Key points
- Rubella can lead to complications and death and can be prevented by vaccination.
- Many rubella infections aren't recognized; the rash resembles many other rash illnesses.
- Clinical diagnosis of rubella virus is unreliable. Up to half of infections may be subclinical.
- Isolate people suspected to have rubella and report them to the local health department.

Introduction
Rubella virus is an enveloped, positive-stranded RNA virus classified as a Rubivirus in the Matonaviridae family.
Incubation period
The average incubation period of rubella virus is 17 days, with a range of 12 to 23 days. People infected with rubella are most contagious when the rash is erupting. But they can be contagious from 7 days before to 7 days after the rash appears.
How it spreads
Rubella is transmitted primarily through direct or droplet contact from nasopharyngeal secretions. Humans are the only natural hosts. In temperate climates, infections usually occur during late winter and early spring.
Disease rates
Prior to vaccine introduction:
Before the rubella vaccine was licensed in the United States in 1969, rubella was a common disease that occurred primarily among young children. Epidemics occurred every 6 to 9 years, with the highest number of cases during the spring.
Post-vaccine era:
Rubella was declared eliminated (the absence of endemic transmission for 12 months or more) from the United States in 2004. However, it is still commonly transmitted in many parts of the world. As a result, less than 10 cases (primarily import-related) have been reported annually in the United States since elimination was declared. Rubella incidence in the United States has decreased by more than 99% from the pre-vaccine era.
Because rubella continues to circulate in other parts of the world, an estimated 100,000 infants are born with congenital rubella syndrome (CRS) annually worldwide.
Clinical features
Rubella is characterized by a mild, maculopapular rash along with lymphadenopathy, and a slight fever. About 25% to 50% of infections are asymptomatic.
Characteristics of maculopapular rash:
- Usually starts on the face
- Becomes generalized within 24 hours
- Lasts a median of 3 days
- Occurs in 50% to 80% of people infected with rubella
Characteristics of lymphadenopathy:
- May precede rash
- Often involves posterior auricular or suboccipital lymph nodes
- Can be generalized
- Lasts between 5 and 8 days
Prevention
Rubella vaccination:
Rubella can be prevented with rubella-containing vaccine. Rubella vaccine is usually administered as the combination measles, mumps, and rubella (MMR) vaccine. The combination measles, mumps, rubella, and varicella (MMRV) vaccine can be used for children aged 12 months through 12 years.
