2006 STD Prevention Conference - SEE FACT SHEET - 8 May 2006
This web page is archived for historical purposes and is no longer being updated.
CDC’s Updated Plan to Eliminate Syphilis in the United States
In 1999, the Centers for Disease Control and Prevention (CDC) launched The National Plan to Eliminate Syphilis from the United States to capitalize on a decade of declining rates of syphilis. The ambitious plan was designed to end the sustained transmission of the disease in the U.S. by focusing efforts on the populations most affected by syphilis – heterosexual minority populations, particularly African Americans. In these populations, substantial progress has been made in reducing the burden of syphilis, yet overall syphilis rates have been on the rise since 2001, largely due to increasing rates of syphilis among men who have sex with men (MSM).
To overcome emerging challenges, while continuing progress among African Americans and women, CDC today issued an updated plan, Together We Can: The National Plan to Eliminate Syphilis from the United Statespdf icon[PDF – 7.3 MB]. This fact sheet highlights key elements of the updated plan.
What is syphilis elimination and what will it mean for the nation’s health?
At the national level, syphilis elimination is defined as the absence of sustained transmission of the disease. Despite recent challenges, generally low syphilis rates provide an opportunity to achieve this goal. Syphilis elimination is possible because the disease is easy to cure once diagnosed, and because the syphilis epidemic is concentrated in a small number of geographic areas. In 2004, more than 50 percent of infectious (also called primary and secondary, or P&S) syphilis cases were reported from just 20 U.S. counties.
Elimination of syphilis would have far-reaching public health benefits because it would remove two serious consequences of the disease – increased likelihood of HIV transmission, and serious complications in pregnancy and childbirth, such as spontaneous abortions, stillbirths, and congenital syphilis (syphilis among newborns who acquired it from their mothers).
Syphilis elimination accomplishments to date
Since CDC’s original plan was issued in 1999, there have been significant declines in syphilis rates among key populations at risk, including African Americans, women, and newborns. Between 1999 and 2004:
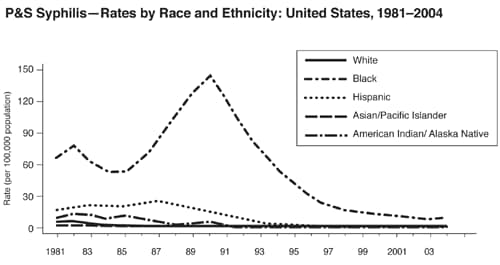
- P&S syphilis rates among blacks decreased 37 percent, from 14.3 to 9.0 cases per 100,000
- The black-white racial disparity in syphilis rates fell from 28.6:1 to 5.6:1
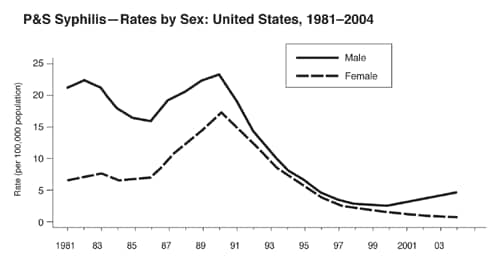
- Rates among women overall fell 60 percent, from 2.0 to 0.8 cases per 100,000
- Rates of congenital syphilis declined 39 percent, from 14.5 to 8.8 per 100,000 live births
Elimination efforts face new challenges
Despite important gains in many populations, overall syphilis rates have been on the rise since 2001, largely due to increases among MSM. Overall, the P&S syphilis rate among males increased 68 percent from 1999 to 2004. While surveillance data are not available by risk behavior, a separate CDC analysis suggests that approximately 64 percent of all adult P&S syphilis cases in 2004 were among MSM, up from an estimated 5 percent in 1999. In addition, P&S syphilis rates increased among African Americans in 2004, for the first time in more than a decade. The increase largely reflected significant increases among black men (up 22.6% from 2003 to 2004).
CDC’s updated plan expands elimination efforts to meet the latest challenges
CDC’s updated plan, Together We Can: The National Plan to Eliminate Syphilis from the United Statespdf icon[PDF – 7.3 MB], is designed to sustain elimination efforts in populations traditionally at risk, and to carry out innovative solutions to the resurgence of syphilis among MSM.
The plan is guided by three goals, each of which includes concrete activities for CDC, state and local health departments, community organizations, and private healthcare providers.
