At a glance
Scenario models are a type of disease model that explore hypothetical outcomes under different assumptions about the future. Scenario models do not aim to predict the future, but rather allow us to explore “what-if” hypothetical situations. CDC uses a scenario model as part of CFA’s Respiratory Season Outlook to explore potential COVID-19 scenarios over the course of several months. We describe the key features of this model here.
COVID-19 scenario modeling overview
Scenario models are a type of disease model that explore medium- to long-term hypothetical outcomes under different assumptions about the future. Unlike forecasts produced for the short-term future, scenario models do not aim to predict the future; instead, they allow us to explore "what-if" hypothetical situations. By exploring potential scenarios, decision-makers can better prepare and plan for an uncertain future. Our Behind the Model shares more about how scenario modeling can be used to inform decision-making. In this document, we focus on scenario models produced by CFA, which are submitted to the Scenario Modeling Hub and used in CFA's Respiratory Season Outlooks. Research or operational questions determine the focus for each round of scenario modeling from the Scenario Modeling Hub; previous rounds have focused on the impact of changes in behavior, vaccination, and the introduction of new variants. Specific scenarios defined for the Respiratory Season Outlooks also vary by the respiratory season, but have focused on peak timing and size, and variant emergence.
We project COVID-19 dynamics under different scenarios using a transmission model with a compartmental structure that takes into account population age structure, infection history, vaccination history, immunity waning status, and SARS-CoV-2 variants. Immunity is determined by immunogenic events (infections and vaccinations) and time since the most recent event. Protection against infection is variant-specific: past infection with a more similar variant, or vaccination with a better-matched vaccine, provides a higher level of protection against the challenging variant. The model uses mathematical equations, implemented in computer code, to describe how groups move between compartments (e.g., from uninfected to infected or from unvaccinated to vaccinated).
2026 Summer COVID-19 Outlook
Detailed model structure
The COVID-19 model used for the 2026 Summer Outlook is a Susceptible, Exposed, Infectious, Susceptible (SEIS) model, which models the movement between the population states Susceptible, Exposed, Infectious, and back to Susceptible. Each compartment is stratified by several factors, or dimensions: age group, vaccination status, infecting variant, and immunity levels, which wane over time and are boosted by vaccination and infection. The categories within each dimension (e.g., not vaccinated, one dose of vaccination, etc.) are shown in Table 1.
