Key points
- Symptom presentation varies due to different species of the schistosome parasite.
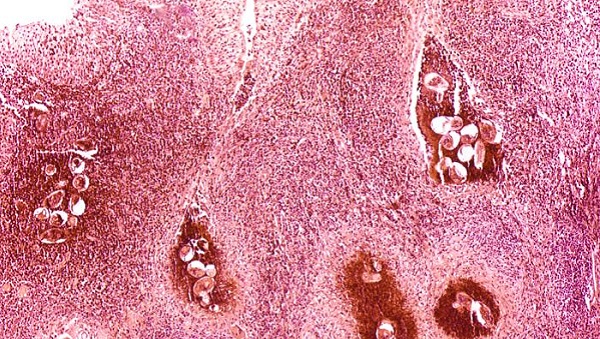
- Examination of stool and/or urine for ova is the primary method of diagnosis for suspected schistosome infections.
- Review travel and residency history to assist with proper diagnosis.
Recommended tests
Testing of stool or urine can be of limited sensitivity, particularly for travelers who may have lighter burden infections. The eggs are shed intermittently and in low amounts in light-intensity infections. Collect three samples on different days to increase the sensitivity of stool and urine examination.
Hematuria testing
The presence of hematuria can suggest a S. haematobium infection. However, this test is more useful for population studies in Africa and is not sufficiently sensitive or specific for individual patient diagnosis.
Serological testing
Serologic testing for antischistosomal antibody is recommended for diagnosis of travelers or immigrants from endemic areas who have not been treated appropriately for schistosomiasis in the past. Commonly used serologic tests detect antibodies to the adult worm.
For new infections, the serum sample tested should be collected at least 6 – 8 weeks after likely infection, to allow for full development of the parasite and antibody to the adult stage.
Serologic testing may not be appropriate for determining active infection in patients who have been repeatedly infected and treated in the past. This is because specific antibodies can persist despite cure. In these patients, serologic testing cannot distinguish resolved infection from active infection.
Antigen testing
An antigen test has been developed that can detect active infection based on the presence of schistosomal antigen. However, this test is not commercially available in the United States and is currently undergoing field evaluations for accurate diagnosis of low-intensity infections.
Diagnosis
Stool and urine
Examination of stool and/or urine for ova is the primary method of diagnosis for suspected schistosome infections. The choice of sample to diagnose schistosomiasis depends on the species of parasite likely causing the infection.
Adult stages of S. mansoni, S. japonicum, S. mekongi, and S. intercalatum live in the mesenteric venous plexus of infected hosts and eggs are shed in feces. S. haematobium adult worms are found in the venous plexus of the lower urinary tract and eggs are shed in urine.
Travel and residency
Careful review of travel and residence history is critical for determining whether infection is likely and which species may be causing infection.
It is important to remember that both S. mansoni and S. haematobium are endemic in some areas of sub-Saharan Africa. Patients with freshwater exposures in those areas should have both stool and urine samples examined for eggs.