
Overview
More than 800,000 people in the U.S. live with end-stage kidney disease, and more than half of them belong to a racial or ethnic minority group. High blood pressure and diabetes are medical conditions that increase a person’s risk of developing end-stage kidney disease. Some people with end-stage kidney disease have a kidney transplant, but most receive dialysis treatments (a process of filtering and removing waste products and excess fluid from the body).
Dialysis treatment puts patients at higher risk for serious infections because it requires frequent access to the bloodstream using needles or catheters (soft plastic tubes inserted into large veins). If germs get into a patient’s blood, they can cause serious infections that may lead to sepsis (a potentially life-threatening immune system response) and even death. Many germs can cause dialysis bloodstream infections. The most common is a group of germs called Staphylococcus aureus (staph). Staph infections can be difficult to treat and may be deadly.
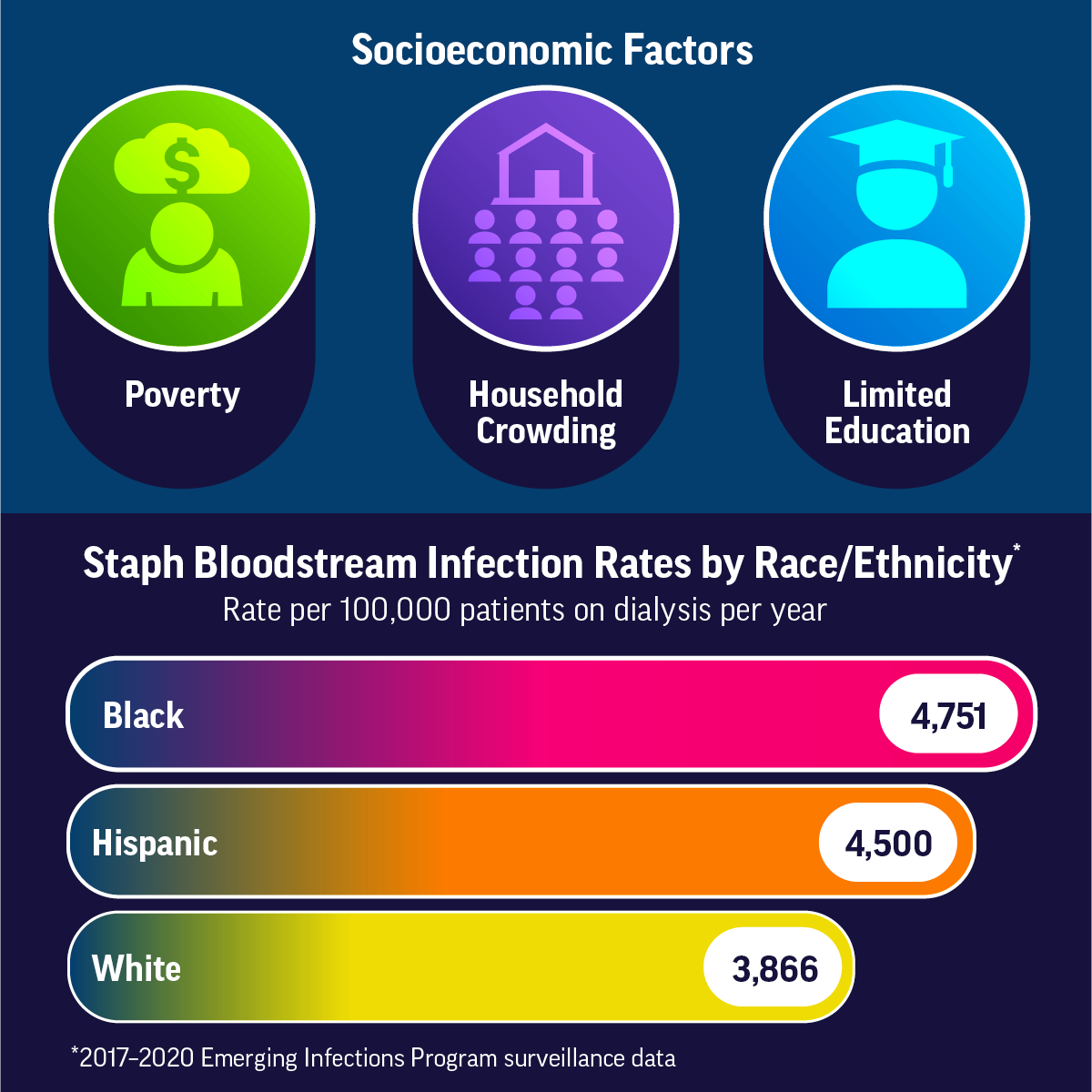
