
The emerging fungus C. auris spreads in hospitals. It can cause severe multidrug-resistant illness.
Learn how healthcare providers can stop C. auris from spreading and protect patients.
Patients are screened to find out if they carry and can spread C. auris.
In 2024 there were 6,304 clinical cases of C. auris reported. Cases have increased since 2016.
For healthcare and laboratory professionals

Healthcare providers and laboratorians can find important resources on C. auris.
More fungal diseases and related resources
Fungal diseases and antifungal resistance are increasing worldwide. Misdiagnosis is common.
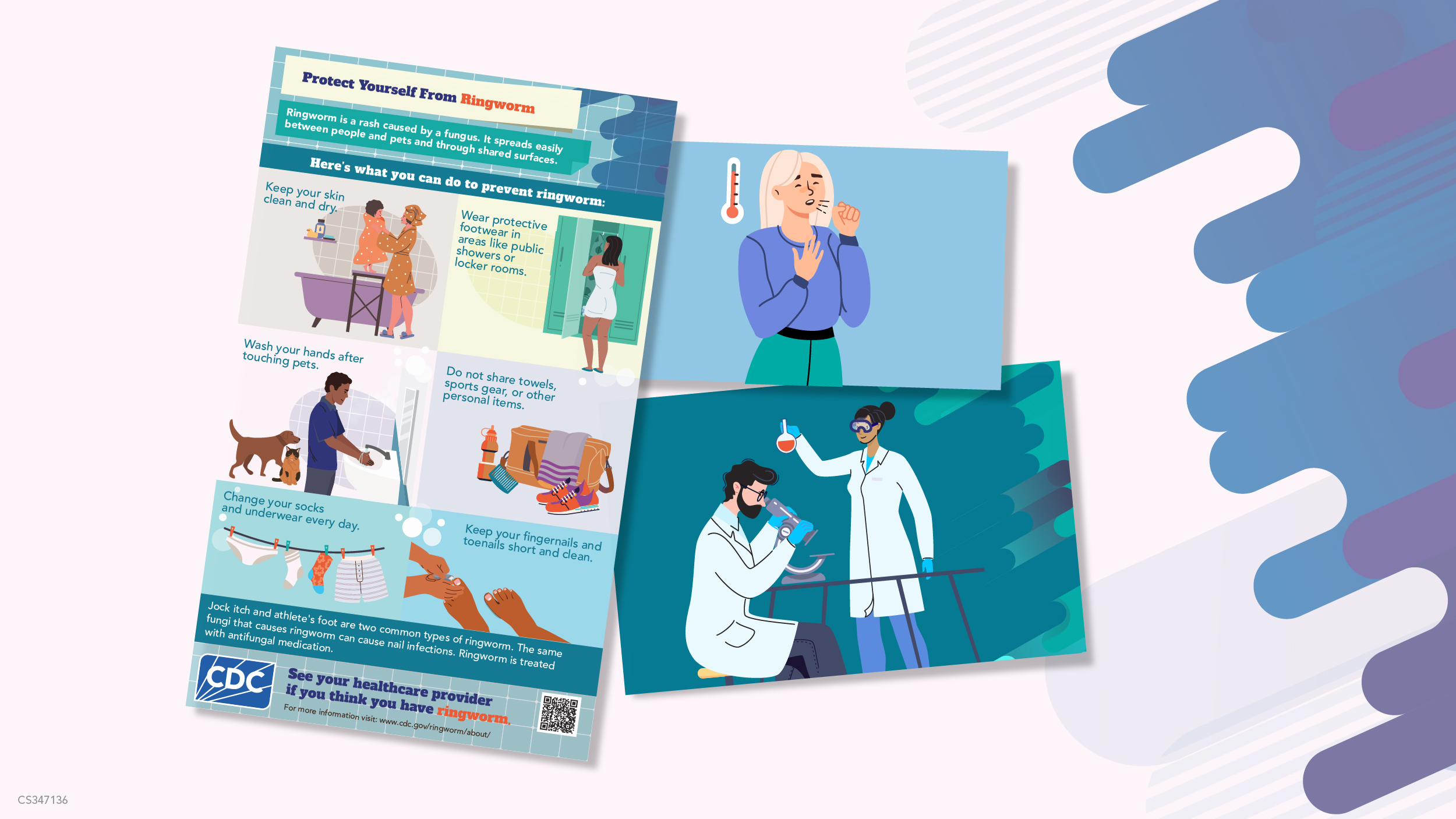
Find and download social media graphics, fact sheets, infographics, and animated videos.

Access webinars and podcasts featuring world experts in fungal diseases and find clinical resources.