Key points
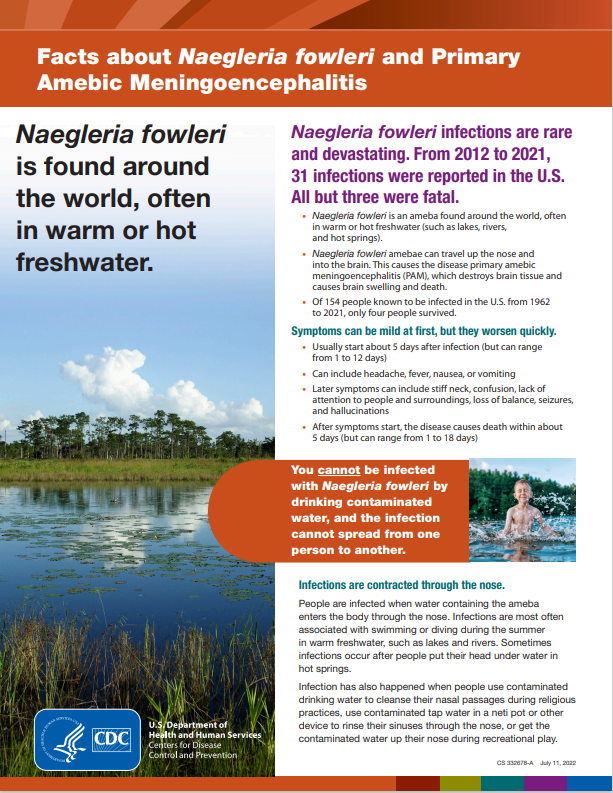
- Naegleria fowleri is a free-living ameba, a kind of one-celled organism that thrives in warm freshwater lakes, rivers, and hot springs.
- It is often called the "brain-eating ameba" because it can infect the brain and destroy brain tissue.
- Brain infections caused by Naegleria fowleri are very rare but nearly always fatal.

Overview
Naegleria fowleri lives in soil and warm freshwater lakes, rivers, ponds, and hot springs around the world.
In very rare cases, Naegleria fowleri has been found in poorly maintained swimming pools, splash pads, and other recreational venues. The ameba also has been found in tap water.
If water containing the ameba goes up the nose and to the brain, it can cause an infection called primary amebic meningoencephalitis (PAM). Typically, fewer than 10 people a year in the United States get PAM. Nearly everyone who gets PAM dies from it.
Between 1962 and 2024, there were 167 reported cases of PAM in the United States. Only four have survived.
Signs and symptoms
Early symptoms of PAM can include headache, fever, nausea, and vomiting. PAM progresses rapidly. Most people with PAM die within 1 to 18 days after symptoms begin. It usually leads to coma and death after 5 days.
As PAM progresses, symptoms can include stiff neck, confusion, lack of attention to people and surroundings, loss of balance, and hallucinations.
Exposure risks
Brain infections caused by Naegleria fowleri usually occur after someone goes swimming or diving in a lake, river, or other fresh water during summer months. Infections often happen when it's been hot for long periods, resulting in higher water temperatures and lower water levels.
A few infections have occurred when people used tap water that contained Naegleria fowleri to rinse their sinuses or cleanse their nasal passages.
In very rare instances, people have become infected from recreational water like splash pads and a surf park that did not have enough chlorine.
You cannot get a Naegleria fowleri infection from swallowing water containing the ameba. You also can't get an infection from someone else or pass it on to others.
Reducing risk
To help protect yourself against a Naegleria fowleri infection:
- Hold your nose or wear a nose clip if you are jumping or diving into fresh water.
- Always keep your head above water in hot springs.
- Don't dig in shallow water because the ameba is more likely to live there.
- Use distilled or boiled tap water when rinsing your sinuses or cleansing your nasal passages.
Diagnosis
A Naegleria fowleri infection is diagnosed using laboratory tests. These tests are available in only a few labs in the United States, including CDC.
Because these infections are so rare and hard to detect, diagnosis sometimes happens after a person has died.
Contact a healthcare provider immediately if you or a loved one is experiencing symptoms of PAM.
Treatment and recovery
Naegleria fowleri can cause PAM which destroys brain tissue and causes the brain to swell. Unfortunately, more than 97% of people with PAM have died from the infection.
PAM progresses very quickly. This has made treatments for the disease difficult to identify. There is some evidence that certain drugs may be effective.
What CDC is doing
CDC's Free-Living and Intestinal Amebas Lab is one of only a few labs in the country that can identify Naegleria fowleri. It is experienced in diagnosing Naegleria fowleri infections and can provide results quickly.
Free-living amebas
A free-living ameba is a kind of one-celled organism that lives in water and soil around the world. Most people will come into contact with these amebas during their lives but won't get sick. Others will develop rare but serious infections.
Although there are several types of free-living amebas that live in the environment, three are known to cause severe disease in people:
- Naegleria fowleri
All of these amebas can cause life-threatening brain infections. Some can also cause infections of the eyes, skin, sinuses, and other parts of the body.