019 Summer (June–August) |
|
| 2019 September | Release to Public: HL7 2.5.1 Implementation Guide for Syndromic Surveillance for Trial Use Version 1 (STU) |
| 2019 September–November |
|
| 2019 September–2022 September | Publish Standard for Trial Use (STU) for Trial Period of 1 to 3 years (during which time additional comments may be submitted and dispositioned and additional releases of the guide published) |
* Milestones revised June 20, 2019.
** Version 2.0 is currently being used; subsequent versions are working drafts only.
Shaded activities have been completed.
Implementation Guide Available to Validate Messages
The Implementation Guide is now available for HL7 message validation via the National Institute of Standards and Technology Implementation Guide Authoring Tool (NIST IGAMT). Anyone can validate a message as a guest user for this specification. Once you’re on the website, go to Tool Scopes in the upper right-hand corner and select “Syndromic Surveillance.”

CDC Funding Recipients and Partnership Updates
Arizona’s success in identifying a potential case of Rocky Mountain Spotted Fever was presented at the 2019 CSTE Conference. People over the age of 40 years account for the highest number of reported cases, however, children under 10 years old represent the highest number of reported deaths.1
Arizona Monitors Transfer of Patients with Suspected RMSF
Rocky Mountain Spotted Fever (RMSF) is a bacterial disease spread through the bite of an infected tick. Most people who get sick with RMSF will have a fever, headache, and rash. RMSF can be deadly if not treated early with the right antibiotic.2

In Arizona, people with suspected RMSF are often transported from tribal lands to Maricopa County hospitals. RMSF is not locally acquired in Maricopa County, and physicians do not always suspect RMSF as the cause of an illness. Although an RMSF transfer protocol had been in place since 2012, sometimes people with suspected RMSF can spend days in Maricopa County facilities and often are discharged before the Maricopa County Department of Public Health (MCDPH) is notified. Also, sometimes RMSF acquired on Arizona tribal land does not present with a rash, unlike what is observed in other parts of the United States, which can lead to misdiagnosis. Doxycycline,3 the recommended first-line antibiotic, is usually given before transport. Due to misperceptions about doxycycline staining teeth among children younger than 8 years of age, these children run the risk of lifesaving treatment being interrupted.
Analysts at the MCDPH used NSSP–ESSENCE to create a myESSENCE dashboard and an RMSF query. They designed the query to capture patients with a residential tribal ZIP code being treated at a Maricopa County facility that followed the RMSF transfer protocol. The query had RMSF-related terms in the chief complaint or reason for admission. On June 8, 2018, the NSSP–ESSENCE syndromic surveillance system flagged a suspected case of RMSF—an infant transferred to a Maricopa County hospital two days earlier.
Read the story (posted in the Knowledge Repository) to see the terms they searched on and learn how cases are flagged and categorized. This is a good example of syndromic surveillance providing timely information that informs public health response.
Data-sharing Workshops Strengthen Public Health Jurisdictions
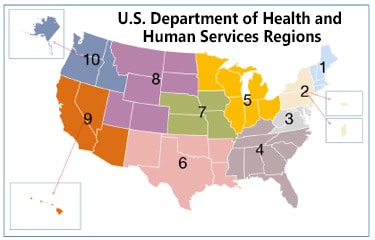
NSSP in partnership with the Council of State and Territorial Epidemiologists (CSTE) is conducting four regional data-sharing workshops and one capstone course to strengthen the capacity of public health agencies that conduct syndromic surveillance (SyS) and collaborate across jurisdictions. The workshops will enhance situational awareness using real-time electronic health data from emergency departments through interjurisdictional data sharing and surveillance practice collaborations.
The workshop design takes into account the shared interests and priorities of professionals in each of the U.S. Department of Health and Human Services’ (HHS) ten regions. Workshops are customized to meet the participants’ objectives, maximizing the workshop’s practical value and setting the foundation for subsequent collaborative work with colleagues nationwide.
At the end of the workshop, participants will be better prepared to support agency activities for opioid crisis response. They will have examined and shared best practices in SyS analytic methods and NSSP tool use, developed action steps for interjurisdictional data sharing, and fostered collaboration among their peer network of surveillance professionals.