More than 14,000 bloodstream infections occurred in patients on dialysis in the U.S. in 2020, and more than one in three were caused by staph. The risk for staph bloodstream infection is strongly affected by how a person’s blood circulation is connected to the dialysis machine, known as vascular access type. Staph bloodstream infections happen more often in Black and Hispanic patients on dialysis than White patients on dialysis, although other factors besides race and ethnicity may be involved. There are more staph bloodstream infections in areas of the U.S. with higher poverty, more household crowding, and lower education levels (from U.S. census data).
The good news is that bloodstream infections in patients on dialysis have gone down since 2014 with the widespread use of proven practices to prevent and control infections. Preventing infections among patients receiving dialysis requires a broad and equitable approach to prevention and care of kidney disease for people from all racial, ethnic, and socioeconomic* groups, including:
- Encouraging practices that are known to prevent and slow the progression of chronic kidney disease.
- Increasing the use of vascular access types that are proven to be lower risk for infections, such as fistulas and grafts, for people starting and currently on dialysis.
- Continuing to apply proven practices to prevent and control infections in all U.S. dialysis facilities.
*A way of describing people often based on their level of education, income, place of residence, and job type.

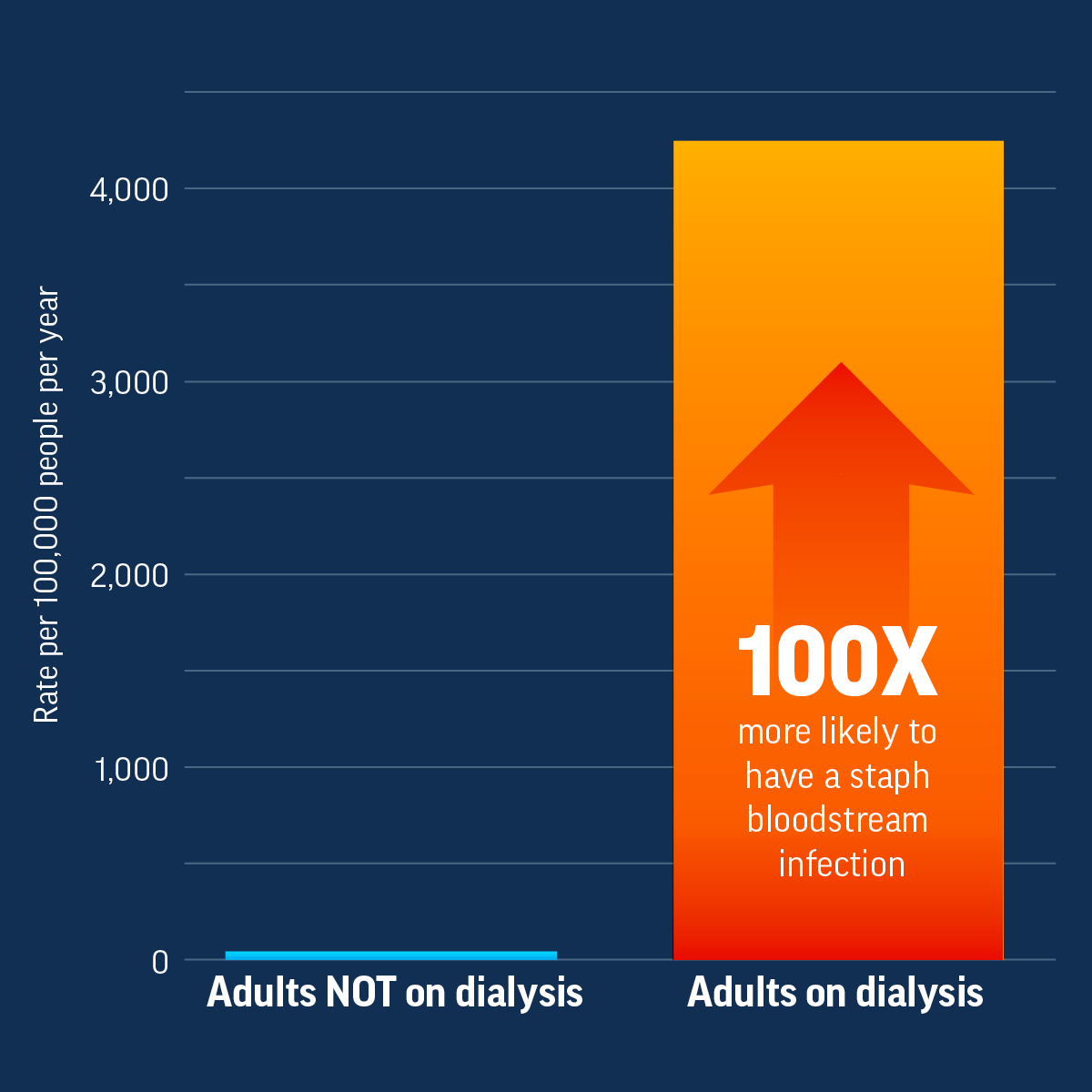
High risk for infection: Infections are common among patients on dialysis. These patients are more likely to get a staph bloodstream infection than people not on dialysis. Staph bloodstream infections can be serious or lead to death, and some infections are resistant to some of the most common antibiotics used to treat them, making the drugs ineffective.
