NSSP Update – June 2019

- Community of Practice
- NSSP CoP Cooperative Agreement is Transitioning
- NSSP Community of Practice Call
- Implementation Guide for Syndromic Surveillance
- CDC Funding Recipients and Partnerships
- North Carolina Integrates DMAT Data to Improve Situational Awareness
- NSSP BioSense Platform User Assessment
- ESSENCE Queries

- Free-text Coding in NSSP– ESSENCE
- Data Quality Corner
- Questions and Tips
- Spotlight Article: Building Site and Local Public Health Capacity in Syndromic Surveillance Through an Online Community of Practice

- Technical Updates
- NSSP and Community Enhance MFT
- May Update to AMC
- Soon to be Published
- Current Month and Upcoming Events
- Last Month’s Technical Assistance
- NSSP Participation
People
Community of Practice
NSSP CoP Cooperative Agreement is Transitioning to a New Partner
- NSSP CoP Transition Schedule
- Transition Letter to CoP Members
- Transition FAQs
- ISDS membership profile—Update by June 14, 2019!
For almost three years, the International Society for Disease Surveillance (ISDS) has facilitated the National Syndromic Surveillance Program Community of Practice (NSSP CoP). ISDS—a leader in health informatics and preparedness activities since 2005—has played a critical role in advancing the science and practice of health surveillance worldwide. Thanks to the ISDS body of work, its facilitation of the NSSP CoP, and the hard work of many dedicated experts in syndromic surveillance, NSSP has a strong, sustainable community of practice.
On May 9, 2019, ISDS and CDC NSSP notified community members that the current cooperative agreement between CDC and ISDS that supports the work of the CoP will end June 30, 2019. It will be replaced with a new partner cooperative agreement being competed through CDC’s Center for State, Tribal, Local, and Territorial Support National Partnership (CSTLTS) cooperative agreement.
As we transition from one cooperative agreement to another, we encourage you to continue your membership in the NSSP CoP and to engage in ongoing community activities. Popular ways to interact with your peers—including workgroups, committees, and monthly NSSP CoP call—will sharpen your surveillance skills and provide valuable sources of information.
Consent to Transfer Your Membership Information from ISDS to CDC
On May 17, 2019, ISDS emailed members with a Subject Line: NSSP CoP Transition_ Continuation of NSSP CoP Membership. Members, if you don’t see the notice in your email, you may want to check your spam folder. In that email, you will see a link where you can provide your consent to have your member profile shared with CDC. If you do not complete this consent form, your NSSP CoP member information will NOT be shared with CDC and you will not receive future CoP communications. If you didn’t receive the email and would like to consent to have your member profile shared with CDC, contact Emilie Lamb (elamb@syndromic.org).
Update your Member Profile
Please take a few minutes to review and update your member profile on healthsurveillance.org. Profiles may be updated until 11:59 PM ET on June 14, 2019. Changes made after this date will not be shared with CDC.
Help Us Bridge the Gap during the Transition
If you’re a NSSP CoP workgroup or committee member, CDC will provide interim support to the CoP groups until the new cooperative agreement has been awarded. Your chair and co-chairs have been provided information to share with you. The work of committees and workgroups is highly valued, and we request your support to ensure minimal disruption to activities.
Please be patient with us as we work through the transition. Syndromic surveillance is an essential part of CDC’s Strategic Surveillance Strategy, and we will continue supporting it and the NSSP CoP throughout the transition and beyond.

NSSP Community of Practice Call

Please join the monthly NSSP CoP call. This call is powered by community members who share guidance, resources, and technical assistance. The call includes a forum for discussion and questions. The next call will be held on June 18, 2019, 3:00–4:30 PM ET. The discussion topic is Heat-related Illness Surveillance.
NSSP Community of Practice Article Published in Public Health Reports
The online May/June 2019 issue of Public Health Reports includes an article about the NSSP Community of Practice: “Building State and Local Public Health Capacity in Syndromic Surveillance Through an Online Community of Practice.” The article was written by Deborah W. Gould, Emilie Lamb, Shandy Dearth, and Krystal Collier. The authors describe the NSSP CoP’s design, membership, activities, and opportunities to use collective knowledge to build syndromic surveillance. (The article is this month’s featured “spotlight article.”)
