Key points
- Rift Valley Fever (RVF) is caused by a virus carried by mosquitoes that can spread to livestock or people.
- People get RVF through contact with blood, body fluids, or tissues of infected animals.
- People also get RVF through bites from infected mosquitoes.
- Most people with RVF get better without treatment.
More Information
Overview
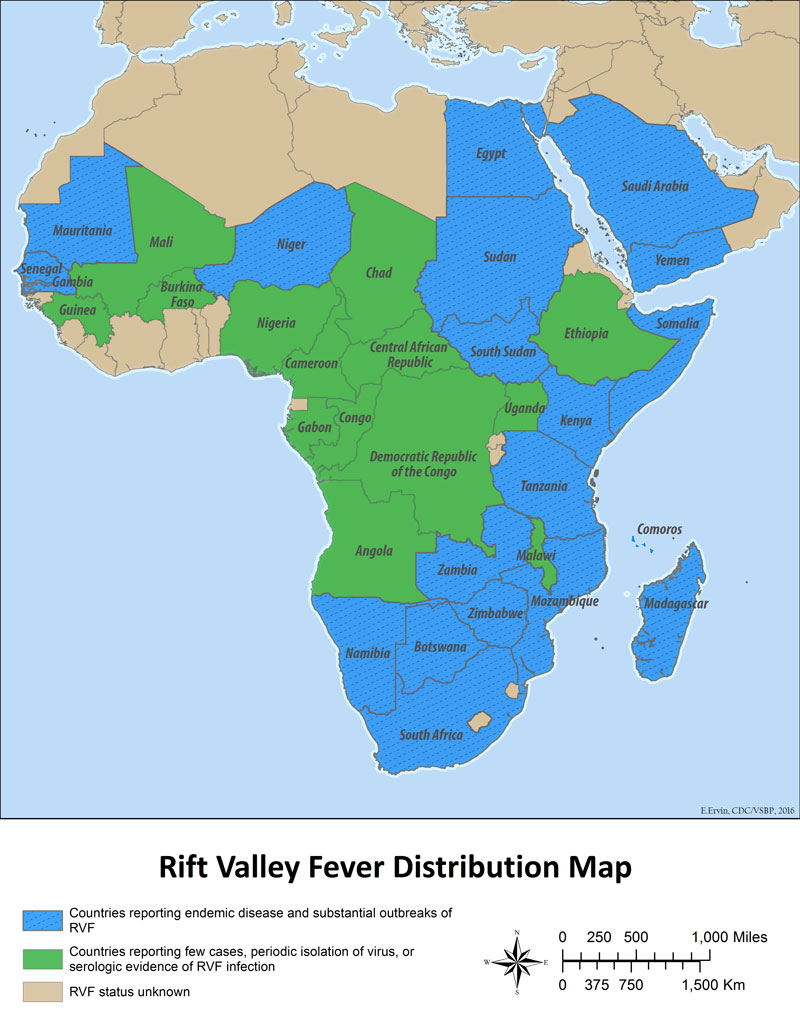
Rift Valley fever (RVF) is caused by Rift Valley fever virus, which is found in most of sub-Saharan Africa, especially eastern and southern Africa. Rift Valley fever virus is carried by mosquitoes and can spread to people and animals, including cows, buffalo, sheep, goats, and camels.
RVF most often affects domestic animals including livestock and causes severe illness, pregnancy loss and death in the animals. RVF creates a major economic burden in affected areas as raising animals for milk and meat is an important source of income for many people.
People usually get RVF through contact with blood, body fluids, or tissues of infected animals in areas where the virus is found. This can happen when people perform the following activities without taking steps to prevent infection:
- Slaughtering or butchering
- Caring for sick animals
- Providing veterinary procedures like helping an animal give birth
- Eating or drinking raw or undercooked animal products
People can get RVF through bites from infected mosquitoes and, rarely, other biting insects. Laboratory workers have also gotten accidentally infected during testing for Rift Valley fever virus.
There has never been a case reported of RVF virus spreading from person to person.
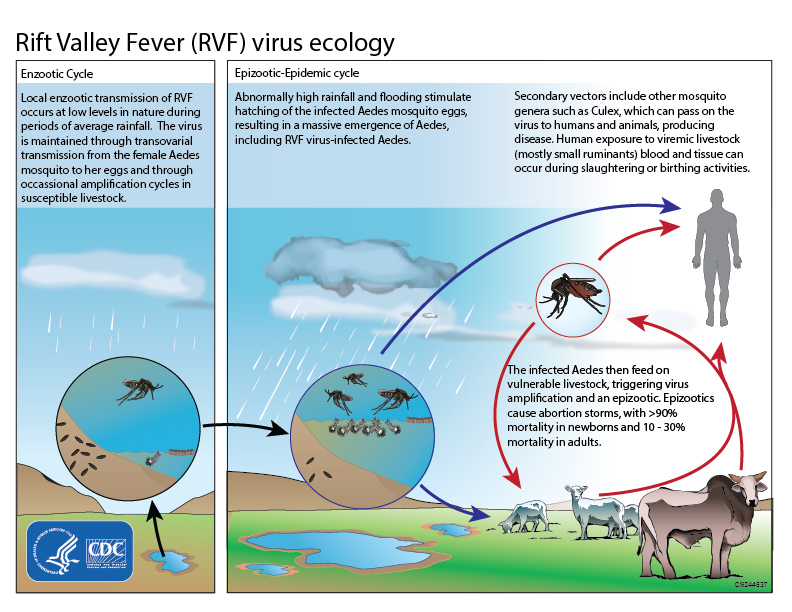
RVF outbreaks typically occur during years of unusually heavy rainfall and flooding.
