At a glance
Summary
Updated CDC vaccination recommendations for adults are published annually. To assess vaccination coverage among adults aged ≥19 years, CDC analyzed data from the National Health Interview Survey (NHIS). The NHIS is a continuous, cross-sectional national household survey of the noninstitutionalized U.S. civilian population. Interviews are conducted over the course of the year in a probability sample of households, and data are compiled and released on an annual basis. For this report, adult receipt* of influenza, pneumococcal, and herpes zoster vaccines (including any type of herpes zoster vaccine, zoster vaccine live [ZVL] or recombinant zoster vaccine [RZV]) was assessed using the data collected in 2023. Recent trends in adult vaccination were examined using data from 2018–2023.
Coverage among recommended age groups for all vaccines differed by race and ethnicity with generally lower coverage among Black and Hispanic adults compared with White adults**. Linear trend tests indicated that since 2018, coverage increased for any type of herpes zoster vaccination among adults aged ≥50 years, remained stable for influenza vaccination (aged ≥19 years) and pneumococcal vaccination among adults aged 19–64 years at increased risk of disease, and decreased for pneumococcal vaccination among adults aged ≥65 years. While the overall trend for influenza vaccination among adults aged ≥19 years with high-risk conditions demonstrates increased coverage, coverage has plateaued since the 2020–21 season. Coverage with ≥2 doses of RZV among adults aged ≥50 years increased from 1.1% in 2018, when RZV was first recommended, to 24.1% in 2023.
Substantial improvement in adult vaccination uptake is needed to reduce the burden of vaccine-preventable diseases nationally.
Methods
The NHIS is a continuous, cross-sectional national household survey of the noninstitutionalized U.S. civilian population conducted by the U.S. Census Bureau for CDC's National Center for Health Statistics.1 The objectives of the NHIS are to monitor the health of the U.S. population and provide estimates of health indicators, health care use and access, and health-related behaviors.2 Respondents aged ≥19 years with interviews conducted during August 2022–June 2023 (for influenza vaccination) and January 2023–December 2023 (for pneumococcal and herpes zoster vaccination) were included in this analysis. The total sample of persons aged ≥19 years was 29,234 in 2023. The final sample adult core response rate was 47.0% for the 2023 NHIS. One adult from each family in the household was randomly selected and asked questions regarding their receipt of adult-recommended vaccinations. Vaccination questions included in the 2023 NHIS were as follows:
- For influenza vaccination, respondents were asked if they had received an influenza shot or nasal spray during the preceding 12 months and, if so, in which month and year;
- For pneumococcal vaccination, respondents were asked if they had ever had a pneumonia shot; and,
- For herpes zoster vaccination, respondents were asked if they had ever received a shingles vaccine and, if yes, in which year; ever had RZV (if shingles vaccine was received in 2017 or later), and number of RZV doses received.
Weighted data were used to produce national vaccination coverage estimates. The weighted proportion of respondents who reported receiving selected vaccinations was calculated for non-influenza adult vaccination coverage estimates. Influenza vaccination coverage was assessed separately using season-specific approach and the Kaplan-Meier survival analysis procedure was used to assess season-specific influenza vaccination coverage.3 Race and ethnicity were categorized into five mutually exclusive groups: White, Black, Hispanic, Asian, and other. In this report, persons were included in White, Black, Asian, or other race categories if they did not report Hispanic ethnicity. Persons who reported Hispanic ethnicity were classified as Hispanic in the analyses regardless of reported race. Other race was defined as non-Hispanic persons reporting American Indian, Alaska Native, Native Hawaiian, Pacific Islander, or any other race and persons who reported multiple races.
Point estimates and 95% confidence intervals (CIs) were calculated using SUDAAN software (Research Triangle Institute, Research Triangle Park, NC, version 11.0.1) to account for the complex sample design. Changes in vaccination coverage for pneumococcal and herpes zoster were assessed by calculating the simple difference between 2022 and 2023. T-tests were used to compare data years and by each level of each respondent characteristic to a chosen referent level (e.g., for race and ethnicity, White was the reference group). Statistical significance was defined as p<0.05. Coverage estimates are not reported for small sample size (n<30) or large relative standard errors (standard error/estimate >0.3). Trends in adult vaccination were assessed from 2018 through 2023 for influenza, pneumococcal, and herpes zoster vaccinations using weighted linear regression of annual estimates using the inverse of estimated variances of the estimates as weights. Tetanus vaccination data (respondents were asked if they had received a tetanus shot in the past 10 years) were assessed in 2018, 2019, and 2022 due to the NHIS survey question rotation every three years starting in 2019 and are included in the trend figure for a more complete picture of adult vaccination coverage.
