Learn about this groundbreaking effort to modernize the nation's public health data systems.
Learn More About the PHDS

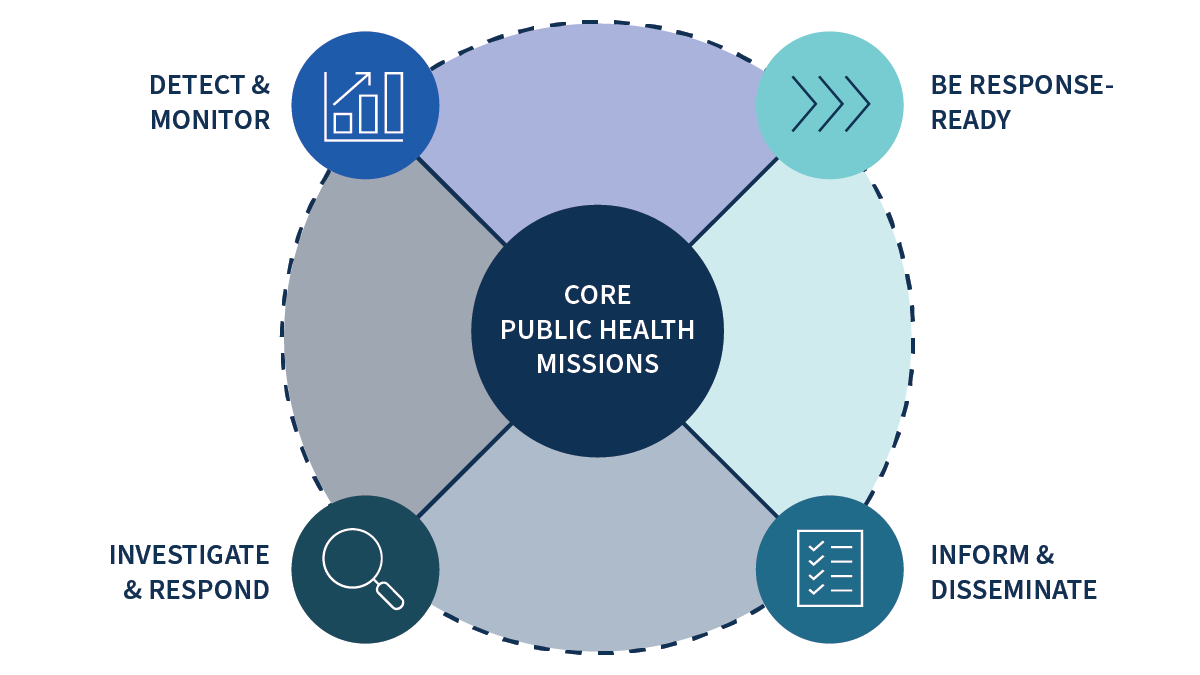
PHDS milestones are updated annually and center on four critical public health data goals.

Remarkable progress has been made in strengthening the nation’s public health data infrastructure.
The Public Health Data Strategy involves extensive collaboration with public health partners.
Stories

Examples of PHDS accomplishments and progress.