Workshop Schedule
- South and East (HHS Regions 3, 4, and 6); April 30–May 1, 2019; Atlanta, GA
- Northeastern (HHS Regions 1, 2, and DE and PA); June 11–12, 2019; Boston, MA
- West (HHS Regions 8, 9, 10, and NM); July 23–24, 2019; Phoenix, AZ
- Midwest (Regions 5 and 7); August 6–7, 2019; Chicago, IL
Capstone Meeting
On August 21, 2019, NSSP will host a capstone meeting in Atlanta, Georgia, to summarize what was accomplished throughout the four regional workshops and to identify an action plan for moving forward. Follow-up documentation will be provided on best and promising practices for using SyS, benefits and barriers to data sharing, solutions to high-priority barriers, and improvements to analytic methods.
These workshops are sponsored by the Centers for Disease Control and Prevention (CDC) through a cooperative agreement (1 NU380T000297-01-00) with the Council of State and Territorial Epidemiologists.
ESSENCE QUERIES

Query Terms from May 2019
A key feature of NSSP–ESSENCE is its ability to use free-text definitions across different fields to generate custom queries. The SyS community can use this feature to develop and refine category definitions and to identify and respond to public health events that may not be apparent in established categorical definitions (i.e., syndromes, subsyndromes, and Chief Complaint and Discharge Diagnosis [CCDD] categories).
This word cloud summarizes free-text and coded values that epidemiologists and data analysts queried in ESSENCE during May 2019. This word cloud was generated using the Wordcloud2 package in RStudio. The relative size of the terms suggest the frequency of use in a query. NSSP super administrators can query ESSENCE usage logs to learn what queries are run nationwide and how long they take to complete.
Do you enjoy seeing national-level data depicted in a word cloud? Let us know!
Practice
Free-text Coding in NSSP–ESSENCE
This is the third in a series of articles about how to write ESSENCE free-text queries.
“Part 1. Wildcards” can be found here.
Introduction

The search criteria for ESSENCE free-text queries are built around Boolean logical operators and regular expressions. Free-text queries are not case-sensitive and may contain “^” for wildcards; “,” for multiple entries; “ISBLANK” to look for blanks; “ISNULL” to look for nulls; [COMMA] to look for commas; and operators “and,” “or,”, “andnot,” and parentheses “()” to define order and grouping. This series will cover all these topics in-depth.
Free-text queries are what makes syndromic surveillance practice, particularly practice using NSSP–ESSENCE, adaptable to different data sources and types. By using free-text queries, analysts and epidemiologists can exercise a high level of customization. They can quickly code free-text queries and rapidly respond to outbreaks, disasters, and events that unfold. Such capabilities empower users to customize queries to fit their level of data, ensuring accurate results.
Free-text coding in ESSENCE, which is accessible to all users, follows distinct patterns. Learning to read these patterns allows users to take queries from many places and repurpose them to suit their unique needs. Syndromic surveillance depends heavily on sharing methods, and practitioners must understand the language.
Part 3. Inclusionary Terms
Now that this series has covered basic query notation and use of Carets, Underscores, and Brackets, the next step is to string together query criteria in a series. Even though a syndrome definition could technically be a single term, the use of multiple terms allows for diversity in capturing different contents from a field like Chief Complaint (CC) text or forms of Discharge Diagnosis (DD) codes. This part covers the basic “OR” and “AND” statements linking multiple terms and recommends basic tips for using these statements.
“OR” statements
“OR” statements are the most basic way to use multiple query terms in ESSENCE. Many queries and data explorations start with a basic search for “SYMPTOM #1” OR “SYMPTOM #2.” In ESSENCE, an “OR” statement is automatically applied to terms separated by a comma, but a best practice is to include all operators to improve troubleshooting and readability when sharing syndrome definitions. ESSENCE queries are not case sensitive, and neither are the operators. Some ESSENCE users prefer to capitalize all operators to make them stand out, whereas other users prefer to leave operators lowercase. It’s all personal preference. However, operators should always be surrounded by commas, and the correct format of a query for THIS, THAT, or THERE follows:
THIS,OR,THAT,OR,THERE
Note the commas around each instance an operator is used.
Let’s assume the following Chief Complaints (used in Parts 1 and 2) and a desire to create a query for fall-related injuries.