Results
- Overall, coverage with ≥1 dose of any type of pneumococcal vaccine among adults aged 19–64 years at increased risk for pneumococcal disease was 23.4% in 2023, similar to the estimate for 2022.
- Coverage with ≥1 dose of any type of pneumococcal vaccine among adults aged ≥65 years was 65.6%, similar to the estimate for 2022.
- Coverage among White adults aged ≥65 years (69.1%) was higher compared with Black (53.9%), Hispanic (54.2%), and Asian (55.1%) adults.
- Overall, coverage with ≥1 dose of any type of herpes zoster vaccination among all adults aged ≥19 years with an indication for vaccination (adults aged ≥50 years or adults aged ≥19 years with weakened immune systems) was 38.3% in 2023, higher than the estimate for 2022 (34.4%).
- White adults aged ≥19 years with an indication had higher coverage (41.8%) compared with Black (28.7%), Hispanic (27.4%), and other race adults (35.3%).
- Coverage with ≥1 dose of any type of herpes zoster vaccination was 40.4% among adults aged ≥50 years and 47.6% among adults aged ≥60 years in 2023, higher than estimates for 2022.
- White adults aged ≥50 and ≥60 years had higher coverage compared with Black, Hispanic, and other race adults.
- Coverage with ≥1 dose of any type of herpes zoster vaccination was 26.7%, 8.1%, and 40.0% among adults aged ≥19, 19–49, and ≥50 years with weakened immune systems, respectively.
- RZV coverage (≥2 doses) was 22.7% among adults aged ≥19 years with an indication and 24.1% among all adults aged ≥50 years: 17.5% among adults aged 50–59 years, 24.3% among adults aged 60–64 years, and 28.7% among adults aged ≥65 years in 2023, all higher than estimates for 2022.
- Coverage was 27.5% among adults aged ≥60 years, higher than the estimate for 2022 (21.4%).
- Coverage was 14.9%, 2.4%, and 23.9% among adults aged ≥19, 19–49, and ≥50 years with weakened immune systems, respectively.
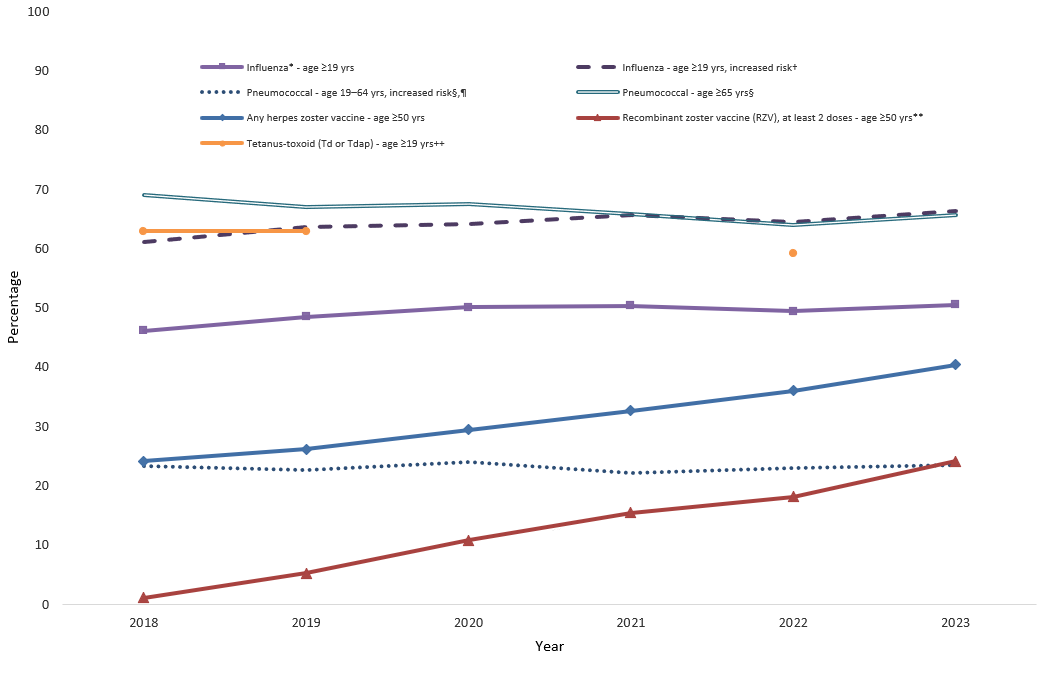
- Trends in coverage from 2018–2023 with selected vaccines recommended for adults are shown in Figure 1.
