At a glance
- Diagnosis of malaria depends on blood smears and evaluation of clinical severity in presenting patients suspected of malaria.
- Providers may determine the appropriate treatment using CDC's algorithm.

Clinical resources
CDC Malaria Hotline
Healthcare providers can call the CDC Malaria Hotline for clinical consultation about malaria diagnosis and treatment:
- Monday – Friday, 9 a.m. 5 p.m. EST: (770) 488-7788
- After hours, weekends, and federal holidays: (770) 488-7100
Algorithm: diagnosis and treatment of malaria
Detailed dosing information and treatment regimens for special populations (children and pregnant women) can be found in the CDC Malaria Treatment Tables.
Download the PDF version of the diagnosis and treatment algorithm.
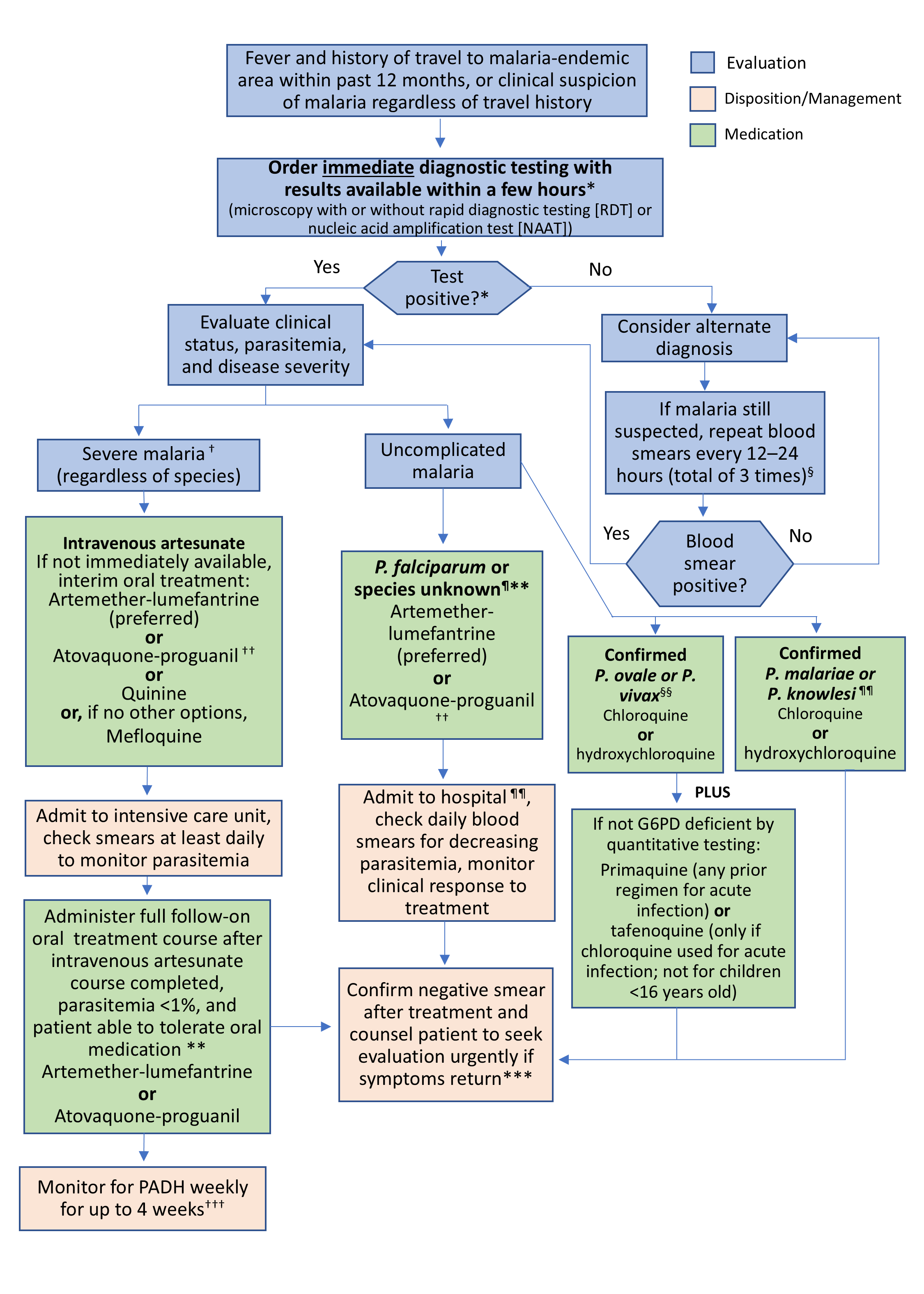
G6PD = Glucose 6 Phosphate Deficiency; PADH = Post Artesunate Delayed Hemolysis; NAAT= Nucleic acid amplification test; RDT = Rapid Diagnostic Test
Footnotes:
* Malaria can rapidly progress to severe life-threatening disease in the absence of prompt diagnosis and appropriate treatment. An initial diagnostic test result for malaria must be available immediately (i.e., results available within a few hours) and should not be sent out to laboratories that take days or weeks. Preliminary review of blood smears concerning for intracellular parasites is sufficient to initiate treatment. If your facility cannot provide results immediately, strongly consider transferring the patient for prompt evaluation of malaria. If RDT or NAAT performed, microscopic evaluation of blood smears should also be performed concurrently.
† Laboratory-confirmed or suspected malaria cases with ≥1 clinical criteria for severe disease (impaired consciousness/ coma, prostration, seizures, severe anemia [hemoglobin <7mg/dl], acute kidney injury/ decreased urine output, pulmonary edema or acute respiratory distress syndrome, circulatory collapse/ shock, acidosis, jaundice, abnormal bleeding/ disseminated intravascular coagulation, hypoglycemia); and/or parasitemia ≥5%.
§ If validated molecular test (PCR or other NAAT) is negative, subsequent smears are generally not necessary unless clinical suspicion remains high.
¶ Chloroquine (or hydroxychloroquine) is an option for P. falciparum acquired in Central America west of Panama Canal, Haiti, or Dominican Republic. Additional options include quinine plus doxycycline (or quinine plus clindamycin in pregnant women); or mefloquine if no other treatment options are available.
** If species later identified as P. vivax or P. ovale, anti-relapse treatment for hypnozoites is necessary.
†† Atovaquone-proguanil not indicated for pregnant women unless no other options and benefits outweigh risks.
§§ If P. vivax acquired in Papua New Guinea or Indonesia, use treatment options for P. falciparum because P. vivax resistance to chloroquine has been reported in these countries.
¶¶ Admission recommended for any P. falciparum, P. knowlesi, or if species is unknown until parasitemia has been shown to be decreasing in response to treatment and patient is afebrile and clinically appropriate for discharge.
*** If discharged or never hospitalized before a negative smear, it should be confirmed as an outpatient within a week of treatment, if possible.
††† If CBC is abnormal, additional laboratory evaluation should include reticulocyte count, haptoglobin, lactate dehydrogenase, total bilirubin, and a repeat blood smear.