- Fall
- Fell getting out of car
- Left arm injury; Fall
- Falling out with friends; Suicidal
- Feels crestfallen
- Patient brought in after falling on face
- Fall; Left wrist injury
- Feels congested; Allergies
You may reasonably assume the boldfaced CCs 1, 2, 3, 6, and 7 are the intended cases and 4, 5, and 8 are false positives.
Here’s a table that shows examples of the “OR” query:
| “OR” Query Examples | |
|---|---|
| Code | Description |
^Fall^ |
This is a simple query of a term surrounded by carets taken from Part 1. It returns CCs 1, 3, 4, 5, 6, and 7. |
| Fall,OR,Fell getting out of car,OR,Left arm injury; Fall,OR,Patient brought in after falling on face,OR,Fall;Left wrist injury | This extremely long query lists the CCs exactly as they appear and accomplishes our goal to include CCs 1, 2, 3, 6, and 7 while excluding CCs 4, 5, and 8. Although it works for this very small sample of CCs, it almost certainly will not work well on the broad range of real syndromic data. It’s also long and hard to read. |
^Fall^,OR,^Fell^ |
This covers both forms of “Fall” in our CCs. Returns CCs 1, 2, 3, 4, 5, 6, and 7. |
^ Fall^,OR,Fall ^,OR,Fall,OR,^Fell^ |
The first term removes the false positive “Crestfallen,” and the second term captures visits where the term starts the CC. The third term returns the stand-alone fall term, and the fourth term returns all visits containing “Fell.” Returns CCs 1, 2, 3, 6, and 7. |
Sometimes an analyst or epidemiologist will want to code a text string to appear by itself and not in the middle of another word. The code may be a series of terms associated with “OR” statements. For example, the code ^ Fall ^ surrounds the term in spaces, ensuring the term doesn’t appear in the middle of a text string like “crestfallen.” This query would miss any visit where the queried variable has the text string “Fall” at the start or end of the field because, in these instances, it wouldn’t be preceded and followed by a space. To capture these other forms, try including the code in four ways:
^ Fall ^,OR,Fall,OR,^ Fall,OR,Fall ^
In this query, ^ Fall ^ specifies it can’t appear in the middle of a word, and ,Fall,OR,^ Fall,OR,Fall ^ specifies any time the term appears by itself as the only field text at the end of a field and at the beginning of a field, respectively
Speaking of multiple forms, part 2 of this series touched on ways to include different forms of ICD9 and ICD10 codes. If your query term for an ICD9 or ICD10 code goes beyond the decimal place, a best practice is to include the decimal and non-decimal form of the code separated by an “OR” statement. Some facilities omit the decimal from the ICD code, which can change how your query performs. By including both forms, you ensure the query picks up as many relevant visits as possible. An example is the use of ICD9 code E888.9 and ICD10 code W19.XXXA, both concerning an unspecified fall:
^E888.9^,OR,^E8889^
^W19.XXXA^,OR,^W19XXXA^
“AND” statements
“AND” statements are another way to use multiple query terms to craft a syndrome definition in NSSP–ESSENCE. Unlike “OR” statements that specify at least one criteria be met, terms linked by an “AND” statement look for visits that meet more than one criteria. “AND” statements do not specify the order the terms appear or location within the field queried. “AND” operators follow the same format as “OR” statements and must be surrounded by commas. The correct query format for THIS, and THAT, and THERE follows: THIS,AND,THAT,AND,THERE
Let’s assume the following Chief Complaints, used in Parts 1 and 2, and a desire to create a query for fall-related injuries.
- Fall
- Fell getting out of car
- Left arm injury; Fall
- Falling out with friends; Suicidal
- Feels crestfallen
- Patient brought in after falling on face
- Fall; Left wrist injury
- Feels congested; Allergies
You may reasonably assume the boldfaced CCs 1, 2, 3, 6, and 7 are the intended cases and 4, 5, and 8 are false positives.