- Increases in coverage from 2018–2023 were observed for influenza vaccination among adults aged ≥19 years at high risk (annual average percentage point increase: 0.9%, 95% CI: 0.3, 1.5).
- However, coverage was similar from the 2020–21 through 2022–23 seasons.
- Increases in coverage from 2018–2023 were observed for any herpes zoster vaccination among adults aged ≥50 years (annual average percentage point increase: 3.3%, 95% CI: 3.0, 3.6).
- Coverage with ≥2 doses RZV among adults ≥50 years increased from 1.1% in 2018 to 24.1% in 2023 (annual average percentage point increase: 4.5%, 95% CI: 4.2, 4.9).
- Decreases in coverage were observed for pneumococcal vaccination among adults aged ≥65 years (annual average percentage point decrease: -0.8%, 95% CI: -1.1, -0.5).
- Coverage for pneumococcal vaccination among adults aged 19–64 years at increased risk remained stable from 2018 to 2023.
- Tetanus vaccination coverage among adults aged ≥19 years decreased from 62.9% in 2018 and 2019 to 59.2% in 2022.
Discussion
NHIS data from 2023 indicate that many adults in the United States remained unprotected against vaccine-preventable diseases. Overall vaccination trends indicated that, for the years assessed, influenza (adults aged ≥19 years at increased risk) and herpes zoster vaccination coverage increased. Still, influenza vaccination coverage (adults aged ≥19 years at high risk) has plateaued since the 2020–21 season, and coverage with ≥2 doses of RZV is still relatively low across age groups, including for those ≥19 years with weakened immune systems for whom ACIP recommended vaccination in October 2021.4 Pneumococcal vaccination coverage remained stable among adults aged 19–64 years at increased risk of disease and decreased among adults aged ≥65 years. Differences in vaccination coverage by race and ethnicity persist for all vaccines, with generally lower coverage among Black and Hispanic adults compared with White adults.
Pneumococcal vaccination coverage among adults aged ≥65 years decreased, especially during the COVID-19 pandemic period. Separate analyses of adults aged 65–70 years eligible for pneumococcal vaccination during 2015–2022 showed a pandemic effect on pneumococcal vaccination coverage; reductions in persons accessing vaccination services among older adults may have resulted in a modest decrease in pneumococcal vaccination coverage (56 , CDC unpublished data). Similar findings were observed using data collected from the Behavioral Risk Factor Surveillance System (5 , CDC unpublished data). While recommendations for pneumococcal vaccination have changed over time, throughout this study period, one or more doses of 23-valent pneumococcal polysaccharide vaccine (PPSV23) or pneumococcal conjugate vaccine (PCV), alone or in combination, were recommended for all adults ≥65 years and 19–64 years at increased risk for pneumococcal disease, depending on age, risk condition, and vaccination history.7 The NHIS does not distinguish between PCV and PPSV23, which may affect the interpretation of vaccination coverage data.
Limitations
The estimates in this report are subject to several limitations. First, all data relied on respondent self-report and were not validated with medical records. However, adult self-reported vaccination status has demonstrated ≥70% sensitivity and specificity for influenza and pneumococcal vaccines and zoster vaccine live in one or more studies.8910 Questions specifically addressing recombinant zoster vaccine were only asked if a respondent reported receiving a herpes zoster vaccine in 2017 or later and recall accuracy for type of herpes zoster vaccine (i.e., ZVL or RZV) has not been reported. Second, the NHIS response rate was 47.0% in 2023. Nonresponse bias can result if respondents and non-respondents differ in their vaccination behaviors and if survey weighting does not fully correct for this. Finally, the NHIS sample excludes persons in the military and those residing in institutions, which might result in underestimation or overestimation of adult vaccination coverage levels.