Implementation Guide for Syndromic Surveillance—New Milestones and Dates!
| HL7 2.5.1 Implementation Guide Milestones* | |
|---|---|
| Time Frame | Activity |
| 2015 | Completed Version 2.0 Final RELEASE** |
| 2016 | Released Erratum and Clarification Documents for Version 2.0 |
| 2017 Summer | Released Version 2.2 Working Draft for Community Comment and Consensus |
| 2017 Winter | Released Version 2.3 for Review and Community Comment |
| 2018 March | Released Version .09 |
| 2018 Spring | Submitted DRAFT HL7 Guide for Balloting: Implementation Guide for Syndromic Surveillance Release 1.0 Standard for Trial Use (STU) HL7 Version 2.5.1 |
| 2018 Fall (October–December) |
|
| 2018 November– 2019 March |
|
| 2019 January | Provided Final Resolution for 33 Comments (Pending) |
| 2019 February |
|
| 2019 March–May |
|
| 2019 June | Hand-off to Technical Steering Committee (2-week review) |
| 2019 July |
|
| 2019 Summer (June–August) |
|
| 2019 September | Release to Public: HL7 2.5.1 Implementation Guide for Syndromic Surveillance for Trial Use Version 1 (STU) |
| 2019 September–November |
|
| 2019 September–2022 September | Standard for Trial Use (STU) for a trial period of 1 to 3 years, during which time additional comments may be submitted and dispositioned (additional releases of the guide would be published) |
* Milestones revised May 20, 2019.
** Version 2.0 is currently being used; subsequent versions are working drafts only.
Shaded activities have been completed.
CDC Funding Recipients and Partnership Updates
North Carolina Integrates DMAT with NSSP Data

Last fall, Category 1 Hurricane Florence brought record-breaking rainfall to North Carolina that led to catastrophic flooding and mandatory evacuations. The North Carolina Division of Public Health (DPH) used its state syndromic surveillance system (NC DETECT) and NSSP to monitor the event. Disaster medical assistance teams (DMATs) filled out the picture, capturing data on health issues among populations in shelters.
CDC’s NSSP team asked DPH officials if they wanted to integrate data from the DMATs deployed in North Carolina with the state’s surveillance data in NSSP. Accepting the offer, data from two DMAT teams in different counties were available through NSSP within 24 hours.
NSSP can quickly integrate data from DMATs whenever they are deployed. Other public health departments might want to update their emergency response plans to include the potential use of this data stream. This story also describes how the North Carolina DPH made its data available graphically and for analyses via data visualizations and dashboards.
Content was provided by Zachary Faigen, the lead for the NC DETECT program at the North Carolina Department of Health and Human Services. Faigen was one of the presenters for the April webinar “Data Sharing through Dashboards: The Who, What, Where, When and Why,” posted in the Knowledge Repository. During this lightening talk webinar, he describes the value of the North Carolina Disease Data Dashboard.
Please Respond to the NSSP BioSense Platform User Assessment

If you’ve used the BioSense Platform in recent months, you most likely received an email inviting you to take part in the NSSP BioSense Platform User Assessment. This assessment evaluates the utility and functionality of the NSSP’s BioSense Platform—from tool performance to Quick Start Guide usefulness and NSSP support.
Your feedback is very important to us. The BioSense Platform is continually enhanced on the basis of user feedback.
The assessment will close June 13, 2019. Participation is voluntary, but we strongly encourage you to provide us with your thoughts and insight. If you have questions or comments about the assessment, please contact the NSSP mailbox at nssp@cdc.gov and select User Feedback-General Feedback or Hussain Yusuf, team lead for the Program Evaluation Team, at hay0@cdc.gov.
ESSENCE QUERIES

Query Terms from April 2019
A key feature of NSSP–ESSENCE is its ability to use free-text definitions across different fields to generate custom queries. The SyS community can use this feature to develop and refine category definitions and to identify and respond to public health events that may not be apparent in established categorical definitions (i.e., syndromes, subsyndromes, and Chief Complaint and Discharge Diagnosis [CCDD] categories).
This word cloud summarizes free-text and coded values that epidemiologists and data analysts queried in ESSENCE during April 2019. This word cloud was generated using the Wordcloud2 package in RStudio. The relative size of the terms suggest the frequency of use in a query. NSSP super administrators can query ESSENCE usage logs to learn what queries are run nationwide and how long they take to complete.
Do you enjoy seeing national-level data depicted in a word cloud? Let us know!
Practice
Free-text Coding in NSSP–ESSENCE
This is the second in a series of articles about how to write ESSENCE free-text queries.