Racial and ethnic gaps: End-stage kidney disease affects Black and Hispanic people more than White people. Black and Hispanic people have greater numbers of medical conditions, such as high blood pressure and diabetes, which increase their risk of developing end-stage kidney disease. There are also differences in the types of therapies and treatments that Black and Hispanic patients receive for end-stage kidney disease. In addition, more Black and Hispanic patients on dialysis get staph bloodstream infections than White patients on dialysis.
Social and economic factors: Lack of prevention and care of kidney disease, socioeconomic and insurance status, and lack of patient education about treatment options are all factors in end-stage kidney disease treatment differences.
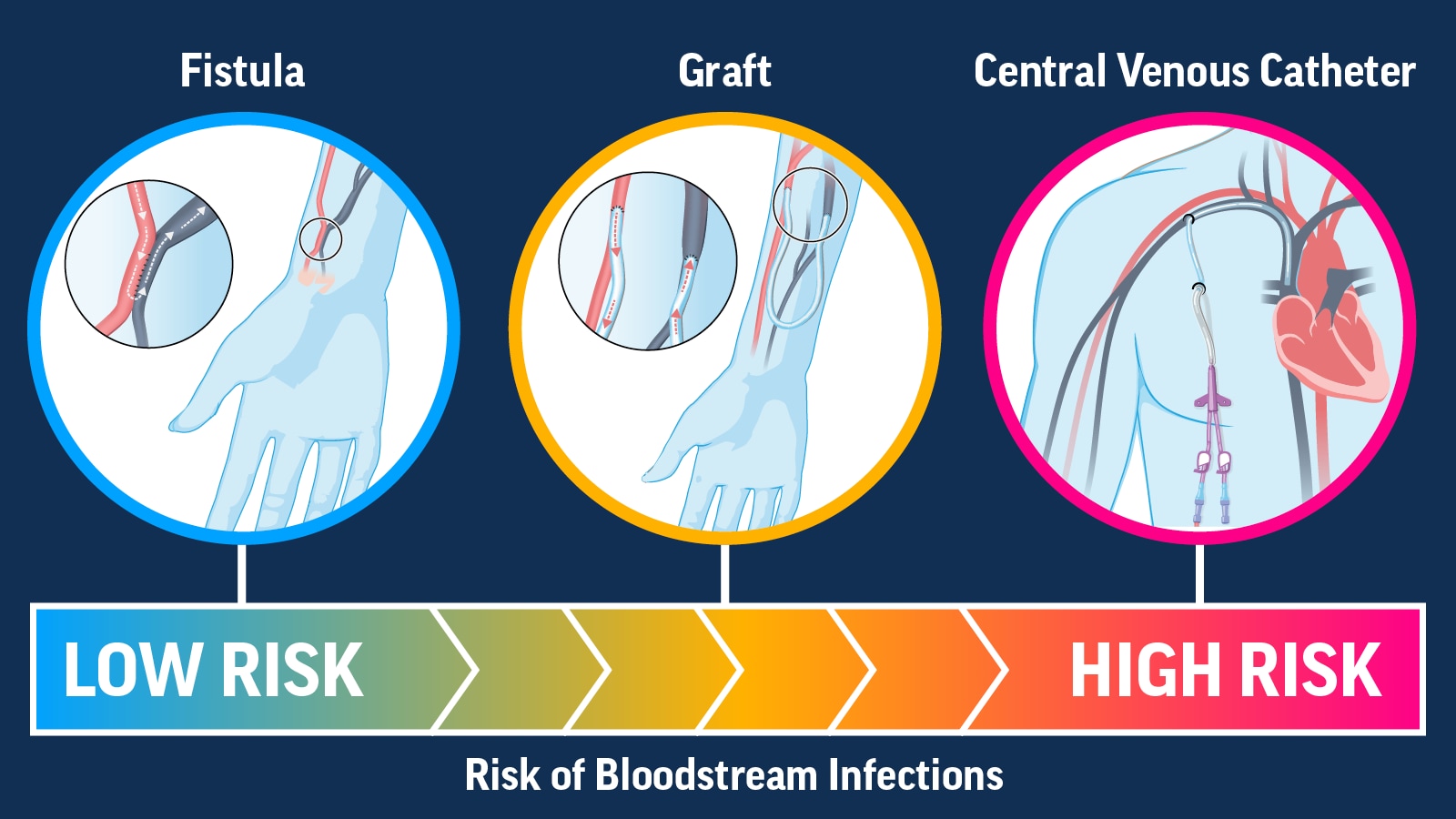
Catheter use: Vascular access type is the major risk factor for bloodstream infections regardless of race, ethnicity, or socioeconomic status. There are three access types: fistula, graft, and central venous catheter. People with any access type can develop an infection, but fistulas have the lowest risk of infection and central venous catheters have the highest risk of infection.