Table 1: Table showing the stratifying features (dimensions) for the SEIS COVID-19 model used in the Summer 2026 COVID-19 Outlook and the specific categories within each dimension.
| Dimension | Category |
|---|---|
| Vaccination Status |
|
| Age (years) |
|
| Modeled strains |
|
|
Immunity waning
(Susceptible compartment only) |
|
|
1 The definition of "season" here is October through mid-May to align with the Respiratory Disease Season Outlook. The seasonally vaccinated category is mutually exclusive to the other vaccination categories.
2 Using empirical data for historical vaccination and sero-prevalence, we initialized our model starting on February 11, 2022, with BA.1 being the dominant variant at that time.
|
|
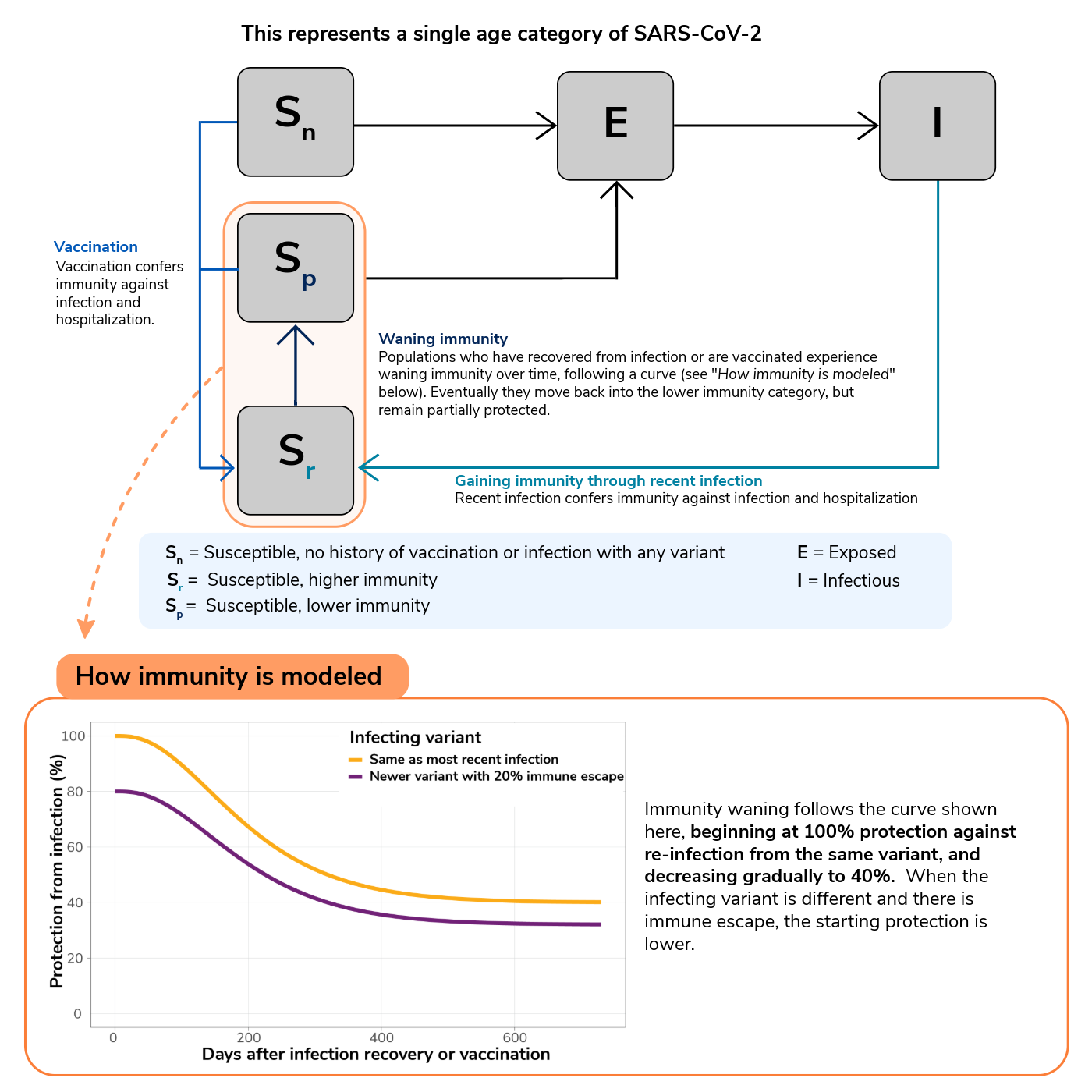
To illustrate this structure, let's consider a single age group and SARS-CoV-2 variant (Figure 1). Populations who are susceptible to infection and have no vaccination or recent infection (and therefore immunity) are treated as a single group (Sn). When they are infected but not yet infectious, they move to the exposed compartment (E). When they become infectious, they move into the infectious compartment (I). Following a period of infectiousness, they then return to being susceptible but move to a higher immunity compartment due to their recent infection (Sr). They then could be re-infected and move into the exposed compartment or, in the absence of a new infection and as immunity wanes, they will return to the lower-immunity category but retain partial immunity (Sp). This structure occurs for each age group and SARS-CoV-2 variant. These structures are interconnected: people across different age groups are mixing, allowing for transmission across age-groups.
Newly introduced variants have immune-escape properties that may allow them to spread in a population that is highly immune to previous variants. The introduction of a particular SARS-CoV-2 variant is determined by parameters defining the introduction time. These parameters are estimated for historical variants, and the distributions of those estimates are used to inform scenarios for future potential variants.
Immunity
Upon recovery or vaccination, people are placed at the high immunity status regardless of their previous immunity status. By representing immunity as people “flowing” between these high and low states of partial protection, we approximate population-level immunity that changes smoothly over time (Figure 1 and 2). For re-exposures to the same variant that caused the most recent infection, we assume high immunity status confers 100% protection from infection; this protection wanes to 40% for low immunity status. The half-life of this protection, or amount of time for people to decrease from 100% protection to 70%, is approximately 188 days. When challenged with newer variants with, for example, 20% immune escape, the high immunity status confers only 80% protection from infection and eventually wanes to 32% protection. These assumptions imply an immunity waning profile as shown in the bottom panel of Figure 1.