“Part 1. Wildcards” can be found here.

Introduction
The search criteria for ESSENCE free-text queries are built around Boolean logical operators and regular expressions. Free-text queries are not case-sensitive and may contain “^” for wildcards; “,” for multiple entries; “ISBLANK” to look for blanks; “ISNULL” to look for nulls; [COMMA] to look for commas; and operators “and,” “or,”, “andnot,” and parentheses “()” to define order and grouping. This series will cover all these topics in-depth.
Free-text queries are what makes syndromic surveillance practice, particularly practice using NSSP–ESSENCE, adaptable to different data sources and types. By using free-text queries, analysts and epidemiologists can exercise a high level of customization. They can quickly code free-text queries and rapidly respond to outbreaks, disasters, and events that unfold. Such capabilities empower users to customize queries to fit their level of data, ensuring accurate results.
Free-text coding in ESSENCE, which is accessible to all users, follows distinct patterns. Learning to read these patterns allows users to take queries from many places and repurpose them to suit their unique needs. Syndromic surveillance depends heavily on sharing methods, and practitioners must understand the language.
Part 2. Underscores_and Brackets [ ]
Underscores and Brackets are alike in that each represents a single position in a string of numbers, text, or symbols. An Underscore is a placeholder that specifies that something, anything at all, must be in a particular position. A Bracket allows the user to specify what options can appear in that position.
_ Underscores
A placeholder indicating that something must be present in the position.
Let’s assume the following Chief Complaints (CC), previously used in Part 1 Wildcards, and a desire to create a query for fall-related injuries.
- Fall
- Fell getting out of car
- Left arm injury; Fall
- Falling out with friends; Suicidal
- Feels crestfallen
- Patient brought in after falling on face
- Fall; Left wrist injury
- Feels congested; Allergies
You may reasonably assume the boldfaced CCs 1, 2, 3, 6, and 7 are the intended cases and 4, 5, and 8 are false positives.
Here’s a table that shows how the use of the _Underscore can affect results:
| _ Underscore Query Examples | |
|---|---|
| Code | Description |
| ^Fall_^ | An Underscore at the end of a text string means something must follow the text. Returns CCs 4, 5, 6, and 7. Notice the Underscore takes the place of an “e” in CC 5 and a “;” in CC 7. |
| ^_Fall^ | This Underscore at the beginning specifies that something must be before the text. Returns CCs 3, 5, and 6. Notice the Underscore takes the place of a space in CCs 3 and 6. |
| ^_Fall_^ | This specifies something must precede and follow the text. Returns CCs 5 and 6. |
| ^F_ll^ | A common use of Underscores, this Underscore is in the middle of a text string and specifies that something must be in that spot. Returns CCs 1, 2, 3, 4, 5, 6, and 7. |
| ^F__ll^ | Underscores can be used in series. Two in a row means something must be in both spots. Returns CCs 1, 2, 3, 4, 5, 6, and 7. Moving outside of our example CCs, this code would also return the text strings, Feel, Left lower, Fail, and potentially many others. |
Notes on How to Use Underscores in Queries
- To query the Underscore symbol, place it in Brackets: ^[_]^
- Underscores are useful in ICD10-CM queries when the query coder cares about what’s in later digits of the code but does not need to specify what comes before it.
In the following example, the two Underscores in a row indicate that in this definition the “2” in the sixth place indicates intentional self-harm and is the important part of that diagnosis code: ^T39.__2^
It is is common practice to include decimal and non-decimal forms of ICD10 codes in syndrome definitions and free-text code. Use caution when doing this.
If we delete the decimal in the ^T39.__2^ example to create a non-decimal query ^T39__2^, we would pick up the intended non-decimal form ICD10 codes like T39012A and T392X2A—BUT, the query would also capture unintended codes like the ICD10 codes T39.121A or T39.829A. Luckily, this isn’t relevant for our “intentional self-harm” example because there are no valid T39 ICD10 codes with a 2 in the fifth place, but this isn’t true for all codes and could result in the inclusion of unintended visits in your query.
[ ] Brackets
Placeholders that specify items that can be present in a position.
