At a glance
As of November 26, 2025
CDC assessed the risk posed to the United States by the Marburg outbreak in Ethiopia during the next three months. The risk to the general U.S. population is low, with moderate confidence.
The purpose of this assessment is to provide context about the Marburg outbreak in Ethiopia to inform U.S. preparedness efforts. The assessment relied on subject-matter experts’ evaluation of a range of evidence related to risk, including epidemiologic data from the Ethiopia outbreak and historical data on Marburg virus epidemiology and clinical severity. We continue to monitor the outbreak situation and will update this risk assessment if new information warrants changes.
Risk assessment for the general population of the United States
Likelihood
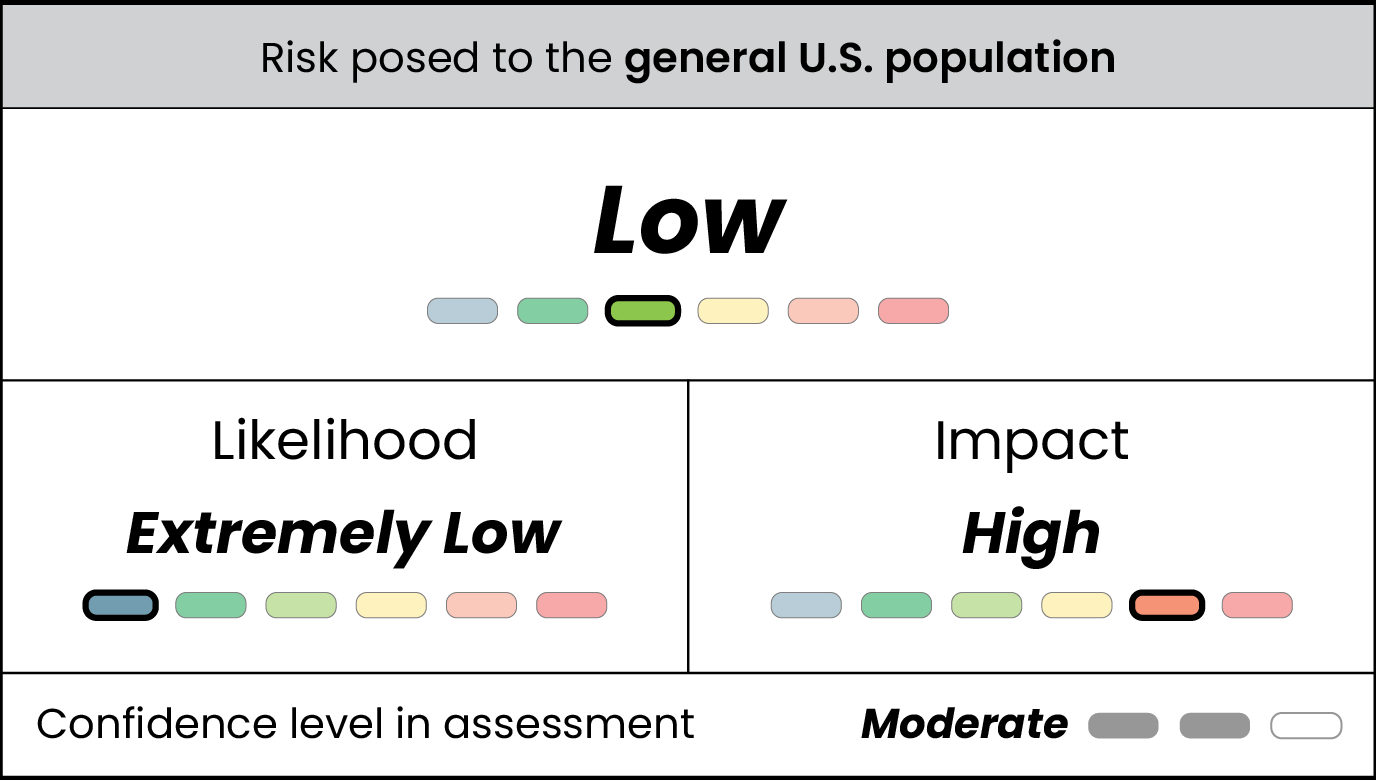
The likelihood of Marburg infections occurring in the U.S. general population is extremely low. Factors that informed our assessment of likelihood include:
- There are no known cases of Marburg in the United States. Available data suggest the outbreak in Ethiopia is currently limited in size. There remains, however, a risk of potential spread from Ethiopia to the United States, via travelers arriving in the United States from Ethiopia who might be infected.
