Key points
- An anthrax-like illness has been documented in welders and other metalworkers.
- Welder's anthrax is defined as pneumonia in a metalworker caused by bacteria within the B. cereus group that produces anthrax toxin.
- Symptoms include fever or chills, cough, dyspnea, and hemoptysis.
- Patients should receive prompt treatment with antibiotics and anthrax antitoxin.
Overview
Welder's anthrax refers to a serious infectious disease caused by an anthrax toxin-expressing species within the Bacillus cereus group. It manifests as a severe, rapidly progressive pneumonia with systemic illness in welders and other metalworkers. It has a high fatality rate.
Causes
Several studies have shown an increased risk of pneumonia and death among welders and other workers exposed to metal fumes and mineral dusts. Research suggests it is possible that exposure to metal fumes might increase susceptibility to lung infection, even with common, relatively harmless infectious agents. Furthermore, iron oxide deposited in the lungs after inhaling welding fume has been found in the lungs for years, even after removal from exposure.
How metal fumes cause disease is mostly unknown. Theories include that metal fumes (or iron) act as a growth nutrient for bacteria, enhance the binding of bacteria to lung tissues, or impair immune responses in the lung through oxidative stress. Like all pathogens, B. anthracis and B. cereus anthrax toxins need iron to survive and thrive.
While iron overload might partially explain the increased susceptibility of welders for B. cereus infections, exposure is still important. Several researchers have noted that soil iron is much higher around welding sites than elsewhere. Future research measuring soil iron levels may provide useful information.
Known cases
CDC has identified 9 U.S. cases of welder's anthrax from 1994-2024.
- All patients were metalworkers, and 8 were welders.
- All patients worked in either Texas or Louisiana.
- 6 of the 9 patients died.
- All patients presented with severe pneumonia and were hospitalized. Among those that survived past the emergency room, all were admitted to the intensive care unit and received antibiotics.
- 2 of 3 surviving patients received antitoxin.
Clinical features
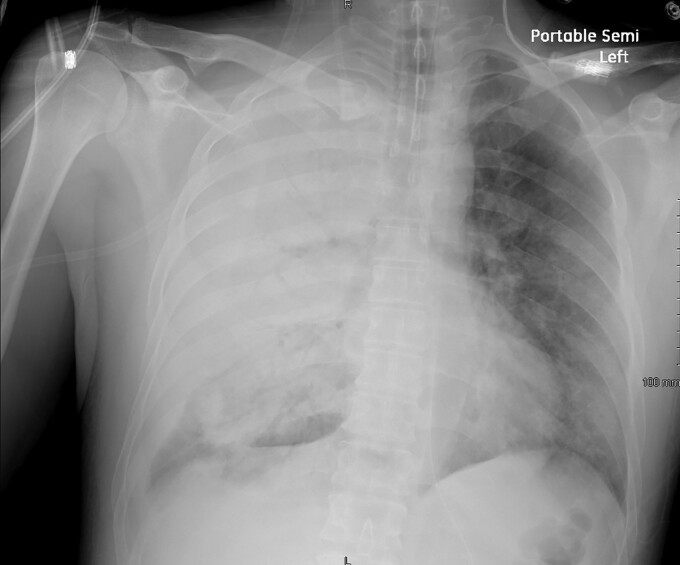
People diagnosed with welder's anthrax had abnormal chest imaging, including pneumonia and pleural effusions. Clinicians should suspect welder's anthrax if a welder or metalworker has a severe, rapidly progressive pneumonia. Mediastinitis, which is usually seen in anthrax, is not typical in welder's anthrax.
Welder's anthrax signs and symptoms are similar to inhalation anthrax and affects the lungs. These include:
- Fever or chills
- Cough
- Dyspnea
- Hemoptysis or bloody sputum
Testing
Healthcare providers in the United States rarely see a patient with welder's anthrax. CDC guidance is available to help doctors diagnose welder's anthrax and order necessary diagnostic tests.
The only ways to confirm a diagnosis of welder's anthrax are to:
- Test for presence of anthrax toxin genes from B. cereus group bacteria isolated from a clinical sample
- Measure anthrax toxin in blood
Take patient samples before the patient begins taking antibiotics if it does not delay the start of treatment.