| “AND” Query Examples | |
|---|---|
| Code | Description |
^Fall^,AND,^Injur^ |
This “AND” statement requires the term Fall appear alongside the term Injur. Returns CCs 3, and 7. |
^Fall^,AND,^Face^ |
This query requires the face be mentioned alongside the term fall. Returns CC 6 ONLY. |
^Fall^,AND,^Fall^ |
Be careful of duplicative “AND” statements. This does not guarantee the text appears twice in the query. Each can be thought of as a separate search of the query and the return is the overlap. Returns CCs 1, 3, 4, 5, 6, and 7. |
^Fall^,AND,(,^Injur^,OR,^Face^,) |
This is a simple combination of “AND” and “OR” statements grouped by parentheses. Parentheses will be covered later in the series, but like the rules of math, the “AND” statement means the term “fall” must appear alongside at least one term from within the parenthetical statement. Returns CCs 3, 6, and 7. |
Here are several examples that show how “AND” and “OR” statements can be used in practice:
-
This example is from the CDC Heroin Overdose v4 CCDD Category. Like the fall-related ICD example shown previously, notice how this excerpt uses “OR” statements to code multiple DD forms and also includes both decimal and non-decimal terms.…..^[;/ ]T40.1X1A^,OR,^[;/ ]T401X1A^,OR,^[;/ ]T40.1X4A^,OR,^[;/ ]T401X4A^,OR,^[;/ ]965.01[;/]^,OR,^[;/ ]96501[;/]^,OR,^[;/ ]E850.0^,OR,^[;/ ]E8500^,or,…..
-
The next example is from the CDC Legionella v1 CCDD Category. Notice how different spellings of Legionella/Legionnaire’s Disease are included with “OR” statements to ensure relevant visits are captured.^LEGIONNAI^,or,^LEGIONE^,or,^LEGIONA^,or,^PONTIAC^FEVER^,…..
-
These next two examples are taken from the CDC Firearm injury V1 and Norovirus v1 CCDD Categories, respectively. Both include parenthetical statements but can be expanded into (much less compact) equivalent codes.(,^hit^,or,^ricochet^,or,^graze^,),and,(,^bullet^,) is equivalent to ^hit^,AND,^bullet^,OR,^ricochet^,AND,^bullet^,OR,^graze^,AND,^bullet^(,^stomach^,and,(,^bug^,or,^virus^,or,^ flu ^,)) is equivalent to ^stomach^,AND,^bug^,OR,^stomach^,AND,^virus^,OR,^stomach^,AND,^ flu^
NSSP–ESSENCE also applies “AND” and “OR” statements across different fields.
After typing or pasting your code into a free-text field, you may apply the “OR” statements by selecting fields from the box titled “Also apply the search string to” …
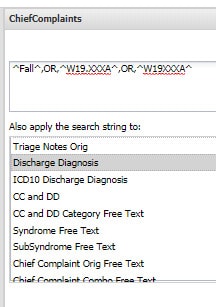
…and hitting select. “OR” statements applied correctly in the Selected Query Fields will look like this:
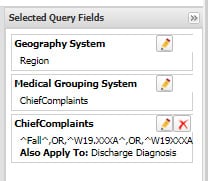
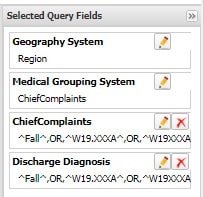
“AND” statements between fields in NSSP–ESSENCE will look like this with separate criteria selected for each field:
Try it out!
Compare the results of the following queries in the CCDD field of ESSENCE:
^Fall^,OR,^W19.XXXA^,OR,^W19XXXA^
^Fall^,AND,^W19.XXXA^,OR,^Fall^,AND,^W19XXXA^
Try selecting other “Also apply the search string to:” options and then try pasting the query into more than one field to see how this alters results.
We thank Senior Data Analyst Zachary Stein for volunteering to write a series of articles about free-text coding. Stein, formerly with the Kansas Department of Environment and Health, does epidemiologic work to support NSSP efforts. Stein is an active participant in the NSSP CoP. He initially wrote about free-text coding as an entry on the NSSP CoP Syndrome Definition Committee forum. The forum generated considerable interest, inspiring this series. Stein acknowledges input provided by others who contributed to the forum post.
Data Quality Corner
ESSENCE Data Quality Filter
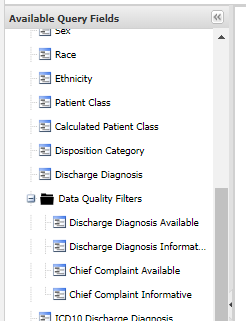
A recent update to ESSENCE introduced a Data Quality Filter. This new feature can help you track and enhance data quality for Chief Complaint and Discharge Diagnosis. Given the importance of these elements to syndromic surveillance, this feature should prove useful during internal data quality checks and associated analyses. The Data Quality Filters are listed below:
- Chief Complaint Available
- Chief Complaint Informative
- Discharge Diagnosis Available
- Discharge Diagnosis Informative
To access the Data Quality Filter tab in ESSENCE, go to the Query Portal and scroll down within the Available Query Fields as shown:
There are two indicators to understand:
- Chief Complaint Available: This indicator measures completeness of the chiefcomplaintparsed (the CC of the CCDD) element at the visit level. Visits with a complete chief complaint are set to 1 (Yes) and counted as “available” within the ESSENCE “Chief Complaint Available” field. (Note. This metric simply measures the presence of a value in this segment, nothing further.)