- As of November 26, 2025, 12 confirmed cases of Marburg have been reported in the country's South Region, including seven deaths. This is Ethiopia's first known Marburg outbreak. Investigations are ongoing; the Ministry of Health has reported tracing contacts of the identified cases already and a national and international response has begun.
- Broader spread of Marburg cases within Ethiopia – especially to more populous areas – or to neighboring countries would increase the risk of importation to the United States.
- There are no direct air passenger arrivals from Ethiopia into the United States. Some air passengers may experience short stopovers prior to arrival and air passengers do not change planes.
- The Ethiopian national authorities are scaling up response activities including screening, isolation of cases, treatment, contact tracing, airport exit screening and public awareness campaigns to curb the spread of the Marburg virus.
- CDC recommends travelers to Ethiopia practice usual precautions.
- This is Ethiopia's first Marburg outbreak, and health officials and in-country partners are working to respond to it.
- Since 2001, CDC has worked closely with the Government of Ethiopia and partner organizations to detect, prevent, and control infectious disease outbreaks (including viral hemorrhagic fevers like Marburg), and to build and strengthen the country's core public health capabilities.
- During this outbreak, CDC's Ethiopia Country Office is supporting the Ministry of Health in the response. The country office is also working to provide infection prevention and control supplies and training to reduce risk of further transmission of the disease.
- Nearby countries Tanzania and Uganda have successfully contained their first Marburg outbreaks in 2023 and 2024.
- If Marburg virus is introduced to the United States through a traveler, we expect there could be limited spread before control measures are implemented, as symptoms can appear suddenly and may be similar to many other illnesses.
- While there is no approved vaccine to prevent infection, the United States has a high capacity for implementing case identification, isolation, contact tracing, and infection prevention and control measures that are likely to stop a domestic outbreak before it grows significantly. These measures are likely to be effective in part because the average interval between subsequent cases is long (9 days) and individuals are considered not to be infectious before symptoms appear.
- For example, in 2014-2015, the Ebola virus - a related pathogen - resulted in no community spread and only two infections in healthcare workers in the United States following two introductions and seven medical evacuations from other countries to the United States.
- Additionally, there is a vaccine currently undergoing clinical trials that has been used in other recent Marburg virus outbreaks under an investigative use protocol. There are also treatments, such as monoclonal antibodies and antivirals, being actively researched.
- United States healthcare workers would have an elevated chance of infection if a patient with unrecognized Marburg virus disease were to seek care in the United States.
- Some of the suspected cases in the Ethiopia outbreak are in healthcare workers. Healthcare workers have been disproportionately affected during past Marburg outbreaks (e.g., in the 2024 outbreak in Rwanda, more than 80% of confirmed cases were in healthcare workers).
- Marburg infections in this group could result in spread to close contacts if not detected immediately.
Impact
The impact of Marburg infections occurring in the U.S. general population would be high. Factors that informed the assessment of impact included the following:
- Marburg virus disease is a serious, sometimes deadly disease. During past outbreaks, between 20% and 90% of people infected with the virus died. However, many patients who died in past outbreaks were in locations that did not have access to the level of care that is available in U.S. intensive care units. Currently, treatment for Marburg is limited to supportive care, including rest, hydration, managing oxygen status and blood pressure, and treatment of secondary infections.
- There are no Food and Drug Administration (FDA)-approved treatments or vaccines currently available. However, investigational vaccines and treatments are available and could be utilized in limited scenarios under clinical trial settings, should the need arise and if appropriate FDA authorizations were approved.
- Even very limited Marburg virus spread in the United States could cause significant fear among the public. In addition to the lives directly affected, Marburg virus spread would require significant public health resources, risk communication, and community engagement. Containment requires extensive contact tracing activities, long quarantine for people with high-risk exposures (up to 21 days), and stringent barrier protection measures for healthcare workers and laboratory personnel.
Confidence
We have moderate confidence in this assessment.
We note uncertainty in the implications for the United States of the Marburg outbreak in Ethiopia, including uncertainties related to limited visibility on the epidemiology of the current outbreak in Ethiopia, the potential for geographic spread beyond Ethiopia's South Region, and the extent to which measures are in place to limit transmission.