Conclusions
Coverage of routinely recommended vaccines among adults remains low. Differences in vaccination coverage by race and ethnicity were seen for all vaccines assessed. Ensuring access to and increasing uptake of recommended vaccines is needed to maximally reduce the burden of vaccine-preventable diseases.
Authors
Mei-Chuan Hung, MPH, PhD1,2; Anup Srivastav, B.V.Sc.&A.H., MPVM, PhD1,2; Peng-jun Lu, MD, PhD1; Carla L. Black, PhD1; Charleigh J. Granade, MPH1; Tara C. Anderson, DVM, PhD3; James A. Singleton, PhD1
1Immunization Services Division, National Center for Immunization and Respiratory Diseases, CDC 2 Eagle Health Analytics, Inc, Atlanta, GA
3Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC
Footnotes
*The following are the current recommendations for adult vaccinations:
Influenza: annual vaccination is recommended for all adults aged ≥19 years.
Pneumococcal: previously recommended for adults aged 19–64 years at increased risk and those aged ≥65 years; Since October 2024 (after data collection for this report), it is recommended for those aged ≥50 years as well as adults aged 19–49 at increased risk.
Herpes zoster: recombinant zoster vaccine is recommended for adults aged ≥50 years, and for adults aged ≥19 years with weakened immune systems.
**In this report, persons identified as White, Black, Asian, or other race are non-Hispanic. Persons identified as Hispanic might be of any race. "Other" includes American Indian/Alaska Native, Native Hawaiian, Pacific Islander, or any other race and persons who identified multiple races. The five racial/ethnic categories are mutually exclusive.
- National Center for Health Statistics. Survey description, National Health Interview Survey, 2023. Hyattsville, Maryland. 2023. Available at: https://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHIS/2023/srvydesc-508.pdf.
- National Center for Health Statistics. Public-use data file and documentation. Available at: https://www.cdc.gov/nchs/nhis/about/.
- Lu PJ, Santibanez TA, Williams WW, Zhang J, Ding H. et al. Surveillance of influenza vaccination coverage—United States, 2007-08 through 2011-12 influenza seasons. MMWR Surveill Summ. 2013 Oct 25;62(4):1-28. Available at: https://www.cdc.gov/mmwr/preview/mmwrhtml/ss6204a1.htm.
- Anderson TC, Masters NB, Guo A, et al. Use of recombinant zoster vaccine in immunocompromised adults aged ≥19 years: recommendations of the Advisory Committee on Immunization Practices — United States, 2022. MMWR Morb Mortal Wkly Rep 2022;71:80–84. DOI: http://dx.doi.org/10.15585/mmwr.mm7103a2.
- CDC. Pneumococcal vaccination among adults 65–70 years of age before and during the COVID-19 pandemic— United States, 2021. Available at: https://www.cdc.gov/adultvaxview/publications-resources/pandemic-impact-on-ppv.html.
- Czeisler MÉ, Marynak K, Clarke KEN, et al. Delay or avoidance of medical care because of COVID-19–related concerns—United States, June 2020. MMWR Morb Mortal Wkly Rep 2020;69(36):1250–1257. doi: 10.15585/mmwr.mm6936a4.
- Kobayashi M, Pilishvili T, Farrar JL, et al. Pneumococcal Vaccine for Adults Aged ≥19 Years: Recommendations of the Advisory Committee on Immunization Practices, United States, 2023. MMWR Recomm Rep 2023;72(No. RR-3):1–39. doi: 10.15585/mmwr.rr7203a1.
- Rolnick SJ, Parker ED, Nordin JD, et al. Self-report compared to electronic medical record across eight adult vaccines: do results vary by demographic factors? Vaccine 2013;31(37):3928–3935. doi: 10.1016/j.
- Donald RM, Baken L, Nelson A, Nichol KL. Validation of self-report of influenza and pneumococcal vaccination status in elderly outpatients. Am J Prev Med. 1999; 16:173–177. doi: 10.1016/s0749-3797(98)00159-7.
- Zimmerman RK, Raymund M, Janosky JE, et al. Sensitivity and specificity of patient self-report of influenza and pneumococcal polysaccharide vaccinations among elderly outpatients in diverse patient care strata. Vaccine. 2003; 21:1486–1491. doi: 10.1016/s0264-410x(02)00700-4.