- Chief Complaint Informative: Through collective input from the community working with the NSSP team, a systematic list of uninformative/not useful chief complaint terms was created. The acronym coined to describe terms with no relevance to syndromic surveillance is “NICC,” which stands for non-informative chief complaint (see the June issue for details). When any NICC occurs in chiefcomplaintparsed (the CC of the CCDD), the Chief Complaint Available will be marked as complete. But keep in mind, NICCs are not meaningful for the purposes of syndromic surveillance.
| NICC* Terminology | |||||||
|---|---|---|---|---|---|---|---|
| NICC ID | NICC Term | NICC ID | NICC Term | NICC ID | NICC Term | NICC ID | NICC Term |
| 1 | “” | 12 | other | 23 | Ambulance | 34 | Sick |
| 2 | null | 13 | xxx | 24 | EMS/Arrive by | 35 | Evaluation |
| 3 | unknown | 14 | Evaluation | 25 | EMS/Ambulance | 36 | Injury |
| 4 | unknown | 15 | Follow up | 26 | ; | 37 | ill |
| 5 | n/a | 16 | medical | 27 | ;; | 38 | Eval |
| 6 | na | 17 | illness | 28 | Triage | 39 | squad |
| 7 | Chief complaint not present | 18 | General | 29 | Triage peds | 40 | referral |
| 8 | ed visit | 19 | General Symptom | 30 | Triage- | 41 | Code 1 |
| 9 | ed visit | 20 | EMS | 31 | Triage peds- | 42 | Code 3 |
| 10 | er | 21 | AMR | 32 | See chief complaint quote | ||
| 11 | Advice only | 22 | medical | 33 | See CC quote | ||
*Non-informative Chief Complaint (NICC)
When the Chief Complaint is solely populated with any of these terms (NICCs), ESSENCE processing will flag that Chief Complaint as uninformative and set it to 0 (No) in the ESSENCE “Chief Complaint Informative” field going forward. This allows you to perform selective analysis on visits with informative/meaningful chief complaint.
- Discharge Diagnosis Available: This indicator measures completeness of the discharge_diagnosis (the DD of the CCDD) at an ESSENCE visit level. Visits with a DD code (valid or otherwise) are set to 1 (Yes) within ESSENCE “Discharge Diagnosis Available” field going forward. (Note. This variable also measures the presence of a value in the segment, nothing more.)
- Discharge Diagnosis Informative: This indicator was created to distinguish ESSENCE visits containing usable and meaningful dischargediagnosis (the DD of the CCDD) from those that have NO syndromic value. Currently, ESSENCE uses the same list of terms to scan for Discharge Diagnosis as it does to scan for non-informative Chief Complaint. To date, the terms that have been found include the word “null” and a blank space. Although these words in the discharge_diagnosis will mark the data element as complete, they are not meaningful for the purposes of syndromic surveillance.
These features will be useful for daily monitoring of site- and facility-level changes in percentages of CC and DD that are informative or available so that you can take action as needed. For example, you might want to create a dashboard and personalize it with your list of facilities so that monitoring trend lines for dips and spikes can be done at a glance. Put another way, use this filter to track data quality over time and to hone in on data for analysis and visualization.
Please review these Data Quality Filters and contact your site inspectors if you have questions or concerns. As usual, we welcome your feedback!
Questions and Tips
Q: How can I use the data quality filters in NSSP–ESSENCE when running a query?
A: Changes in data quality can affect ESSENCE trend lines. For example, if a query depends heavily on the discharge diagnosis, an improvement in completeness of discharge diagnosis could cause a spike in the data, which would not indicate an actual increase in visits. So, although these filters can be useful in subsetting and analyzing data, always use discretion when drawing conclusions. When observing a spike in the data, use the data quality filters to assess whether the spike is a result of improved data quality or if the number of visits has increased.