- Excessive rainfall allows more mosquito eggs to hatch.
- The virus spreads from the female mosquitoes to the eggs.
- As more mosquitoes hatch, the potential for the virus to spread directly to animals and people increases.
- In addition, RVF outbreaks in animals leads to people handling infected animals more often, increasing their risk of getting sick.
Healthcare providers:
Signs and symptoms
Signs and symptoms begin about two to six days after exposure to the RVF virus. People with RVF often have either no symptoms or a mild illness that includes fever, weakness, back pain, and dizziness. Typically, patients recover without treatment within two to seven days after symptoms start.
Eight to 10 percent of people with RVF develop severe symptoms, including:
- Eye disease with blurred and decreased vision, or sores on the eyes. These sores disappear after 10-12 weeks for most patients. Around half of all patients with sores on the center of the retina will have permanent vision loss.
- Inflammation of the brain (encephalitis) in less than 1 percent of RVF patients, which can lead to headaches, coma, or seizure. Encephalitis can cause severe and long-lasting health problems.
- Bleeding occurs in less than 1 percent of all RVF patients. Symptoms of bleeding may begin with yellowing of the skin and eyes (jaundice), vomiting blood, bloody stool, or bleeding from gums, skin, nose, and injection sites. Fifty percent of patients with bleeding die.
Overall, about 1 percent of people infected with RVF die of the disease.
Exposure risks
People at risk for becoming infected with RVF virus include:
- Spending time in rural areas and sleeping outdoors at night in areas where outbreaks regularly occur. This can increase opportunities for being bitten by infected mosquitoes.
- Working with potentially infected animals in areas where the virus regularly occurs. This includes animal herdsmen, slaughterhouse workers, and animal caretakers like veterinarians.
- Traveling to areas where RVF regularly occurs or during an outbreak.
Prevention
People living in or visiting areas with RVF can prevent infection with these steps:
- Avoid contact with blood, body fluids, or tissues of potentially infected animals. People working with animals in areas where RVF virus is found regularly should wear gloves, boots, long sleeves, and a face shield to protect themselves.
- Handle, eat, and drink animal products safely. All animal products, including meat, milk, and blood, should be thoroughly cooked before eating or drinking them.
- Protect yourself against mosquitoes and other bloodsucking insects. Use insect repellents and bed nets, and wear long sleeved shirts and long pants to cover exposed skin.
Protect Yourself from Mosquitoes
No RVF vaccines are currently available for people. There are a few types of vaccines available for use in animals.
Testing and diagnosis
Diagnosing RVF, especially early in the illness, can be difficult because symptoms can be mild and similar to many other illnesses. RVF virus can be confirmed with laboratory testing.
For healthcare providers
Clinicians in the United States who may be concerned a patient could have RVF should contact their local or state, tribal, local, or territorial health department immediately.
Treatment and recovery
Most RVF cases are mild, and people tend to get better without treatment within two to seven days. Over-the-counter medications like ibuprofen or acetaminophen can help with symptoms of mild illness like fever and body aches. People who are very sick may need to go to the hospital, where they'll receive supportive care like fluids and pain medication.
Resources
Posters
- What to Know about RVF (English)
- What to know about RVF (French)
- What to Know about RVF for Herders, Farmers, Butchers and Abbatoir Workers (English)
- What to Know about RVF for Herders, Farmers, Butchers and Abbatoir Workers (French)
- What to Know about RVF for Veterinarians (English)
- What to Know about RVF for Veterinarians (French)
Other resources
Additional viral hemorrhagic fever information
- Detection of Sporadic Outbreaks of Rift Valley Fever in Uganda through the National Viral Hemorrhagic Fever Surveillance System, 2017–2020 in: The American Journal of Tropical Medicine and Hygiene Volume 108 Issue 5 (2023) (ajtmh.org)
- Cossaboom CM, Nyakarahuka L, Mulei S, et al. Rift Valley Fever Outbreak during COVID-19 Surge, Uganda, 2021. Emerging Infectious Diseases. 2022;28(11):2290-2293. doi:10.3201/eid2811.220364