Factors that could change our assessment
We continue to monitor for additional factors that could change our risk assessment, including:
- Detection of Marburg cases in the United States
- The outbreak in Ethiopia intensifying in Ethiopia or spreading to other countries in the region or globally, raising the likelihood of imported cases in the United States
- Release of further information related to this outbreak that reveals more extensive transmission than currently reported
- Any evidence suggesting increased Marburg transmissibility compared to past outbreaks
- Any evidence of changed clinical severity compared to past outbreaks · Evidence from clinical trials for vaccines and/or treatments
Background
On November 14, 2025, Ethiopia's Ministry of Health reported suspect cases of viral hemorrhagic fever in the country's South Region in the town of Jinka. As of November 26, 2025, Ethiopia has reported that 12 patients have been confirmed positive for Marburg virus, seven of whom have died. Other potential illnesses remain under investigation.
Jinka has an estimated population of at least 20,000 people and is the largest town in the administrative zone. While Jinka has a domestic airport, it has limited road networks and is distant from major urban centers.
This is the first reported Marburg outbreak in Ethiopia, but CDC has worked closely with the Government of Ethiopia and partner organizations to build and strengthen the country's core public health capabilities since opening an office in Ethiopia in 2001. Ethiopia's Ministry of Health has responded swiftly and is working with regional and global partners to deploy technical staff, supplies, and other resources to the region.
Marburg virus disease is a rare, severe viral hemorrhagic fever in the same viral family as Ebola virus. The Marburg virus is most commonly found in sub-Saharan Africa. The virus is found in Egyptian Rousette fruit bats and can spread from infected bats to people through the bats' saliva, urine, blood and feces. Once the disease has "spilled over" from wildlife to people, people who are sick can spread the disease to other people. Infections are spread through direct contact with body fluids–through broken skin or mucous membranes in the eyes, nose, or mouth–or through contaminated objects such as bedding or medical equipment.
People with Marburg usually start getting sick five to 10 days after infection, although this time can range from two to 21 days. Symptoms can appear suddenly and may include fever, vomiting, diarrhea, rash, and severe bleeding. There are no specific treatments or vaccines that are FDA-approved for Marburg virus, although candidate vaccines and treatments are under development and evaluation.
Groups at higher risk of acquiring Marburg include:
- People, including healthcare workers, who are caring for individuals sick with Marburg without proper protective equipment and procedures
- People in contact with Egyptian Rousette fruit bats or their excretions in countries where the bats are found
- People in contact with infected nonhuman primates in countries where the bats are found
CDC is supporting response efforts:
- CDC's Ethiopia Country Office is supporting the country's Ministry of Health in the response.
- The country office is providing infection prevention and control supplies and training to reduce risk of further disease transmission.
- CDC and its partners across Africa continue to work together to investigate the outbreak, help ensure local laboratories have adequate testing capacity, train local laboratory and public health staff, and advise on treatment practices and proper protection protocols for healthcare workers.
- On November 17, 2025, CDC published a Level 1 Travel Health Notice for Ethiopia and is raising awareness of the outbreak among public health professionals in the United States.
- CDC, through its Ethiopia Country Office, routinely works with the Government of Ethiopia and partner organizations to develop public health capabilities such as a national disease surveillance system, implementation of laboratory safety guidance, public health workforce training, and emergency management capacity-building. This partnership has included training on detecting and responding to viral hemorrhagic fever outbreaks.
Methods
CDC subject-matter experts specializing in risk assessment methods, infectious disease modeling, global health, and Marburg virus and other filoviruses collaborated to develop this rapid assessment. Experts initially convened in November 2025 to discuss the need for an assessment examining the risks to the United States posed by the Marburg virus outbreak in Ethiopia, key evidence related to this outbreak, and specific populations to include in the assessment. To conduct this assessment, experts considered evidence including epidemiologic data from the ongoing Marburg virus outbreak in Ethiopia and historical data on Marburg virus outbreaks in central and eastern Africa. CDC staff in-country, supporting the Government of Ethiopia's response, helped to provide local context.
Risk was estimated by combining the likelihood of infection and the impact of the disease. For example, low likelihood of infection, combined with high impact of disease, would result in moderate risk. The likelihood of infection refers to the probability that members of the general U.S. population would acquire Marburg virus disease over the next three months, which in turn depends on the likelihood of exposure, infectiousness of the disease, and susceptibility of the population. The impact of infection considers several factors affecting the consequences of infection, including the severity of disease, level of population immunity, availability of treatments and vaccines, and necessary public health response resources. A degree of confidence was assigned to each level of the assessment, taking into account evidence quality, extent, and corroboration of information.
For more details on our methods, please see our rapid risk assessment methods webpage.