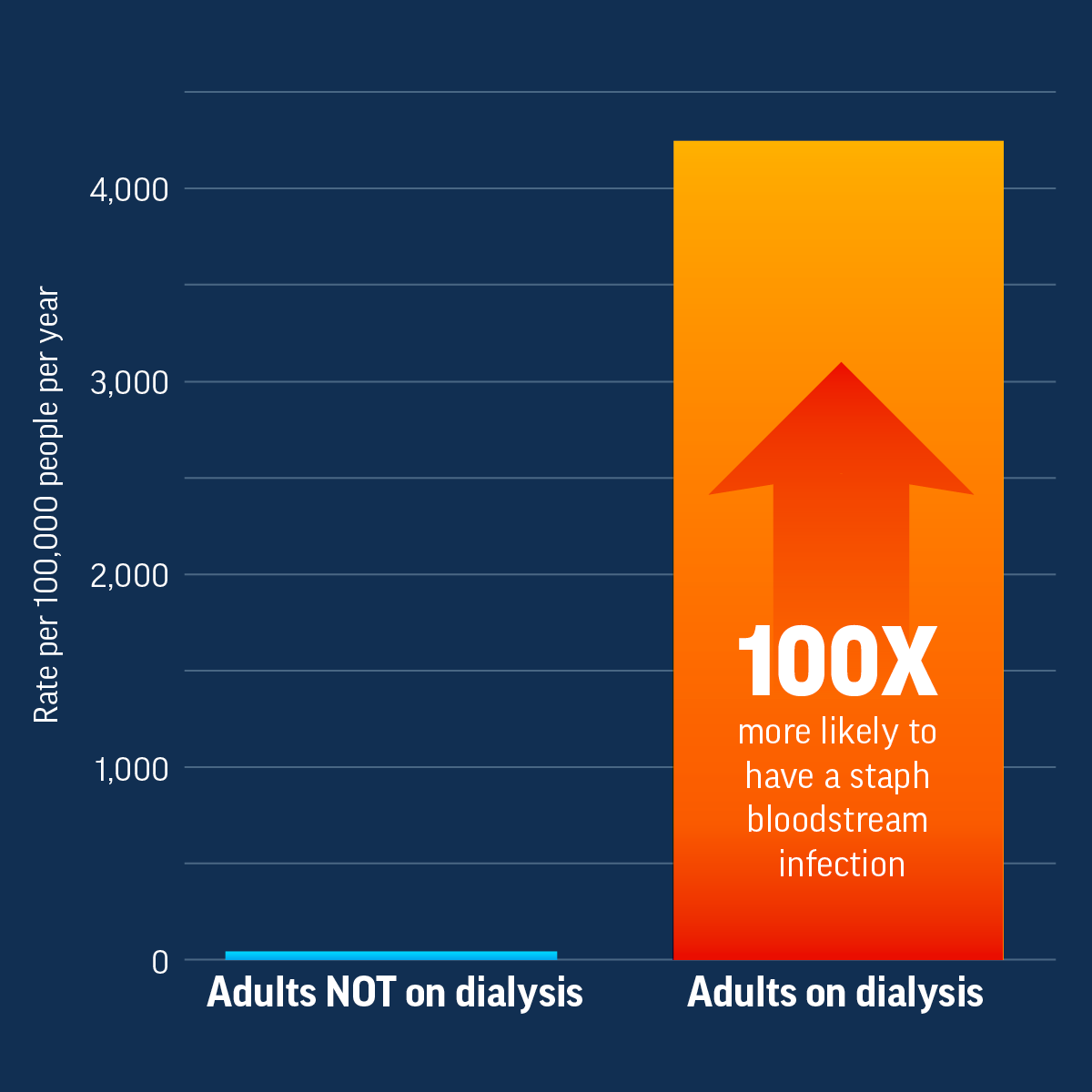
Adults on Dialysis Are More Likely to Have Staph Bloodstream Infections
Adults on dialysis are 100 times more likely to have a staph bloodstream infection than adults not on dialysis.
Inequities Can Lead to More Staph Bloodstream Infections
Race, ethnicity, and socioeconomic factors can lead to more dialysis bloodstream infections.
Adults on Dialysis Are More Likely to Have Staph Bloodstream Infections
Adults on dialysis are 100 times more likely to have a staph bloodstream infection than adults not on dialysis.
Inequities Can Lead to More Staph Bloodstream Infections
Race, ethnicity, and socioeconomic factors can lead to more dialysis bloodstream infections.
Increase Use of Lower-Risk Vascular Access Types for Dialysis
Reducing the use of central venous catheters for people on dialysis can help prevent bloodstream infections.