Patient management
Antibiotics
Treatment of suspected welder's anthrax initially follows guidelines for systemic anthrax with modifications based on susceptibility testing, if available. Since the B. cereus group has different innate susceptibilities than B. anthracis, modifications can be made based on susceptibility testing, if available.
Given the severity of these infections, treatment will generally be started empirically prior to confirmation. Patients should receive:
- Two bactericidal agents from different antimicrobial drug classes
- PLUS one protein synthesis inhibitor OR an RNA synthesis inhibitor (RNAI)
Anthrax antitoxin
After anthrax toxins have been released in the body, one possible treatment is anthrax antitoxin. Doctors must use antitoxin together with other treatment options, including antibiotics.
Anthrax antitoxin is only available through the Strategic National Stockpile.
Reporting
Welder's anthrax is a reportable disease in all U.S. states and territories. Welder's anthrax cases must be reported to state and territorial jurisdictions when identified by a healthcare provider, hospital, or laboratory. Specific requirements for who must report cases and when to report vary by jurisdiction.
Resources
- Welder's Anthrax | Blogs | CDC
- Welder's Anthrax: A Review of an Occupational Disease
- Welder's Anthrax: A Tale of 2 Cases - PMC
- Prevention and Treatment of Anthrax in Adults (2023): Results of CDC Expert Panels
- Collecting Samples to Send to Laboratories
- Torén, K.; Blanc, P.D.; Naidoo, R.N.; Murgia, N.; Qvarfordt, I.; Aspevall, O.; Dahlman-Hoglund, A.; Schioler, L. Occupational Exposure to Dust and to Fumes, Work as a Welder and Invasive Pneumococcal Disease Risk. Environ. Med. 2019, 77, 57–63.
- Koh, D.H.; Moon, K.T.; Kim, J.Y.; Choe, S.W. The Risk of Hospitalisation for Infectious Pneumonia in Mineral Dust Exposed Industries. Environ. Med. 2011, 68, 116–119.
- Torén, K.; Qvarfordt, I.; Bergdahl, I.A.; Järvholm, B. Increased Mortality from Infectious Pneumonia after Occupational Exposure to Inorganic Dust, Metal Fumes and Chemicals. Thorax 2011, 66, 992–996.
- Wong, A.; Marrie, T.J.; Garg, S.; Kellner, J.D.; Tyrrell, G.J.; SPAT Group. Welders Are at Increased Risk for Invasive Pneumococcal Disease. J. Infect. Dis. 2010, 14, e796–e799.
- Palmer, K.T.; Cullinan, P.; Rice, S.; Brown, T.; Coggon, D. Mortality from Infectious Pneumonia in Metal Workers: A Comparison with Deaths from Asthma in Occupations Exposed to Respiratory Sensitisers. Thorax 2009, 64, 983–986.
- Marongiu, A.; Hasan, O.; Ali, A.; Bakhsh, S.; George, B.; Irfan, N.; Minelli, C.; Canova, C.; Schofield, S.; De Matteis, S.; et al.. Are Welders More at Risk of Respiratory Infections? Findings from a Cross-sectional Survey and Analysis of Medical Records in Shipyard Workers: The WELSHIP Project. Thorax 2016, 71, 601–606.
- Lockey, J.E.; Schenker, M.B.; Howden, D.G.; Desmeules, M.J.; Saracci, R.; Sprince, N.L.; Harber, P.I. Current Issues in Occupational Lung Disease. Rev. Respir. Dis. 1988, 138, 1047–1050.
- Kalliomaki, P.-L.; Kalliomaki, K.; Rahkonen, E.; Aittoniemi, K. Lung Retention of Welding Fumes and Ventilatory Lung Functions. A Follow-Up Study among Shipyard Welders. Occup. Hyg. 1983, 27, 449–452.
- Coggon, D.; Inskip, H.; Winter, P.; Pannett, B. Lobar Pneumonia: An Occupational disease in Welders. Lancet 1994, 344, 41–43.
- Dheeba, B.; Sampathkumar, P. Evaluation of Heavy Metal Contamination in Surface Soil around Industrial Area, Tamil Nadu, India. J. Chem. Tech. Res. 2012, 4, 1229–1240.
- Adekeye, E.A.; Ojo, M.A.; Ajayi, O.O. Contributions of Metal Welding Workshops to Environmental Pollution in Akure Metropolis, Ondo State, Nigeria. Environ. Iss. Agric. Dev. Ctry. 2011, 3, 1–7.