What to know
- The Vaccines for Children (VFC) Program provides vaccines to children whose parents or guardians may not be able to afford them.
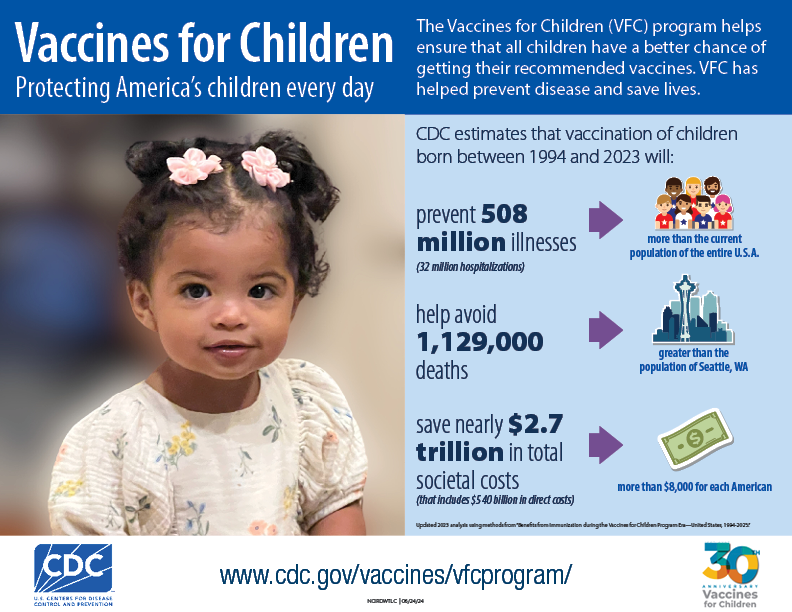
- Serving as one of the nation's most important contributors to vaccine access, the program helps ensure that all children eligible for VFC vaccines have a better chance of getting their recommended vaccinations on schedule and staying healthy.

History of the VFC Program
In 1989 – 1991, a measles epidemic in the United States resulted in tens of thousands of cases of measles and hundreds of deaths. When this epidemic was investigated, the Centers for Disease Control and Prevention (CDC) found that more than half of the children who had measles had not been vaccinated against measles, even though many of them had seen a healthcare provider.123 Cost of the vaccine was found to be a primary reason for children going unvaccinated even in families with a regular health care provider.
In response to this measles epidemic, Congress passed the Omnibus Budget Reconciliation Act (OBRA) on August 10, 1993, creating the VFC Program. The VFC Program became operational October 1, 1994. Known as Section 1928 of the Social Security Act, the Vaccines for Children Program is an entitlement program (a right granted by law) for eligible children, ages 18 and younger. The program was an unprecedented approach to improving vaccine availability nationwide by providing vaccine at no cost to VFC Program-eligible children through VFC Program enrolled public and private health care providers.
How the VFC Program is funded
The Office of Management and Budget (OMB) approves funding for the VFC Program, then allocates the funds through the Centers for Medicare & Medicaid Services (CMS) to CDC. After receiving the funds, CDC buys the vaccines at a discount and distributes them to VFC Program providers at the direction of award recipients (i.e., the 63 state, local, and territorial immunization programs who receive operational funding from the CDC to implement and oversee their VFC Programs). The legislation for the VFC Program provides general guidance for VFC Program policy development—including eligibility, provider recruitment, and considerations for negotiating contracts with manufacturers.
The VFC Program benefits the nation
The goal of the VFC Program is to ensure that a VFC Program-eligible child can access recommended vaccines regardless of their parent or guardian’s ability to pay. The VFC Program supports improved immunization coverage levels among eligible children by:
- Providing free vaccines:
- Automatically covers vaccines recommended by the Advisory Committee on Immunization Practices (ACIP) and approved by the CDC, which includes vaccines for children ages 18 years and younger
- VFC Program-provided vaccines protect against 18 different diseases
- Saving money:
- Provides publicly purchased vaccines for eligible children at no charge to VFC Program-enrolled providers in all states and U.S. territories
- Eliminates or reduces vaccine cost to parents or guardians
- Minimizing barriers to vaccination:
- Reduces disparities in child vaccination rates, ensuring that any child can access recommended vaccines regardless of income or geography
- Allows eligible children to be vaccinated in their regular healthcare provider, reducing the need for referral to health departments
- Eliminates cost to the parents or guardians as a barrier to vaccinating children
- Improving private-public collaboration:
- Allows enrolled private providers to receive publicly purchased vaccine
- Promotes coordination between community and private sector partners and public agencies—including state health departments, state Medicaid programs, and programs serving families and children—to recruit and retain a network of VFC Program providers
- CDC. Measles – United States, First 26 Weeks, 1989.MMWR 1989; 38(50): 863-866,871-872
- CDC. Current Trends Measles – United States, 1989 and First 20 Weeks 1990. MMWR 1990; 39(21): 353-355,361-363
- CDC. Current Trends Measles – United States, 1990. MMWR 1991; 40(22): 369-372