Bloodstream infections are preventable in all patients on dialysis. Actions by healthcare providers, dialysis providers, dialysis partner organizations, and public health professionals can help prevent these infections. Extra attention should be focused on people from groups experiencing racial, ethnic, and socioeconomic differences in staph bloodstream infections. Actions include:
- Promoting practices to prevent and manage chronic conditions like diabetes and high blood pressure and detecting and treating chronic kidney disease in its early stages to prevent the need for dialysis.
- Counseling patients on potential treatment options, in their preferred language, before they develop end-stage kidney disease.
- Coordinating efforts between patients, nephrologists, vascular access surgeons, radiologists, nurses, nurse practitioners, and social workers to reduce the use of central venous catheters for dialysis treatment.
- Educating and empowering patients with culturally appropriate resources to help prevent infections and understand infection risks of different access types, especially central venous catheters.
- Reducing barriers for patients receiving medical care by offering transportation assistance, insurance coverage expertise, social work services, and education resources in multiple languages.
Better information can lead to more effective infection prevention programs and catheter reduction policies that will benefit everyone on dialysis. More data about dialysis bloodstream infections in patients of different races, ethnicities, and socioeconomic statuses can be gained by:
- Improving monitoring for dialysis bloodstream infections that includes racial, ethnic, and socioeconomic factors, as well as patient vascular access types.
- Doing more studies to better understand racial, ethnic, and socioeconomic differences and how these impact people on dialysis.
Bloodstream infections are preventable in all patients on dialysis. Actions by healthcare providers, dialysis providers, dialysis partner organizations, and public health professionals can help prevent these infections. Extra attention should be focused on people from groups experiencing racial, ethnic, and socioeconomic differences in staph bloodstream infections. Actions include:
- Promoting practices to prevent and manage chronic conditions like diabetes and high blood pressure and detecting and treating chronic kidney disease in its early stages to prevent the need for dialysis.
- Counseling patients on potential treatment options, in their preferred language, before they develop end-stage kidney disease.
- Coordinating efforts between patients, nephrologists, vascular access surgeons, radiologists, nurses, nurse practitioners, and social workers to reduce the use of central venous catheters for dialysis treatment.
- Educating and empowering patients with culturally appropriate resources to help prevent infections and understand infection risks of different access types, especially central venous catheters.
- Reducing barriers for patients receiving medical care by offering transportation assistance, insurance coverage expertise, social work services, and education resources in multiple languages.
Better information can lead to more effective infection prevention programs and catheter reduction policies that will benefit everyone on dialysis. More data about dialysis bloodstream infections in patients of different races, ethnicities, and socioeconomic statuses can be gained by:
- Improving monitoring for dialysis bloodstream infections that includes racial, ethnic, and socioeconomic factors, as well as patient vascular access types.
- Doing more studies to better understand racial, ethnic, and socioeconomic differences and how these impact people on dialysis.
Use Proven Practices
- Follow CDC’s approach to bloodstream infection prevention in dialysis facilities, which has been shown to help reduce infections.
- Raise awareness and promote use of CDC audit tools and checklists for recommended infection prevention practices.
- Act fast if you suspect sepsis. Know sepsis signs and symptoms to identify and treat patients early.
Support Catheter Reduction
- Educate patients and staff about end-stage kidney disease therapies, including kidney transplant and vascular access options for dialysis, with culturally appropriate materials in their preferred language. When appropriate, refer patients to vascular access surgeons and assess patients for transplant suitability.
- Identify and address barriers to central venous catheter removal and placement of permanent vascular access types, such as fistulas and grafts.
- Promote education and partnership initiatives like the Making Dialysis Safer for Patients Coalition and the End Stage Renal Disease Network Program.
Everyone can:
- Prevent chronic kidney disease by managing diabetes and high blood pressure. Learn about chronic kidney disease and its risk factors.
- Read and share infection prevention resources for patients on dialysis.
- Clean your hands often with alcohol-based hand sanitizer or soap and water to prevent the spread of germs.
- Watch for signs of infection and its complications, like sepsis.
Get email updates about Vital Signs
VITAL SIGNS RESOURCES