Q: How will data quality filters in NSSP–ESSENCE benefit my daily workflow?
A: These filters provide a unique opportunity to track improvements in completeness and meaningfulness of data. You can better observe trends in data and account for variances in data quality when observing spikes. Also, you can use these filters to subset queries and get more complete and meaningful data.
Spotlight on Syndromic Surveillance Practice
Abstracts from the 2019 International Society for Disease Surveillance (ISDS) Annual Conference have been published in a special supplement of the Online Journal of Public Health Informatics (OJPHI). The supplement features more than 200 abstracts representing some of the finest research being done in the United States and around the world. Visit OJPHI.org to read the abstracts.
Harnessing Data Science to Improve Population Health and Public Health Surveillance1

In his introduction to the abstracts from the 2019 ISDS Annual Conference, Scientific Program Chair Peter Hicks says the lens we use to view data science “needs to focus on more than just ‘Big Data’ analytics and information technology (IT). It must also focus on fostering organizational environments and multiagency collaborations that invigorate curiosity and experimentation…” He continues, saying the end product for surveillance is not analysis and summary results. Instead, we need to communicate findings through “…storytelling of illness and disease to influence public health policy and, ultimately, improve population health.”2
Knowing attendees’ interests were broader than data analytics and IT, planners expanded the conference repertoire to include a host of new topics. A lot of stories are told—from “Precarious Data: Crack, Opioids, and Visualizing a Drug Abuse Epidemic” and “Hepatitis C Testing Trends Among Large Commercially Insured Populations” to “Accuracy of ICD Codes for Identification—Review of Chlamydia, Gonorrhea, and Syphilis.” Also, several abstracts about monitoring opioids are included, such as “Comparing Syndromic Data to Discharge Data to Measure Opioid Overdose Emergency Department Visits.” Just skimming the contents is interesting and gives insight into the creative ways that syndromic data can be used.
More abstracts were submitted in 2019 than in previous years, which bodes well for interest in syndromic surveillance. The abstracts are categorized into Policy (1 abstract); Informatics (33 abstracts); Injury Surveillance (31 abstracts); One Health and Beyond (8 abstracts); General Public/Population Health (13 abstracts); Methods and Science in Surveillance (45 abstracts); Communication, Visualization and Reporting (19 abstracts); Global Health Surveillance (11 abstracts); Chronic Disease and Behavior Health Surveillance (16 abstracts); and Infectious and Communicable Disease Surveillance (51 abstracts).
This compilation of work being done in syndromic surveillance is designed to encourage conversation across disciplines and to expand your vision of what can be accomplished.
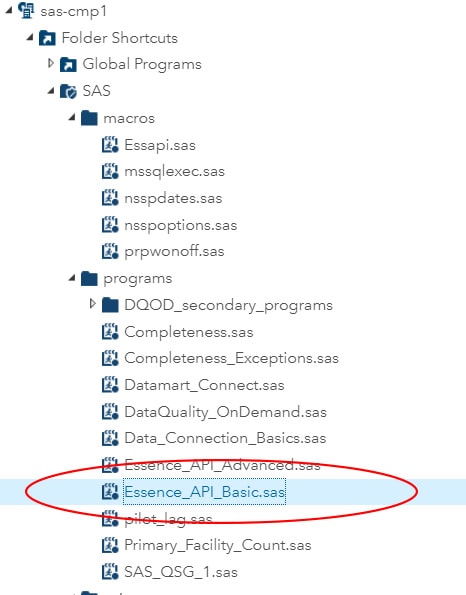
One-stop Shop for SAS Code!
NSSP has developed an improved SAS program to support all ESSENCE application programming interface (API) options including JSON, CSV, and PNG. The program is named ESSENCE_API_Basic.sas and can be found in the SASprograms directory.
The program will accept all ESSENCE API output types and produce a SAS data set that you can use in SAS Studio. All you need to do is paste the ESSENCE API URL into the program, provide the name of the SAS data set to create, and provide the ESSENCE API option being called (JSON, CSV, or PNG).
General
- Annual Server Refresh: NSSP is adding capacity to the production data flow, ESSENCE, and the DataMart.
