About
The NIOSH Strategic Plan reports NIOSH's research and service goals for fiscal years (FY) 2019–2026.
Overview
The NIOSH Strategic Plan reports the Institute's research and service goals for fiscal years (FY) 2019–2026. These goals address a wide range of occupational health and safety hazards, affecting a workforce that constantly changes.
Jobs in the U.S. economy continue to shift from manufacturing to services. They also have longer hours and reduced job security, alongside an aging workforce. These issues are a major challenge for NIOSH's limited resources for research priorities.
NIOSH recognizes that new issues may emerge or become more important during the plan's timeframe. We may retire goals that we have achieved. We may also shift our priorities in response to changing conditions.
NIOSH will give funding priority to extramural research applications that clearly identify the strategic and intermediate goals their proposed work will address or support.
Plan development
NIOSH chose to use three levels of goals: strategic, intermediate and activity. Research and service program staff wrote goals collaboratively using the Burden, Need, and Impact Method. They considered a variety of information to choose priorities, such as surveillance data, partner input, and legislative requirements.
Research and service activities are considered separately in the plan because they operate differently.
Research programs
NIOSH has a portfolio of research programs, organized according to the National Occupational Research Agenda (NORA) framework.
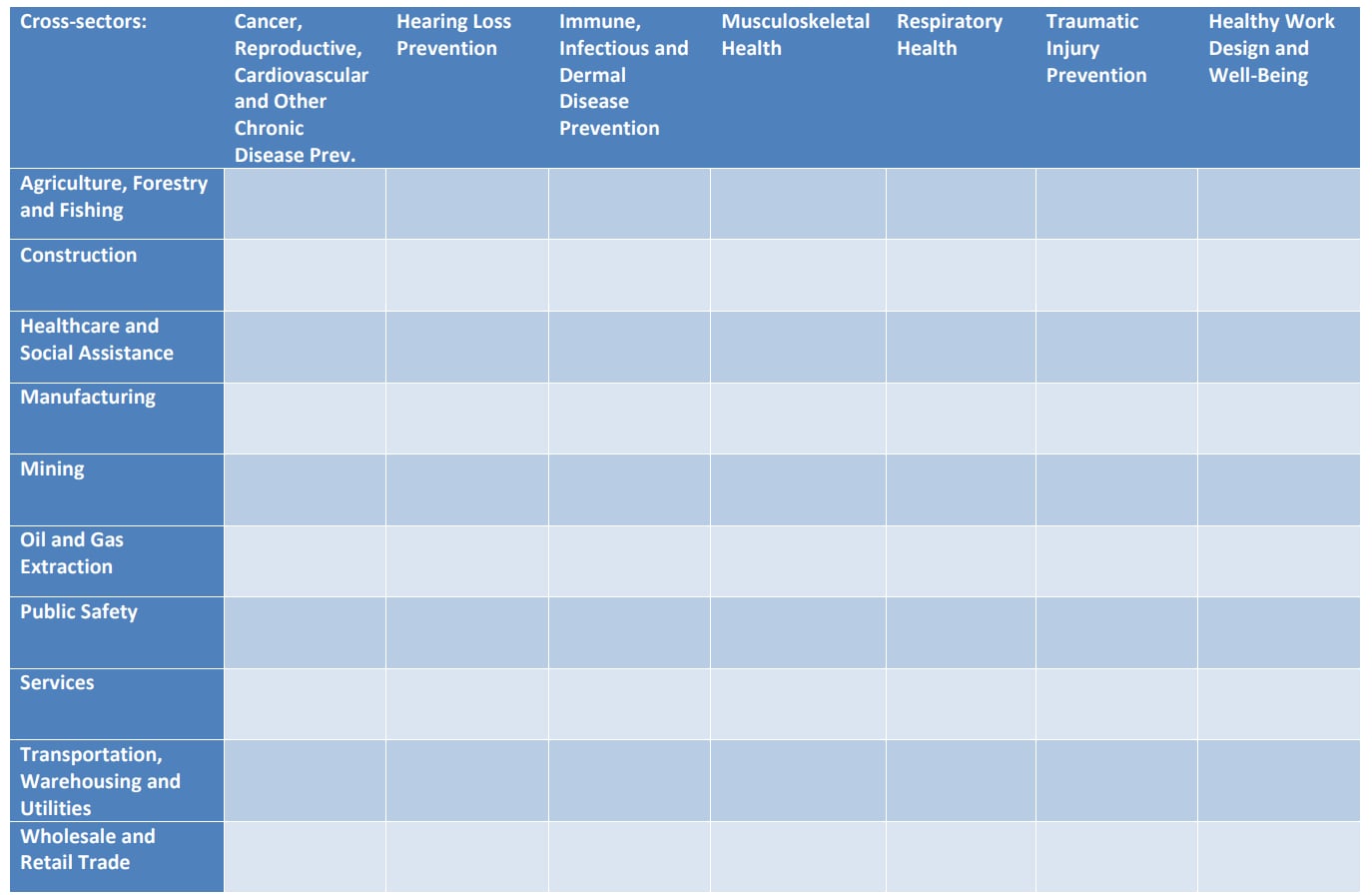
NIOSH's 10 sector programs focus on industrial sectors. Seven cross-sectors programs focus on the major health and safety issues affecting the US working population. They form a program grid infused with core and specialty programs representing:
- Core activities
- Mandates
- Special emphasis areas
- Methodological approaches
These programs cover a wide range of activities, from basic to applied research.
Research goals
NIOSH established seven strategic goals that best represent the health and safety issues facing the U.S. workforce:
- Reduce occupational cancer, cardiovascular disease, adverse reproductive outcomes, and other chronic diseases.
- Reduce occupational hearing loss.
- Reduce occupational immune, infectious, and dermal disease.
- Reduce occupational musculoskeletal disorders.
- Reduce occupational respiratory disease.
- Improve workplace safety to reduce traumatic injuries.
- Promote safe and healthy work design and well-being.
Strategic goals are supported by intermediate and activity goals:
- Intermediate goals describe actions organizations and individuals would ideally take using NIOSH research findings or products.
- Activity goals describe research activity that moves the research through the research to practice continuum.
Service activities
Service activities contribute to the NIOSH mission by:
- Providing a service to individuals and organizations outside of NIOSH,
- Support internally to NIOSH staff, or
- A combination of the two.
Some services are mandated by law.
Services can support a single sector or cross-sector. For example, the Coal Workers' Health Surveillance Program benefits the mining sector. Services can also support multiples sectors or cross-sectors. For example, Fatality Assessment and Control Evaluation (FACE) investigates fatalities in a wide range of industries with a variety of causes.
NIOSH's service work includes, but is not limited to:
- Respirator approvals
- Health Hazard Evaluations (HHE)
- Radiation dose reconstruction
- Emergency preparedness and response activities
- Coal Workers' Health Surveillance Program activities
Service goals
Service activities also use three levels of goals:
- Strategic goals are broad in scope. These are the same seven strategic goals used same research programs.
- Intermediate goals identify improvements and maintenance of service activities. These allow organizations or individuals to take action more easily.
- Activity goals are statements of activities that improve or maintain the timeliness, relevance, and quality of services.