Here’s a table that shows how the use of Brackets can affect results:
| [ ] Bracket Query Examples | |
|---|---|
| Code | Description |
| ^[ ;t]Fall^ | The Brackets near the start mean the text “Fall” must be preceded by a space, semicolon, or a “t”. One and only one of the two bracketed items must precede the term. Returns CCs 3, 5, and 6. |
| ^Fall[ ;i]^ | The Brackets near the end mean that one of the bracketed items must follow the term. Returns CCs 6 and 7. |
| ^[ ;t]Fall[ ;i]^ | The Brackets before and after the term indicate that one of the bracketed items must precede and follow the term. Returns CC 6. |
| ^F[ae]ll^ | This Bracket falls in the middle of a text string. It indicates that an “a” or an “e” must take that place. Returns CCs 1, 2, 3, 4, 5, 6, and 7. |
Notes on Brackets
- Brackets can be troublesome. If your query returns null results, your Brackets might be the source of the issue.
- Brackets can contain ranges like [a-f] or [4-8]. Following are all equivalent Bracket statements:
-
- [0-2] = [012]
- [0123456789] = [0-9] = [0-23-9]
- [a-c] = [abc]
- [0-3a-d] = [0123abcd]
- Bracketed letters are NOT case sensitive.
- Brackets can only take the place of ONE position:
-
- You cannot bracket a number greater than 1 digit.
- [0-24] does NOT give the numbers zero through twenty-four; instead, it will be interpreted as zero through two or four or as the equivalent Bracket [0124].
- Ranges cannot be backwards or looped. Examples of invalid Brackets: [9–2] and [x–a].
- Querying of certain punctuation will only work within Brackets. Examples follow:
-
- [COMMA] to search for commas
- [_] to search for underscores
Examples that Use Underscore and Bracket
Brackets are commonly used in discharge diagnosis (DD) queries. DD codes frequently begin with a bracketed list of punctuation to ensure you get the start of a DD code and that your queried text won’t appear in the middle. Underscores are also useful in DD queries. Note the use of both the Brackets and Underscores in the following excerpt from the CDC Firearm Injury v1 CCDD Category:
…..(,^[;/ ]W3[23]^,andnot,(,^[;/ ]W3[23]___[DS]^,or,^[;/ ]W3[23].___[DS]^,),),…..
This excerpt uses Underscores in its negations. A “D” or an “S” in the seventh place of this ICD10 code indicates that this is a subsequent or sequalae visit and is not an acute firearm injury ED visit. By using a series of Underscores, the writers could specify what they didn’t want in the seventh place without specifying the middle part of the DD code that came before it.
The ICD10 codes in this example specify that the code must be preceded by a semicolon, forward slash, or space. Note the bracketed [23]: this will capture multiple forms with a single statement. For example, the following ESSENCE free-text codes are equivalent, with the second being more concise:
^;W32^,or,^/W32^,or,^ W32^,or,^;W33^,or,^/W33^,or,^ W33^ = ^[;/ ]W3[23]^
Try it out!
Run these two queries in a Discharge Diagnosis field. Notice how the results are the same:
^;W32^,or,^/W32^,or,^ W32^,or,^;W33^,or,^/W33^,or,^ W33^
^[;/ ]W3[23]^
Take a simple query and experiment by replacing letters with an Underscore or a bracketed list. You might find unexpected results when comparing ^Tick^ versus ^T_ck^ versus ^T[aeiou]ck^ or when comparing ^Heroin^ versus ^Her__n^ versus ^her[io][oi]n^
We thank Senior Data Analyst Zachary Stein for volunteering to write a series of articles about free-text coding. Stein, formerly with the Kansas Department of Environment and Health, does epidemiologic work to support NSSP efforts. Stein is an active participant in the NSSP CoP. He initially wrote about free-text coding as an entry on the NSSP CoP Syndrome Definition Committee forum. The forum generated considerable interest, inspiring this series. Stein acknowledges input provided by others who contributed to the forum post.
Data Quality Corner
What’s a NICC?
With last month’s enhancement to ESSENCE, we introduced a new term into our NSSP vocabulary: “NICC,” which stands for non-informative chief complaint. Okay, so why introduce another term? Well, for background, sometimes NSSP receives chief complaint terms that are not informative. By “not informative,” we mean that although the chief complaint may have a non-null value, the value itself may add negligible, if any, value to syndromic surveillance. For example, a chief complaint value of “unknown” is not informative.