Hospitalization rate modeling
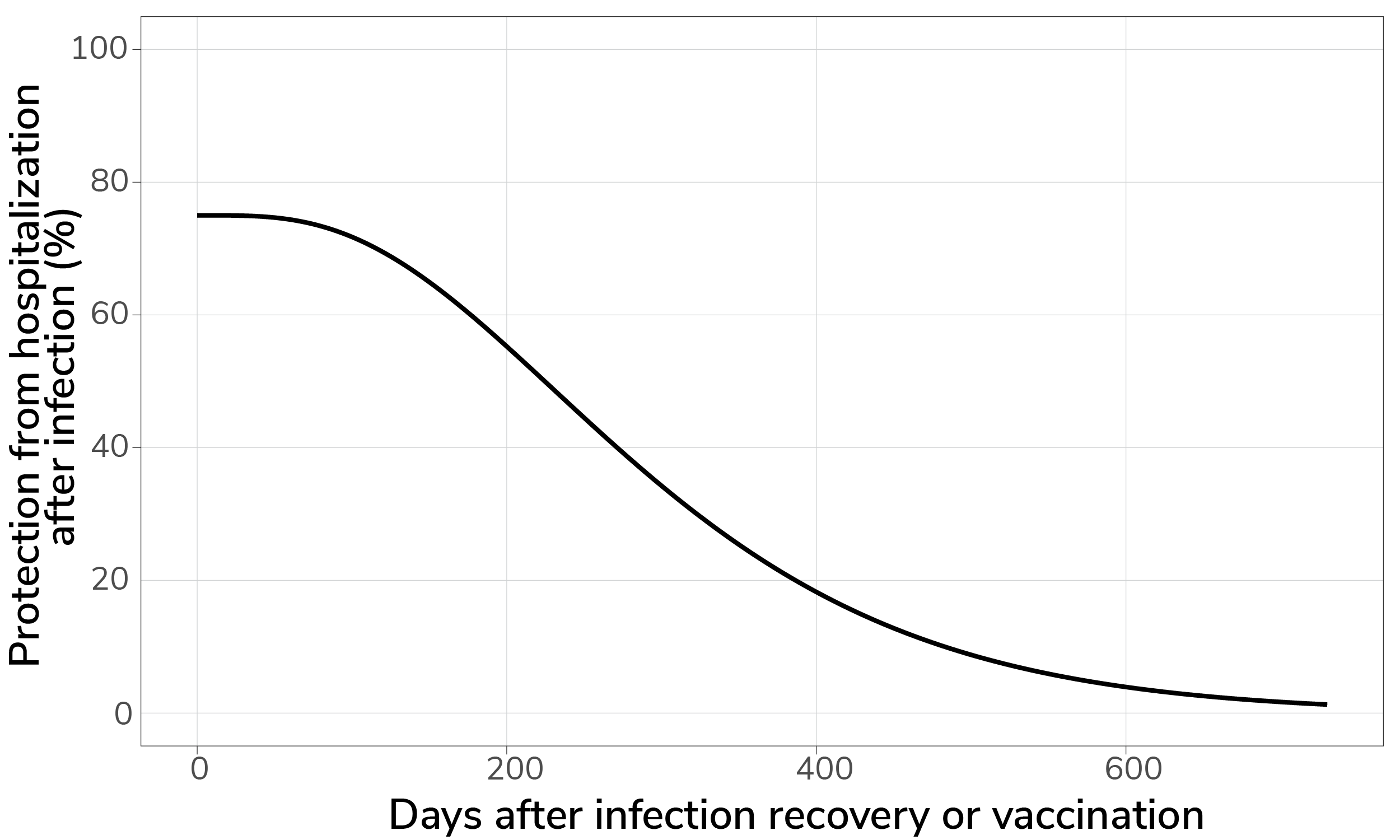
Our model estimates hospitalizations from infections using infection-hospitalization ratios (IHRs). These ratios represent the proportion of infections that result in reported hospitalizations. In our model, infection-hospitalization ratios vary by age group and are influenced by immunity (as discussed in previous section). We assume that people who have recovered from a past infection or received vaccination have a reduced IHR when reinfected and that this benefit is stronger when the immunizing event was recent. This protection factor is estimated by the model to start around 75% and wanes over time (Figure 2). The waning rate is assumed to be slower than that of protection from infection. Because the primary effect of vaccination in the model is refreshing existing immunity, vaccine effectiveness against hospitalization is more appropriately thought of as an output of the model, rather than an input.
