Key points
- Omphalocele (uhm-fa-lo-seal) is a birth defect of the abdominal (belly) wall.
- Surgery is needed to address the condition, putting any organs back into the belly and closing the opening.
- Researchers estimate that about 1 in every 3,704 babies is born with omphalocele in the United States.
What it is
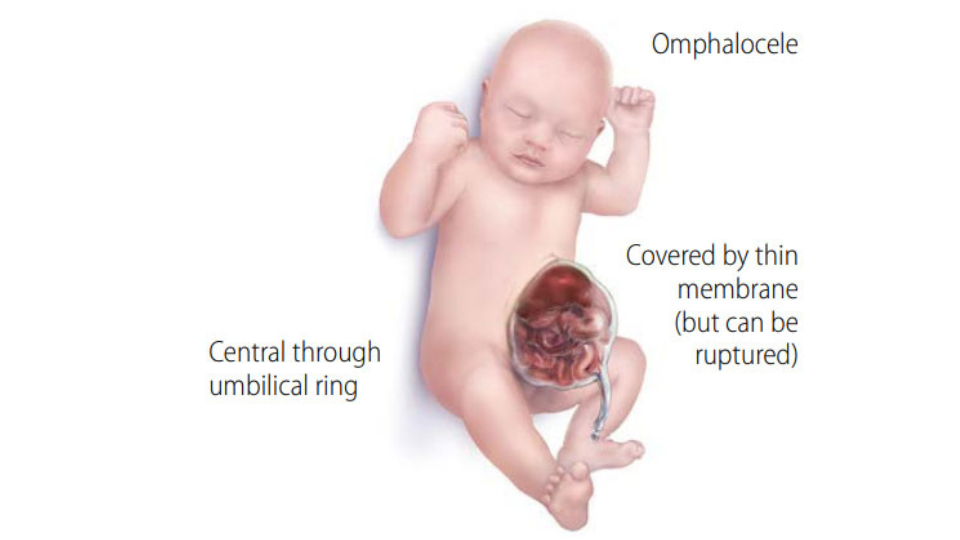
Omphalocele, also known as exomphalos, is a birth defect of the abdominal wall.
The infant's intestines, liver, or other organs stick outside of the belly through the belly button. The organs are covered in a thin, nearly transparent sac that usually is intact at birth.
As babies develop in early pregnancy, the intestines get longer and push out from the belly into the umbilical cord. By the eleventh week of pregnancy, the intestines normally go back into the belly. If this does not happen, an omphalocele occurs.
The omphalocele can be small with only some of the intestines outside of the belly. Or, it can be large, with many organs outside of the belly.
Babies born with an omphalocele may have additional complications. Their abdominal cavity, the space in the body that holds these organs, might not grow to its normal size. Also, infection is a concern, especially if the sac around the organs is broken. Sometimes, an organ might become pinched or twisted, and loss of blood flow might damage the organ.
Babies born with an omphalocele often have other birth defects, such as heart defects, neural tube defects, and chromosomal abnormalities.1
Risk factors
The causes of omphalocele in most cases are unknown. The role that genetics and the environment play in causing omphalocele needs to be studied further. Some known factors that may increase the risk of having a baby with omphalocele include:
- Alcohol or heavy tobacco use before or during pregnancy2
- Use of selective serotonin-reuptake inhibitors during pregnancy3
- Pre-pregnancy obesity4
CDC continues to study birth defects such as omphalocele and how to prevent them.
Screening and diagnosis
An omphalocele can be diagnosed during pregnancy or after the baby is born.
During pregnancy
An omphalocele might result in an abnormal result on a blood or serum screening test. It might also be seen during an ultrasound.
After a baby is born
In some cases, an omphalocele might not be diagnosed until after a baby is born. An omphalocele is seen immediately at birth.
Treatment
Treatment for infants with an omphalocele depends on a number of factors, including:
- The size of the omphalocele
- The presence of other birth defects or chromosomal abnormalities
- The baby's gestational age
If the omphalocele is small, it usually is treated with surgery soon after birth. If the omphalocele is large (many organs outside of the belly), the repair might be done in stages. The exposed organs might be covered with a special material and moved back into the belly over time. When all the organs have been put back in the belly, the opening is closed.
Resources
The views of this organization are its own and do not reflect the official position of CDC.
Omphalocele.net: Omphalocele.net provides support and encouragement to families who may be expecting a child with omphalocele, or people born with omphalocele.
- Stoll C, Alembik Y, Dott B, Roth MP. Omphalocele and gastroschisis and associated malformations. Am J Med Genet A. 2008 May 15;146A(10):1280-5.
- Bird TM, Robbins JM, Druschel C, Cleves MA, Yang S, Hobbs CA, & the National Birth Defects Prevention Study. Demographic and environmental risk factors for gastroschisis and omphalocele in the National Birth Defects Prevention Study. J Pediatr Surg, 2009;44:1546-1551.
- Alwan S, Reefhuis J, Rasmussen SA, Olney RS, Friedman JM, & the National Birth Defects Prevention Study. Use of Selective Serotonin-Reuptake Inhibitors in Pregnancy and the Risk of Birth Defects. N Engl J Med, 2007;356:2684-92.
- Waller DK, Shaw GM, Rasmussen SA, Hobbs CA, Canfield MA, Siega-Riz AM, Gallaway MS, Correa A, & the National Birth Defects Prevention Study. Prepregnancy obesity as a risk factor for structural birth defects. Arch Pediatr Adolesc Med, 2007;161(8):745-50.
- Stallings, E. B., Isenburg, J. L., Rutkowski, R. E., Kirby, R. S., Nembhard, W.N., Sandidge, T., Villavicencio, S., Nguyen, H. H., McMahon, D. M., Nestoridi, E., Pabst, L. J., for the National Birth Defects Prevention Network. National population-based estimates for major birth defects, 2016–2020. Birth Defects Research. 2024 Jan;116(1), e2301.