Before the enhancement, NSSP–ESSENCE would ingest and store the first non-null chief complaint value sent for a visit, regardless of the value of the chief complaint itself. For example, if the first non-null chief complaint was “unknown,” then ESSENCE’s chiefcomplaintorig and chiefcomplaintparsed columns would retain the value “unknown” despite receiving additional or more informative chief complaint data for that visit. Further, using the same example, the “DD” portion of CCDD would also have “unknown.” This was problematic because there may have been more informative chief complaint data reported for a visit but not reflected in ESSENCE chief complaint fields (including CCDD) and, thus, not considered in some CCDD categories.
The NSSP Community of Practice Technical Committee compiled a list of commonly used NICC terms. (See NICC Terminology table below.) The Technical Committee recommended that NSSP consider alternate processing rules when ingesting chief complaint data into ESSENCE. The new processing rules would account for the possibility of a NICC term being reported as the first non-null chief complaint and the subsequent informative chief complaints not being leveraged. On the basis of this recommendation, the NSSP–ESSENCE ingestion process was modified.
The NSSP ingestion process continues to use the first non-null chief complaint during ingestion, even if the first non-null is a NICC. However, with this recent change, the process will “overwrite” a NICC chief complaint when a subsequent informative chief complaint is reported (in other words, a chief complaint value that is not on the NICC list).
Note: The history field for chief complaint (chiefcomplaintupdates) will store all chief complaints reported, including those terms considered non-informative, or “NICC.” So, you will be able to see those visits that did have a NICC at some point in the history of all chief complaints reported.
Let’s take an example of several messages and records associated with the same visit (ESSENCEID). Notice the ChiefComplaintOrig values reflected in the data reported in the messages. The first non-null is a NICC value: “Chief Complaint Not Present.” However, other messages following this “first message” contain chief complaint data that are more informative.
| rowid | messagedatetime | ChiefComplaintOrig |
|---|---|---|
| 94033777 | 2018-10-15 09:36:39.000 | Chief Complaint Not Present |
| 94033774 | 2018-10-15 09:36:59.000 | Chief Complaint Not Present |
| 94647080 | 2018-10-15 09:59:10.000 | NULL |
| 94647082 | 2018-10-15 09:59:10.000 | NULL |
| 94647076 | 2018-10-15 09:59:50.000 | NULL |
| 94647077 | 2018-10-15 09:59:50.000 | NULL |
| 94647079 | 2018-10-15 11:25:02.000 | Kidney Infection |
| 94647083 | 2018-10-15 11:25:02.000 | Kidney Infection |
| 94647078 | 2018-10-15 11:27:47.000 | Kidney Infection |
| 94647081 | 2018-10-15 11:27:47.000 | Kidney Infection |
| 94033776 | 2018-10-15 16:00:56.000 | Chest Pain |
| 94033775 | 2018-10-15 16:41:36.000 | Chest Pain |
How did ESSENCE process these data before the enhancement?
Here’s what a collapsed “one row” of data in ESSENCE looked like with the original processing rules:
ChiefComplaintOrig ChiefComplaintUpdates
Chief Complaint Not Present {1};Chief Complaint Not Present;|{2};;|{3};Kidney Infection;|{4};Chest Pain
Notice the non-informative value, being the first non-null value, is used as the chief complaint.
How does ESSENCE process these data now?
Here’s what the collapsed “one row” of data in ESSENCE looks like with our new processing rules:
ChiefComplaintOrig ChiefComplaintUpdates
Kidney Infection {1};Chief Complaint Not Present;|{2};;|{3};Kidney Infection;|{4};Chest Pain
Notice the non-informative value is now overwritten with the subsequently reported informative value.
| NICC Terminology | |||||||
|---|---|---|---|---|---|---|---|
| NICC ID | NICC Term | NICC ID | NICC Term | NICC ID | NICC Term | NICC ID | NICC Term |
| 1 | “” | 12 | other | 23 | Ambulance | 34 | Sick |
| 2 | null | 13 | xxx | 24 | EMS/Arrive by | 35 | Evaluation |
| 3 | unknown | 14 | Evaluation | 25 | EMS/Ambulance | 36 | Injury |
| 4 | unknown | 15 | Follow up | 26 | ; | 37 | ill |
| 5 | n/a | 16 | medical | 27 | ;; | 38 | Eval |
| 6 | na | 17 | illness | 28 | Triage | 39 | squad |
| 7 | Chief complaint not present | 18 | General | 29 | Triage peds | 40 | referral |
| 8 | ed visit | 19 | General Symptom | 30 | Triage- | 41 | Code 1 |
| 9 | ed visit | 20 | EMS | 31 | Triage peds- | 42 | Code 3 |
| 10 | er | 21 | AMR | 32 | See chief complaint quote | ||
| 11 | Advice only | 22 | medical | 33 | See CC quote | ||
Questions and Tips
Q: What does an API “response” look like?