- Death Indicator Field: In early June 2019, ESSENCE production began prospectively populating the Deathindicator field with Patient_Death_Indicator from the NSSP Processed Tables. The NSSP support team is updating the NSSP Data Dictionary and Enhancements document to reflect this change.
- BioSense Platform Quick Start Guide to Using the Daily Site Processing Summary: Scheduled for publication this month, the guide explains how to use each section of the daily summary. Get details on message processing, status of facilities pending activation, feeds and facilities (alerts, outages), and data flow backlogs.
CDC’s Strategy to Improve Public Health Surveillance

The newly published report Public Health Surveillance: Preparing for the Future chronicles the CDC strategy to improve the agency’s public health surveillance and data capabilities for 3 to 5 years, beginning in 2014. Syndromic surveillance is a core part of this strategy.
Current Month and Upcoming Events
| July 3 | Data Validation Conference Call, 3:00–4:00 PM ET |
| July 16 | Scheduled vendor patches in staging environment: 6:00–10:00 AM ET |
| July 18 | Scheduled vendor patches in production environment: 6:00–10:00 AM ET |
| July 30 | NSSP CoP Call; 3:00–4:30 PM ET; Topic: Preparing for Disaster Surveillance |
Last Month’s Technical Assistance
| June 5 | Held Data Validation Conference Call |
| June 18 | Applied vendor patches in staging environment |
| June 20 | Applied vendor patches in production environment |
| June 27 | Updated the Access & Management Center |
NSSP Participation
A total of 58 sites from 46 states and the District of Columbia participate in NSSP. Currently, there are 4,271 facilities, including 2,893 emergency departments (ED), actively contributing data to the NSSP BioSense Platform. Data from these EDs cover about 66% of all ED visits in the country.
NSSP publishes data for ED visit coverage each quarter. These data and the coverage map shown below were updated April 2019. The calculation method is described in the December 2018 issue of NSSP Update.
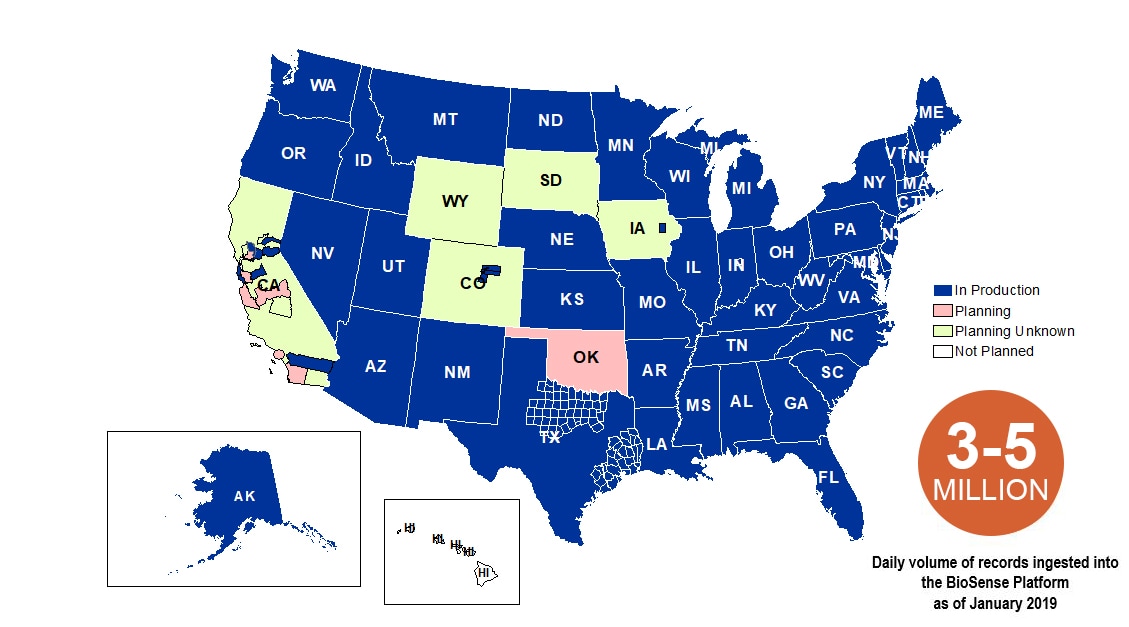
Definitions: NSSP consolidates facilities that provide data under a single data administrative authority called a site administrator. These facilities and single-site administrator constitute a site.