-
Goal One: Invest in and enhance public health services and interventions
Ensuring that the nation’s public health system – including the local and state health departments on the front lines of the fight – is adequately equipped to fight syphilis is critical to success.-
Improve surveillance and outbreak response. Accurate and detailed surveillance data are essential to design effective syphilis prevention programs and to respond to syphilis outbreaks in specific populations. The updated plan recommends that state and local health departments:
- By the end of 2006, collect information on the gender of sexual partners and the sexual orientation of individuals diagnosed with syphilis, to more accurately assess the impact on MSM
- Provide epidemiology training to STD program staff at local health departments, many of which do not have personnel with significant expertise in this area, to ensure that program planners can interpret and respond to emerging trends
- Establish a Syphilis Outbreak Response Plan to address rapid, local increases in syphilis, as occurred among MSM in some U.S. cities over the past several years
-
Improve diagnosis, treatment, and prevention services. Limited resources in public STD clinics and limited training in private healthcare settings result in sub-standard syphilis prevention, care, and diagnosis in many communities.
The plan calls for:
- New and strengthened partnerships between health departments and other healthcare providers, such as community health centers and outreach clinics that serve at-risk populations, to ensure wider coverage of syphilis screening efforts
- Routine syphilis screening of MSM by HIV care providers and increased awareness among MSM of the importance of routine syphilis screening
- Where transmission is primarily among heterosexual populations, increasing the proportion of inmates screened in local jails, particularly female inmates. This strategy may help reach incarcerated commercial sex workers, a population at high risk for syphilis
- Increasing the proportion of pregnant women screened during prenatal care visits
- Improve testing and laboratory services. Among other activities, CDC and its partners are working to develop a rapid syphilis test to quickly diagnose syphilis, particularly in non-traditional community settings such as bars, clubs, and community centers, where people at risk can be reached effectively. The goal is to make a rapid test available for use in the U.S. within the next few years.
-
Improve surveillance and outbreak response. Accurate and detailed surveillance data are essential to design effective syphilis prevention programs and to respond to syphilis outbreaks in specific populations. The updated plan recommends that state and local health departments:
-
Goal Two: Prioritize and target interventions to populations at greatest risk
Expanded partnerships with affected communities, community-based organizations (CBOs), and local healthcare providers can help health officials tailor interventions and select venues to reach populations most at risk.-
Target interventions for groups most at risk. The plan calls for:
- Areas with high syphilis burdens to devote 15 to 30 percent of their CDC syphilis elimination funding to support the activities of local CBOs, in order to better reach affected populations (e.g., African Americans, MSM, and other minorities)
- Assessing healthcare access, and use of care and screening services, in affected populations
- Developing Internet-based interventions to reach the increasing number of MSM and others who meet partners online, and increasing outreach and screening for MSM in bathhouses, bookstores, HIV testing sites, and other venues
- State and local health departments to partner with local drug treatment centers to reach MSM and others who use drugs such as crystal methamphetamine
- Mobilize and support private healthcare providers. A growing number of people are diagnosed with syphilis by private physicians or by healthcare workers in community clinics. Many private practitioners, in particular, need training on case reporting, partner notification, and other public health practices. The plan calls for state and local health departments to provide training, policy guidance, and up-to-date syphilis information to private providers, community clinics, and others who provide services to populations at risk.
-
Target interventions for groups most at risk. The plan calls for:
-
Goal Three: Improve accountability of prevention efforts
Improving the accountability – and results – of syphilis elimination efforts nationwide requires investing in training, data-driven planning and evaluation, and research to enhance syphilis screening and prevention efforts. The plan prioritizes the following areas:- Improve training and staff development. CDC and its public health partners will work to ensure access to needed training for health department staff responsible for carrying out syphilis elimination activities. Training will address skills such as clinical and laboratory methods, data analysis, health communications, and community outreach. These efforts complement the healthcare provider training called for under Goal Two of the plan.
- Use data-driven planning and evaluation. Evidence-based planning and evaluation of programs help ensure the best use of limited program resources. The plan calls for all state and local health departments to develop annual syphilis elimination action plans based on local surveillance and research data.
- Carry out new research and development activities. The plan calls for research into the development of new strategies to diagnose and prevent syphilis. Among other activities, CDC and its partners will conduct research on the cost-effectiveness of new syphilis prevention interventions; examine the economic, social, and behavioral factors that must be addressed in order for interventions to succeed; and develop more effective screening programs.
Next steps – Implementing the plan
CDC is moving rapidly with its partners to implement the revised plan. A national network of Syphilis Elimination Coordinators, drawn from state and local health agencies, has been established to find ways to streamline training for STD program staff, and identify other ways to ensure rapid implementation of the plan. CDC is also taking additional steps to guide federal, state, and local health partners. During the next 6 months to two years, the agency will develop a specific action plan with a five-year timetable of activities, a Syphilis Elimination Research and Development strategy, and a template “outbreak response plan” to be adapted by state and local health departments.