A: An application programming interface, or API, is a structured and consistent way for one machine (or application) to exchange information with another machine or application. One machine will make an API request (URL with query parameters and display format) and the other will respond. An API response (the information returned to the requestor) using the ESSENCE APIs is either a table of data or a time series image.
The most common API response is a table. In this example, Table Builder provided output in CSV format (JSON is an option, too). Shown below is a table of counts for a particular Chief Complaint (CC) and Discharge Diagnosis (DD) category by quarter, HHS Region, and National Center for Health Statistics age group. Here, we have sent a request to ESSENCE to summarize certain information for us and then return aggregate results. You can automate this query to update over time and then further summarize or visualize it in whatever way suits your needs.

Resources
R for Data Science, R Markdown: The Definitive Guide, Text Mining with R
This explanation was provided by CDC Health Scientist Aaron Kite-Powell from his presentation at the ISDS 2019 Annual Conference: How to Use RStudio with ESSENCE Application Programming Interfaces.
TIP—How to Make an ESSENCE API URL Shorter. Occasionally, the API URL you created for the ESSENCE query will be very, VERY long. For example, you might have reason to explicitly include all facilities, all counties, or all ZIP codes for a site. Consequently, the URL character length might be too long to assign to the “url <-” object. When this occurs, all you have to do is split the URL into two or more strings when creating objects, and then pull them together later.
In the code chunk shown below, we start with one long URL (use your imagination here) and break it into two pieces. Then, to create the object “url3,” we paste them together. Finally, to create the “url,” we clean-up “url3” by removing the carriage return (added when you separated the original URL by pressing Enter on your keyboard) and replace it with nothing. The final URL can be passed to ESSENCE along with your authentication credentials to return your results.
url1 <- "https://essence.syndromicsurveillance.org/nssp_essence/api/very_very_very_long_URL_ver_long_use_your_imagination_here...." url2 <- "still_going_even_longer_here..........." url3 <- paste(url1, url2, sep="") url <- gsub("\n", "", url3) #Resulting url print(url)
## [1] "https://essence.syndromicsurveillance.org/nssp_essence/api/very_very_very_long_URL_ver_long_use_your_imagination_here....still_going_even_longer_here..........."
TIP for Writing API Authentication Code. To extract data from ESSENCE, you start by passing authentication information from your RStudio session to ESSENCE so that it knows what data you are allowed to see. Never include your username and password in your code. Instead, let the keyring package do the work. When you run this line of code (with your username entered in the username quotes)
key_set(service = “essence”, username = “username”)
a pop-up will appear in RStudio where you can enter your password. (RStudio will store your password for the remainder of the session without rerunning that line of code.) Once you enter your password in the pop-up, be sure to “comment out” this line of code by adding a hash mark before it, as shown below in this code:
httr::set_config(config(ssl_verifypeer = 0L)) library(jsonlite) library(keyring) #key_set(service = "essence", username = "username")
Spotlight on Syndromic Surveillance Practice
Since June 2016, the Centers for Disease Control and Prevention has had a 3-year cooperative agreement with the International Society for Disease Surveillance to facilitate the National Syndromic Surveillance Program’s Community of Practice. Once the Community of Practice had been implemented, the authors examined the value it had added and whether the goals for it had been realized. This Executive Perspective, published in the February issue of Public Health Reports, describes how a community of practice for syndromic surveillance was designed and its effectiveness in building public health capacity.
Building State and Local Public Health Capacity in Syndromic Surveillance Through an Online Community of Practice1

Public health resources (and expertise) vary from jurisdiction to jurisdiction and state to state. The Centers for Disease Control and Prevention (CDC) assists public health departments through funding and technical support. To increase state and local public health capacity in syndromic surveillance, CDC’s National Syndromic Surveillance Program (NSSP) took a two-pronged approach:
- To support the science, CDC NSSP developed technical infrastructure: the BioSense Platform. This cloud-based platform hosts tools and resources for data collection storage, analysis, and exchange.
- To support practice, CDC invested in people. CDC did this by funding a 3-year cooperative agreement to formalize, manage, and facilitate an online community of practice (CoP) for syndromic surveillance1 with the goal of fostering learning and knowledge sharing. The cooperative agreement to support the CoP was competitively bid and awarded to the International Society for Disease Surveillance (ISDS).