We also assume that more recent variants, starting with JN.1 (Winter 2023), are associated with a lower IHR than variants prior to JN.1. We multiply the estimated hospitalization risks to modeled daily infections to generate daily hospitalizations by age group, using a one-week lag between infection and hospitalization. These daily estimates are then aggregated into weekly totals to generate state-level hospitalization projections across the United States. This approach does not consider hospital capacity or occupancy and assumes that hospitalization does not have a substantial effect on transmission.
Parameter fitting
The COVID-19 model is calibrated to hospitalization data for each U.S. state. For the 2026 COVID-19 Summer Outlook, we used National Healthcare Safety Network (NHSN) hospitalization rate data for the state of Wyoming. For all other states, NHSN data were used prior to April 2024, and projected hospitalization rates inferred from National Syndromic Surveillance Program emergency department visit data were used between April 2024 and either May 2025 (Pennsylvania and Arizona) or Dec 21, 2024 (all other states). This was due to gaps in hospitalization data reporting from NHSN. To infer hospitalization rates from NSSP emergency department visit data, weekly data from April 20, 2023 through April 20, 2024 were used to train four candidate models: a linear model, a linear model with a one-week lag, a generalized additive model, and a generalized additive model with a one-week lag. The best-fitting model was selected separately for each state and age group and used to generate NSSP-inferred hospitalization estimates. Model fitting was carried out by calibrating model-produced hospitalization counts to observed hospitalization counts using an SVI (Stochastic Variational Inference) approach. See Table 2 for key parameters, values, and any references for fixed values.
Table 2: Key parameters, their values and sources for the values for the COVID-19 model
| Parameter | Value | Description | Reference (fixed parameters only) |
|---|---|---|---|
| R0 | Fitted. All variants since winter 2023 are assumed to have the same R0. | Basic reproductive number, or the expected number of secondary infections resulting from each infection, in the absence of control measures. | |
| Latent period | Fixed3 at 2 days for all variants | The time between infection and symptom onset | |
| Infectious period | Fixed4 at 4 days for all variants. This value is in the middle of the range of reported values for the infectious period of COVID-19. | The period of time during which an infected individual is able to infect others | |
| Vaccine coverage | Used age-stratified estimates provided by CDC. The national average was assumed to be the same as 2024-25: 12.8% for under 0-17 years old, 14.1% for 18-49, 24.8% for 50-64 and 44.6% for 65 and above. | The percentage of eligible individuals who receive a vaccination | CDC |
| Seasonality | Assumed to be a bimodal annual curve; parameters are fitted | Function that modifies the transmission rate according to season, with several independently fitted parameters | |
| Immune waning time | Mean of 210 days. Waning curve fitted to BNT162b2 vaccine effectiveness over time. | Waiting time to pass from high to low immunity state, follows a waning curve. | Tartof et al., 2021 |
| Protection against infection |
|
Level of protection against infection by immunity category | |
| Immunity modifiers from past infections with other variants | Calculated as 100% minus the level of immune escape of the newer variant. Level of immune escape is fitted within the model. | Level of protection due to recent past infection with other variants | |
|
3 Due to the model being a system of ordinary differential equations (ODE), this value represents the rate of movement between exposed and infectious compartments which results in a mean incubation period of 2 days. This value is fixed but represents a population mean.
4 Due to the model being a system of ordinary differential equations (ODE), this value represents the rate of movement between infectious and recovered compartments which results in a mean infectious period of 4 days. This value is fixed but represents a population mean.
|
|||
Scenarios
The following two scenarios were modeled for the Summer Respiratory Outlook 2026:
- No emergence of a new variant with significant immune-escape properties: Assumes that no variant will emerge that significantly evades the population's immunity.
- Emergence of a variant with moderate immune-escape properties in between June and September: People in the model experience a small risk of exposure to the new variant from an outside source that increases gradually over two weeks, peaks on a randomly chosen day between the middle of June to middle of September, and then decreases over two weeks. This exposure risk seeds infections that can then propagate via transmission within the population. We assumed that this variant had similar properties to the variants that were dominant during the winter 2024-25 wave, but the risk of hospitalization if infected was reduced at random between 0% and 30% across simulations.
