What to know
CDC's Division of Reproductive Health (DRH) works with health agencies in lower resource countries to help reduce maternal and infant deaths. To improve health services, DRH uses monitoring and evaluation to:
What is monitoring and evaluation?
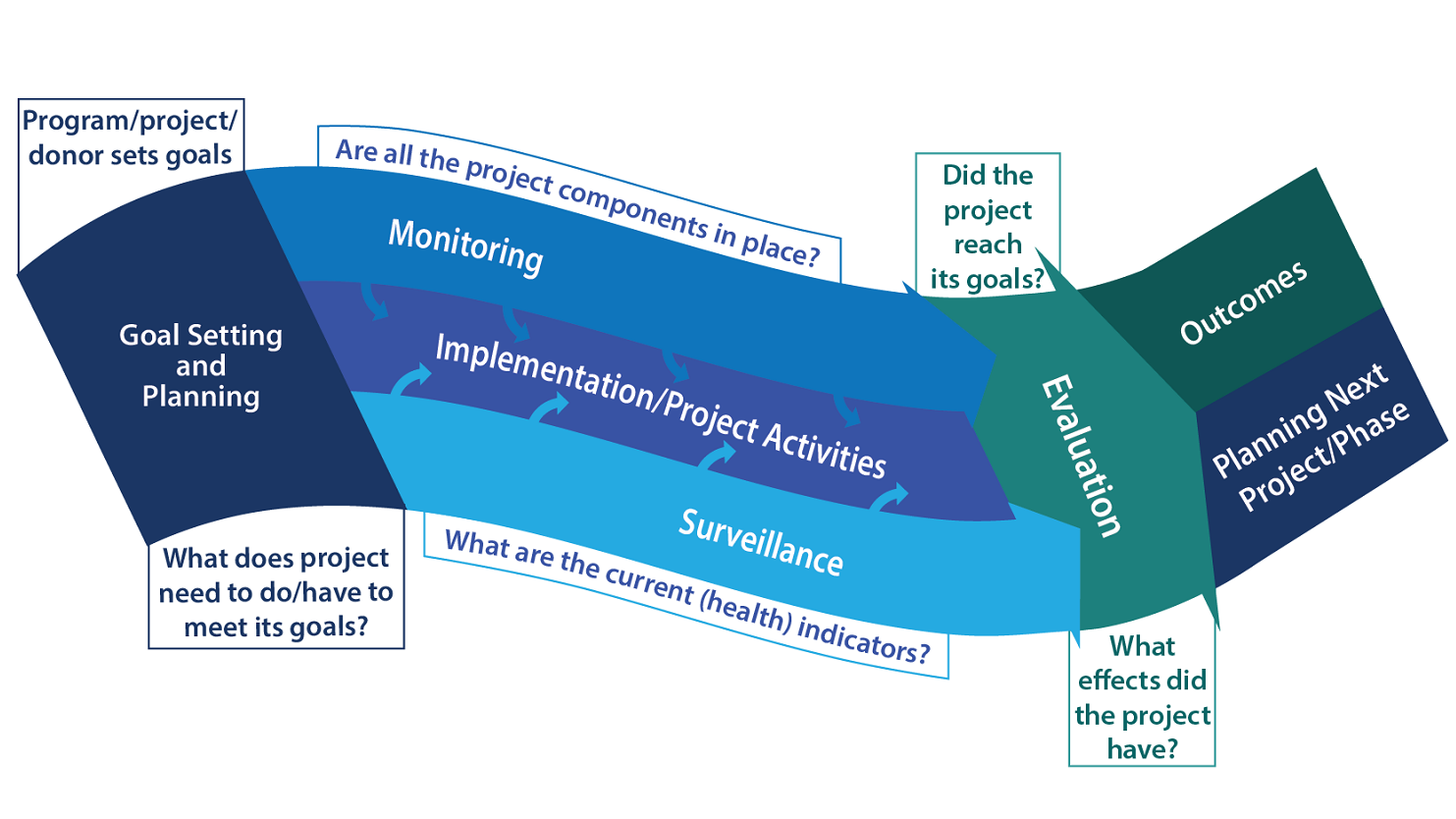
Monitoring and evaluation (M&E) activities may include the following three elements: monitoring, evaluation, and surveillance.
Monitoring
Monitoring a program's progress toward its goals involves:
- Periodically collecting program data (such as counting the number of midwives trained in emergency obstetric care).
- Tracking data over time against the desired outcome.
The following are some examples of DRH's monitoring activities:
- Counting all maternal deaths in areas where maternal mortality had never before been directly measured.
- Collecting data on every birth outcome (for both mother and infant) in health facilities.
- Conducting assessments on the implementation of project interventions, such as improving health facilities and transportation and referral systems.
Evaluation
Evaluating a program's success uses study designs and tools tailored to the program's goals. Evaluation looks at a program's effects on short- and long-term outcomes, such as reductions in mortality and improvements in quality of care.
The following are some examples of DRH's evaluation activities:
- Documenting the reductions in specific causes of maternal death, such as obstetric hemorrhage and sepsis (infection).
- Using geographic information system (GIS) mapping to evaluate project advancement.
- Designing tools, questionnaires, trainings, and data management systems so programs can collect and analyze their data in a scientifically sound manner.
Surveillance
Surveillance of a population's health status over time is done through ongoing detection, investigation, and reporting of health events. These indicators are then analyzed to see if they're improving and can provide an early warning to the program if they are not.
The following are some examples of DRH's health program surveillance activities:
- Helping counties improve systems to identify, report, and reduce maternal deaths
- Investigating the causes, circumstances, and preventability of each maternal death to learn how future deaths might be prevented.
What has DRH M&E work shown?
DRH has worked with the Maternal and Reproductive Health in Tanzania program and the Saving Mothers, Giving Life initiative (SMGL).
CDC's M&E activities produced the evidence that:
- The Maternal and Reproductive Health in Tanzania program contributed to reducing the maternal mortality ratio in health facilities in Kigoma region by 52% in 5 years.
- In 5 years, SMGL activities contributed to reducing maternal mortality in SMGL study districts by 44% in Uganda and by 41% in Zambia.