The article describes capacity building as “activities that strengthen and maintain the infrastructure and resources necessary to sustain or improve system, organizational, community, or individual processes and competencies.”2 Without the capacity to expertly conduct syndromic surveillance, public health practitioners would be limited in their ability to detect, monitor, and characterize potential public health concerns.
NSSP and ISDS team members searched the literature to identify best practices applicable to CoP design. Through surveys, needs assessments, and discussions with experts in syndromic surveillance, they identified five categories of CoP activities: (1) Community-driven Leadership, (2) Member Participation and Engagement, (3) Collaboration and Networking, (4) Knowledge Sharing and Training, and (5) Problem Solving.
These categories are explained and examples are provided. The category on Community-Driven Leadership, for instance, describes the member-appointed Steering Committee. The Steering Committee is a conduit to the community, identifying knowledge gaps, member needs, and topic areas around which workgroups and subcommittees can be set up to focus on these needs. The Collaboration and Networking category describes how the community rallied to refine the technical specifications for transmitting data (published in the Implementation Guide for Syndromic Surveillance).3 The Knowledge Sharing and Training category cites several examples that demonstrate how public health jurisdictions use syndromic surveillance to improve specific areas of public health.
Further, the article describes the CoP membership, making the point that these analysts, epidemiologists, and other health practitioners who are geographically and professionally isolated have worked together to develop a vibrant community. The CoP’s online collaboration opportunities have stimulated innovation in practice and improved the technical infrastructure for conducting syndromic surveillance. The CoP’s momentum is considerable and it has demonstrated the ability to build capacity.
1Gould DW, Lamb E, Dearth S, Collier K. Public Health Reports [Internet]. 2019 Feb 14 [cited 2019 May 16];134(3):223–227. Available from: https://doi.org/10.1177/0033354919828713
2Centers for Disease Control and Prevention. Strengthening Public Health Systems and Services through National Partnerships to Improve and Protect the Nation’s Health [Internet]. 2018 [cited 2019 May 16]. Available from: https://www.cdc.gov/publichealthgateway/partnerships/capacity-building-assistance-OT18-1802.html
3 Centers for Disease Control and Prevention. Public Health Information Network guides [Internet]. 2018 Dec 19 [cited 2019 May 28]. Available from: https://www.cdc.gov/phin/resources/phinguides.html.
NSSP and Community Collaborate to Enhance the MFT

In early 2019, NSSP began working with a small group of community volunteers to gauge interest and value in using the Master Facility Table (MFT) to update multiple facilities at the same time. Site administrators use the MFT to input facility information to ensure data feeds transmit accurately and produce data as expected. The MFT is an integral part of the Access and Management Center (AMC).
This article summarizes the community recommendations that evolved from the collaboration. The community volunteers recommended that a batch update feature for primary facilities would add considerable value to the MFT. On the basis of their recommendation, the NSSP team plans to start development in 2020, with plans to release an updated AMC in 2020 that adds “batch update” functionality to the MFT.
How Will Batch Update Be Used?
Site administrators have several key reasons for wanting to update primary facilities in batches. They want the ability to change the status of multiple facilities to “Active,” update the parent organization, and update the vendor for several facilities at once.
The community recommended that NSSP consider the following when developing batch update functionality:
- ZIP
- Primary Facility Type
- Local Facility Type
- Parent Organization
- Vendor Name
- Specify Other Vendor Name
- Vendor Software
- Specify Other Vendor Software
- Vendor Version
- Vendor Effective Date
- Feed Name
- Alert Hours
- Temporarily Disable Alerts
- Facility Status
- Date Planed
- Site Comments
Interim Step to Batch Updates
Until the batch update feature can be launched, the NSSP team has provided the community with a template for collecting much of this information. The community is using the template to collect information directly from facilities and finds it quite useful.
Are More MFT Enhancements Needed?
As part of this collaborative effort to enhance the MFT, the community volunteers and NSSP team discussed the need to add or modify associated facility information. Keep in mind that associated facilities must belong to one and ONLY one primary facility. After adding a primary facility, site administrators can link one or more associated facilities to that primary facility and specify the characteristics of the associated facilities.
