What to know
- Primary amebic meningoencephalitis (PAM) is a rare but nearly always fatal brain infection caused by the ameba Naegleria fowleri.
- PAM is diagnosed using laboratory tests.
- The tests are available in only a few laboratories in the United States, including CDC.
Diagnosing Naegleria fowleri infection
Clinicians
For 24/7 diagnostic assistance, specimen collection guidance, shipping instructions, and treatment recommendations, contact the CDC Emergency Operations Center at 770-488-7100
PAM is diagnosed by detecting Naegleria fowleri amebas using different tests offered by only a few U.S. laboratories, including CDC. The tests include:
- A polymerase chain reaction (PCR) test that detects Naegleria fowleri in a patient's cerebrospinal fluid (CSF) or tissue
- Immunohistochemical (IHC) testing and indirect immunofluorescent (IIF) staining that use specific antibodies against Naegleria fowleri to detect the ameba
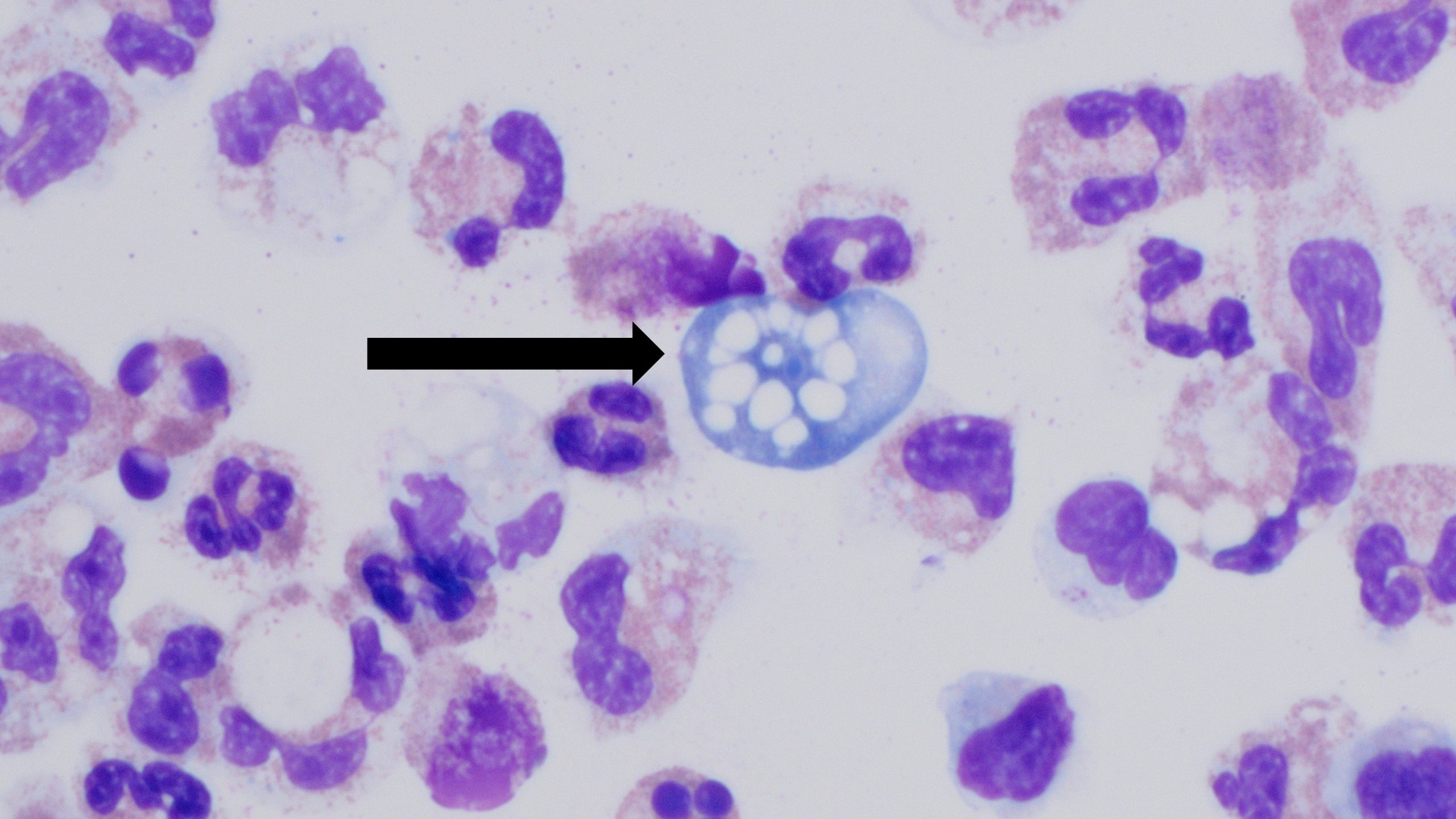
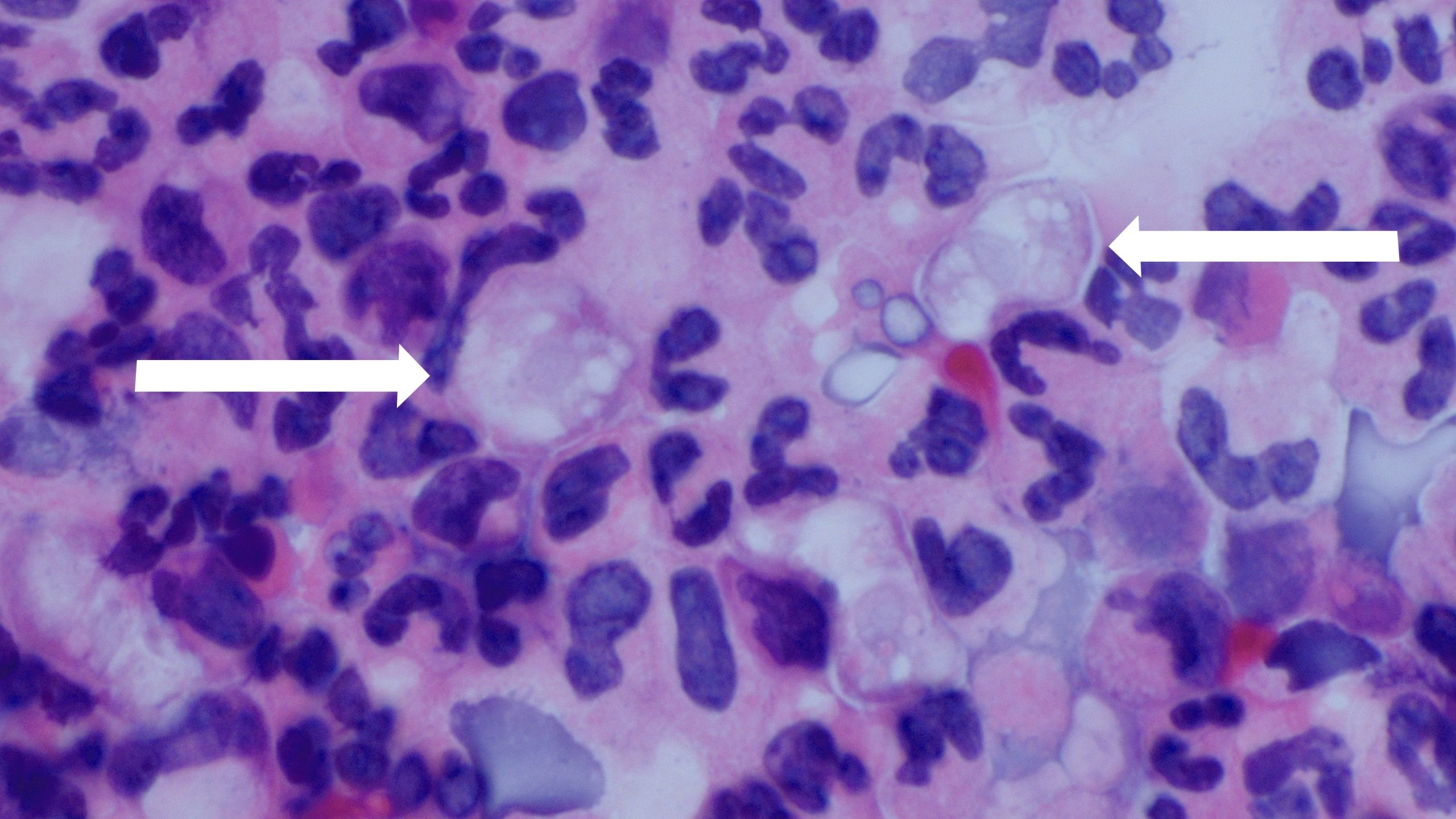
- Direct visualization by examining CSF under a microscope. Naegleria fowleri can be identified in CSF smears or cultures using hematoxylin and eosin (H&E), periodic acid-Schiff (PAS), trichrome, Giemsa, or Wright-Giemsa stains. Note: A Gram stain should be avoided since Naegleria fowleri can be destroyed during heat fixation.
CDC offers diagnostic assistance for Naegleria fowleri infection to physicians and scientists through DPDx and the Free-Living and Intestinal Amebas (FLIA) Lab.
Morphology experts at DPDx can evaluate microscopic images. Scientists at the FLIA laboratory provide diagnostic assistance using molecular and immunofluorescence assays.
For Everyone
About CDC's Naegleria fowleri Program