CDC recommends children get 2 doses of MMR vaccine. Adults born during or after 1957 should receive at least one dose of rubella-containing vaccine. Pregnant women who do not have evidence of immunity should be vaccinated immediately after giving birth.
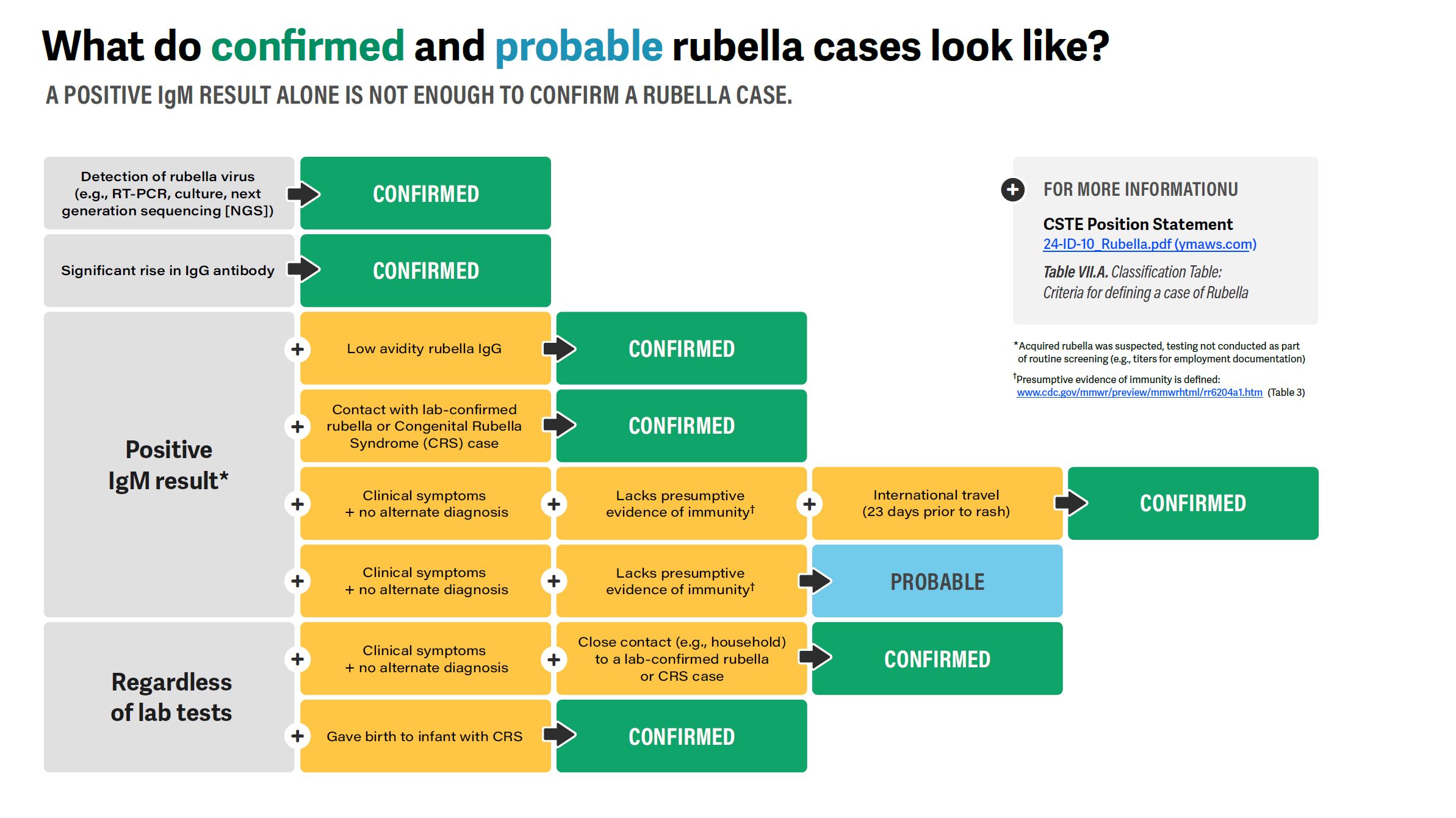
Testing and diagnosis
Clinical diagnosis of rubella virus is unreliable and should not be considered in assessing immune status. Up to half of all infections may be subclinical or inapparent. Many rubella infections are not recognized because the rash resembles many other rash illnesses.
Healthcare providers should:
- Consider rubella in unvaccinated patients with febrile rash illness and other rubella symptoms, especially if the person recently traveled internationally or was exposed to a person with a confirmed rubella case.
- Promptly isolate people suspected to have rubella and report them to the local health department.
- Collect nasopharyngeal swabs, throat swabs, or urine specimens for viral detection by polymerase chain reaction (PCR) testing and molecular typing, and blood for serology testing.
Patient management
There is no specific antiviral therapy for rubella infection.
Isolation
Patients with rubella should be isolated for 7 days after they develop rash.
In settings where pregnant women may be exposed, outbreak control measures should begin as soon as rubella is suspected and should not be postponed until laboratory confirmation of cases.
People at risk who cannot readily provide acceptable evidence of rubella immunity should be considered susceptible and should be vaccinated.
People without evidence of immunity who are exempt from rubella vaccination for medical, religious, or other reasons should be excluded from affected institutions in the outbreak area until 23 days after the onset of rash in the last case of rubella.
Unvaccinated people who receive MMR vaccine as part of rubella outbreak control may immediately return to school provided all people without documentation of rubella immunity have been excluded.
Complications
Rubella can lead to complications and death.
Arthralgia or arthritis may occur in up to 70% of adult women with rubella. Rare complications include thrombocytopenic purpura and encephalitis.
Rubella infection during pregnancy
When rubella infection occurs during pregnancy, especially during the first trimester, serious consequences can result. These include:
- Miscarriages
- Fetal deaths/stillbirths
- Severe birth defects known as CRS