Because most vaccinations for COVID-19 occur in the fall and winter, we did not consider different vaccination scenarios for the summer outlook. Both scenarios assumed vaccinations would occur beginning in fall 2026, at the same rates that were observed for fall 2025. In the scenario in which a variant with moderate immune escape properties emerges, variant-specific parameters were defined by sampling from the national distributions of variant-specific parameters for the last important variants. For each parameter, we sample from a normal distribution with the national median (pooling all 50 states together) as mean, and the average of state-level variances as variance. We produced forward projections for each state and scenario and then aggregated the state-level output to produce national projections.
2025-2026 Respiratory Disease Season Outlook
The scenario model used to produce the 2025-2026 Respiratory Disease Season Outlook is very similar to the structure described above. However, there are several differences:
- Immune protection against hospitalization: The immune protection against hospitalization if infected has a different pattern of waning over time since infection recovery/vaccination. In the version of the model used for the 2025-2026 Outlook, this protection factor is estimated by the model to start around 75% and follows the same waning profile as protection from infection (Figure 2). Because the primary effect of vaccination in the model is refreshing existing immunity, vaccine effectiveness against hospitalization is an output of the model. The model has an implied population-wide relative vaccine effectiveness against hospitalization of 40%, on average, over the 2025-26 respiratory virus season.

- Model calibration to historical hospitalization rate data: For 49/50 states, for the 2025-2026 Respiratory Disease Season Outlook used NHSN hospitalization data up to April 2024, and inferred hospitalization rates from emergency department visits from the National Syndromic Surveillance Program (NSSP) after April 2024 to calibrate the model (due to previous gaps in hospitalization data reporting from NHSN). NHSN was used for calibration for one state (Wyoming) due to unreliable NSSP data. The updated 2026 Summer COVID-19 Outlook uses NSSP data for calibration only between April 2024 and December 2024 for 47/50 states, with NSSP used up to May 2025 for two states (Pennsylvania and Arizona). This change was due to divergences in the relationship between hospitalization rates and ED visit data.
- R0 across variants: In the model used for the 2025-2026 Outlook, R0 is estimated from data, but not allowed to vary across variants from winter 2022 onwards. In the version used for the 2026 Summer Outlook, this restriction is only applied to strains from winter 2023 onwards (i.e., JN1 and XEC/XFG).
- Infectious period and latent period: In the model used for the 2025-2026 Outlook, infectious period was assumed to be 7 days, and in the most recent model it is assumed to be 4 days. In the model used for the 2025-2026 Outlook, the latent period was assumed to be 3.6 days. This has been decreased to 2 days for the 2026 Summer Outlook. The motivation behind this change is that previous parameter choices led to generation times which were longer than those recently reported in the literature. This change scales down both the latent period and infectious period to correct this.
- Scenarios: The following two scenarios were modeled for the 2025-2026 Outlook:
- No emergence of a new variant with significant immune-escape properties: Assumes that no variant will emerge that significantly evades the population's immunity.
- Emergence of a variant with moderate immune-escape properties in November: People in the model experience a small risk of exposure to the new variant from an outside source that increases gradually over two weeks, peaks on November 1, and then decreases over two weeks. This exposure risk seeds infections that can then propagate via transmission within the population. We assumed that this variant had similar properties to the variants that were dominant during the summer 2024 and winter 2024-25 wave, but the risk of hospitalization if infected was reduced at random between 0% and 30% across simulations.
Both scenarios assumed that only people 65+ and those with underlying health conditions would receive a COVID-19 vaccine in the 2025-2026 season. In the model, the 65+ age group received vaccines at the same rate as in 2024-2025. A proportion of 18- to 64-year-olds equivalent to the proportion of the population with relevant underlying conditions ("high-risk" groups) also received vaccination at the same rate as in 2024-2025. We also assumed vaccine effectiveness against infection was the same as in 2024-2025. In the scenario in which a November variant with moderate immune escape properties emerges, variant-specific parameters were defined by sampling from the posterior distributions of variant-specific parameters for the last two important variants (the posterior distributions for immune protection in the previous two waves had mean estimates of 72.4% (SD 4.1%) and 83.1% (SD 2.6%), respectively). We then combined these samples, fit a new multi-variate Gaussian distribution to the combined samples, and then sampled from the new distribution to produce the parameters for the new variant. We produced forward projections for each state and scenario and then aggregated the state-level output to produce national projections.