Key points
- CDC's Pediatric Mild Traumatic Brain Injury (mTBI) Guideline Checklist is for healthcare providers treating children 18 years of age and younger.
- There are 3 main steps: Assess, Counsel, and Refer.
CDC Pediatric Mild TBI Guideline Checklist
Conduct a physical examination to identify findings that:
- Suggest more severe TBI (such as hemotympanum, pupillary asymmetry).
- May impact management of mTBI (such as concurrent injuries or baseline deficits, oculomotor dysfunction).
- Suggest other contributions to symptoms (such as dehydration, cervical tenderness, scalp hematoma).
Do not image routinely (including CT & MRI).
- Use validated clinical decision rules predicting risk for more severe injury to determine need.
A combination of risk factors that may indicate need for neuroimaging include:
- Age < 2 years old
- Recurrent vomiting
- Loss of consciousness
- Severe mechanism of injury
- Severe or worsening headache
- Amnesia
- Non-frontal scalp hematoma
- Glasgow Coma Score < 15
- Clinical suspicion for skull fracture
Assess symptoms using validated scales. Consider cognitive and balance testing.
Examples of validated scales include, but aren't limited to:
- Post-Concussion Symptom Scale
- Health and Behavior Inventory
- Post-Concussion Symptom Inventory
- Acute Concussion Evaluation
Conduct a history to identify risk factors for poor prognosis using validated prediction rules.
Factors associated with poor prognosis:
- Older age (older children/adolescents) or Hispanic ethnicity
- Lower socio-economic status
- History of intracranial injury
- Premorbid histories of mTBI or increased pre-injury symptoms
- Neurological or psychiatric disorder
- Learning difficulties or lower cognitive ability
- Family and social stressors
Provide information about:
- Warning signs that injury may be more serious
- A headache that gets worse and does not go away
- Significant nausea or repeated vomiting
- Increased confusion, restlessness, or agitation
- Slurred speech, drowsiness, or inability to wake up
- Weakness, numbness, or decreased coordination
- Loss of consciousness, convulsions, or seizures
- Typical recovery course.
- How to prevent further injury.
- Gradual re-introduction of activity that does not significantly worsen symptoms.
- The need for social and emotional support.
Offer clear instructions (preferably verbal and written) on return to activity, including school and sports, customized to the patient's symptoms.
- After 1 to 2 days of rest, begin light activity & then gradually re-introduce regular activities (not inclusive of sports) that do not significantly worsen symptoms.
- Assess school-related needs & monitor progress in collaboration with parents and school professionals.
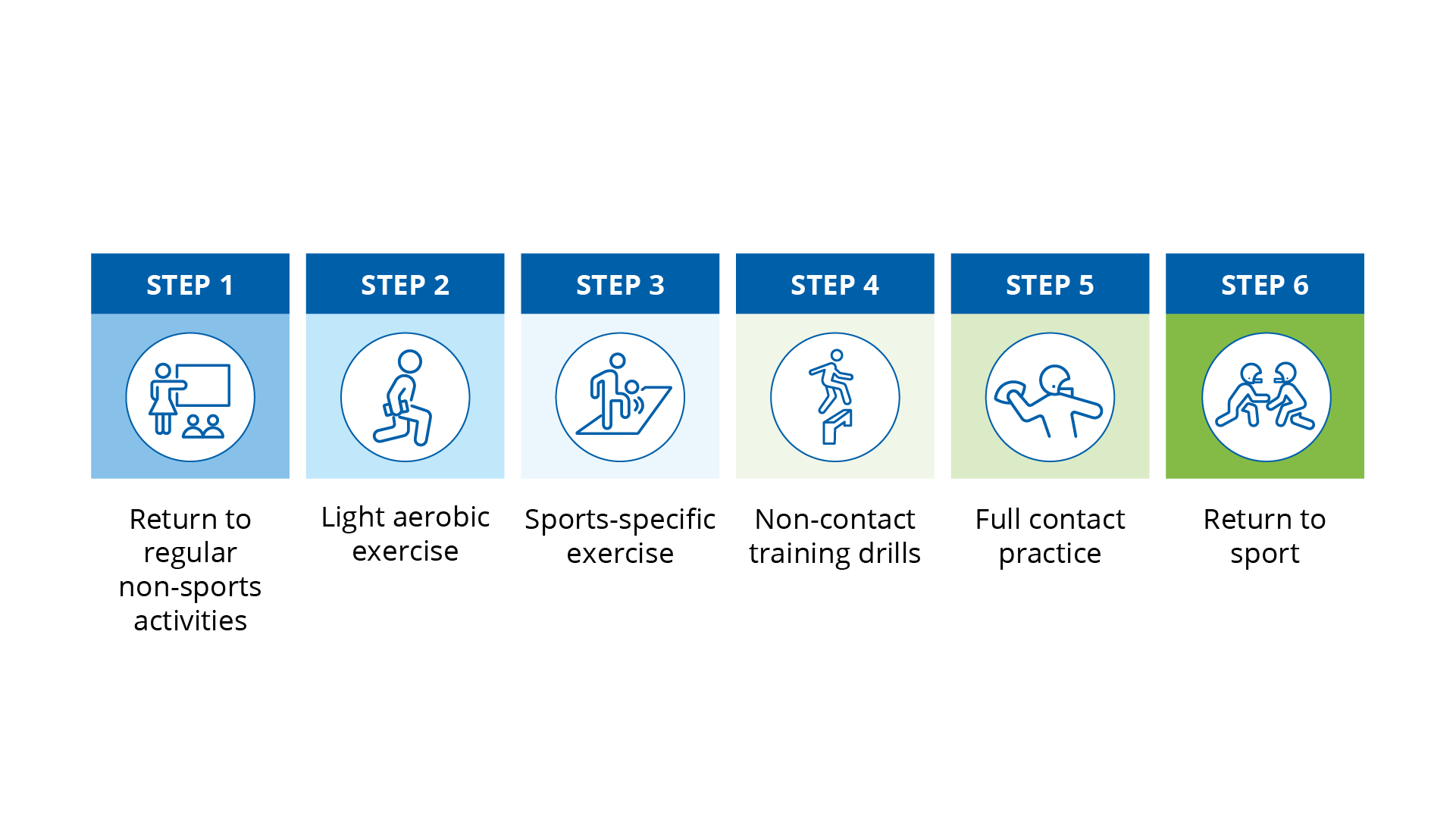
- Once back to regular non-sports activities (including school), patient can begin return to sports using a standard progression with gradually increasing levels of physical exertion.
- No return to contact sports activity until symptom-free with exertion (including without the use of pain medication).
Refer patients whose symptoms do not resolve as expected with standard care after 2 to 4 weeks. In some cases, access to specialists may be limited due to required travel distance or other limitations. In these cases, consider whether telemedicine or telehealth services are possible to connect patients with specialists, depending on the need.
Symptom and recommendation
Acutely worsening symptoms
- Consider neuroimaging
Chronic headache
- Non-opioid analgesia (monitor for overuse), multi-disciplinary evaluation
Vestibulo-ocular dysfunction
- Vestibular rehabilitation
Worsening sleep problem
- Sleep hygiene, sleep specialist
Cognitive impairment
- Treatment directed at etiology, neuropsychological evaluation
Emotional dysfunction
- Psychotherapeutic evaluation and treatment