The community agreed that the MFT’s current functionality, via its “update primary facility” option, met their needs to add more than one associated facility to a given primary facility. Any updating of associated facilities can have major trickle-down effect on the operational crosswalk and data processing workflow. Consequently, NSSP and the community opted to continue this discussion about updating associated facilities before finalizing the enhancement requirements.
The NSSP team thanks the volunteers who participated in conversations to define the requirements for new MFT functionality.
May Update to the AMC
Last month, NSSP successfully put Access & Management Center (AMC) Release 1.4.4 in production. This release removed the yearly audit page and applied bug fixes.
Soon to be Published in Resource Center

BioSense Platform Quick Start Guide to Using SAS Studio—Describes NSSP file retention policy and provides updates about Data Connections Basics program for querying data.
-
BioSense Platform Quick Start Guide to Using the Daily Site Processing Site Summary—Explains how to use each section of the daily summary. Get details on message processing, status of facilities pending activation, feeds and facilities (alerts, outages), and data flow backlogs.
Current Month and Upcoming Events
| June 5 | Data Validation Conference Call, 3:00–4:00 PM ET |
| June 18 | NSSP CoP Call; 3:00–4:30 PM ET; Topic: Heat-related Illness Surveillance |
| June 18 | Scheduled vendor patches in staging environment: 6:00–10:00 AM ET |
| June 20 | Scheduled vendor patches in production environment: 6:00–10:00 AM ET |
Last Month’s Technical Assistance
| May 5 | Held Data Validation Conference Call |
| May 21 | Applied vendor patches in staging environment |
| May 23 | Applied vendor patches in production environment |
NSSP Participation
A total of 58 sites from 46 states and the District of Columbia participate in NSSP. Currently, there are 4,271 facilities, including 2,893 emergency departments (ED), actively contributing data to the NSSP BioSense Platform. Data from these EDs cover about 66% of all ED visits in the country.
NSSP publishes data for ED visit coverage each quarter. These data and the coverage map shown below were updated April 2019. The calculation method is described in the December 2018 issue of NSSP Update.
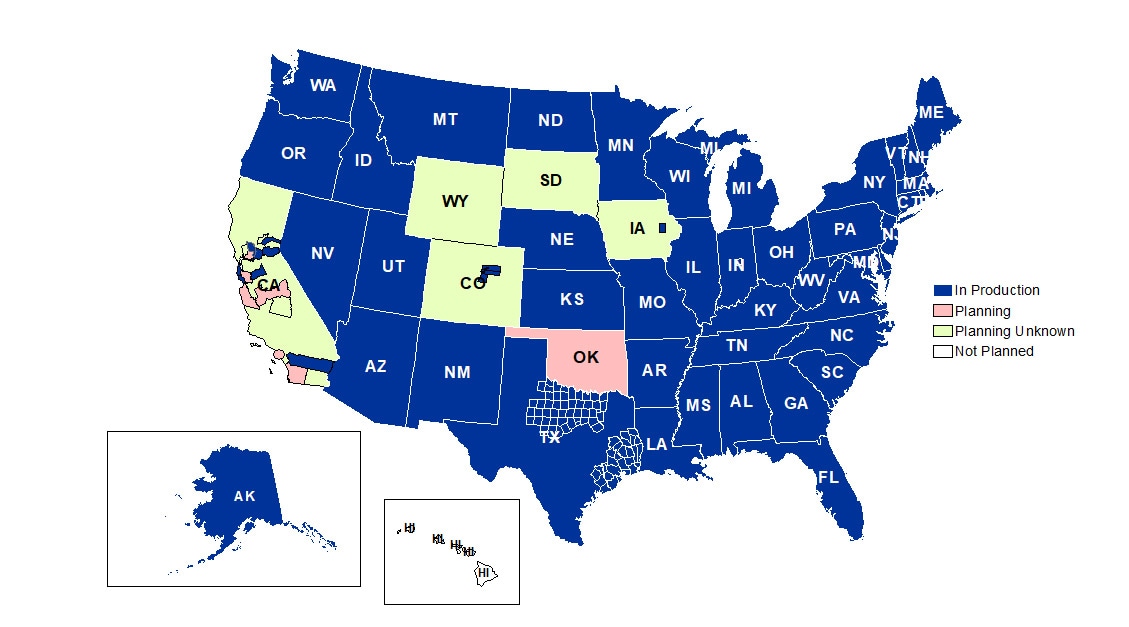
Definitions: NSSP consolidates facilities that provide data under a single data administrative authority called a site administrator. These facilities and single-site administrator constitute a site.
