
Study Syllabus for Classification of Radiographs of Pneumoconioses
Pathology Overview
Pathology Basis of Occupational Lung Disease
Pathologic–Radiological Correlations
Silica and Coal Dust
Although the chest radiograph is an excellent method for assessing the degree of involvement of the lung in CWP and silicosis, certain limitations are recognized. Individual lesions less than 3 mm in maximal dimension usually cannot be visualized radiographically. Therefore, in early macular CWP or nodular silicosis the chest radiograph may appear as “normal.” Radiologic summation effect due to the superimposition of numerous small nodules may nonetheless result in the appearance of small round opacities [“Pathology standards,” 1979]. The ILO system serves as a means of classifying chest radiographs of individuals with pneumoconiosis. It does not define pathologic entities. The distinction between CWP and silicosis by chest radiography alone is usually not possible. Nodular lesions of simple CWP and simple silicosis appear as rounded opacities measuring up to 1 cm in diameter on a chest radiograph [“Pathology standards,” 1979]. Small irregular opacities are less frequent. Lesions of complicated pneumoconiosis are represented radiographically by large opacities that exceed 10 mm in the longest dimension.
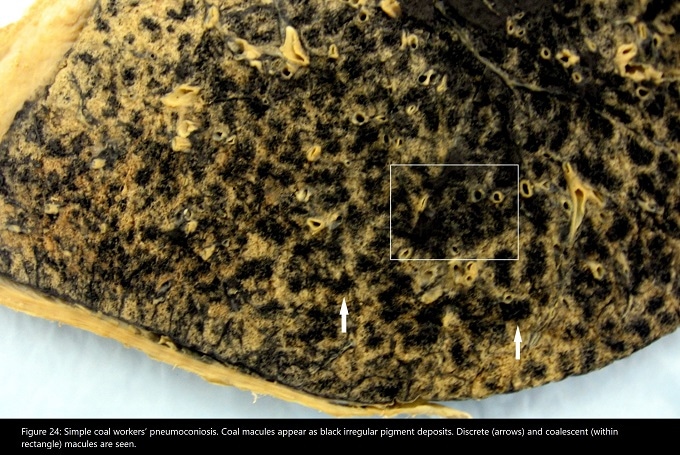
Studies correlating lung pathology with ILO Classification in CWP have shown that small p-type opacities correlate with dust macules and emphysema (Fig. 24), (Fig. 25). Larger q- and r-type opacities are seen as fibrotic nodular lesions [Green and Vallyathan 1998; Vallyathan et al. 1996; Ruckley et al. 1984a]. Type q opacities have been associated with nodular lesions measuring from 1 to 7 mm, while r-type opacities correlate with macronodules measuring from 7 to 10 mm [Vallyathan 1996]. Ruckley et al correlated stellate nodules (Fig. 21) with q-type opacities and round silicotic-type nodules with r-type opacities [Ruckley et al. 1984a] (Fig. 26). There is also a positive correlation between mean weight of retained lung dust and radiographic profusion score for small round opacities in CWP [Ruckley et al. 1984a]. Small irregular opacities in coal workers are somewhat less frequent than rounded opacities and have been associated with emphysema and/or pigment-laden interstitial fibrosis [Ruckley et al. 1984a; Lyons et al. 1974]. (Fig. 31)
{kind=link}
In patients with rapidly progressive pneumoconiosis, features of silicosis were significantly associated with rounded (p, q, r) opacities on chest imaging, while high-grade interstitial fibrosis was associated with the presence of irregular (s, t, u) opacities [Cohen et al. 2016].