Highlights
- In September 2018, Hurricane Florence brought catastrophic flooding to the southeastern region of North Carolina.
- Near real-time syndromic surveillance data were essential to monitor injuries, illness, and deaths during and post-hurricane.
- Using syndromic surveillance, North Carolina epidemiologists monitored injuries, drownings, motor vehicle accidents, carbon monoxide exposure, medication refills, and other storm-related health events.
- Disaster shelter data, emergency department visits, and poison center calls were integrated to provide a complete picture of the storm’s health impacts.

Public health problem
Hurricane Florence made landfall as a Category 1 hurricane in North Carolina in September 2018. As a slow-moving storm, it brought record-breaking rainfall and catastrophic flooding to the southeastern region of the state. Mandatory evacuations swelled statewide shelters to more than 20,000 residents. Hazards such as breaches of coal ash and hog wasters added to the list of potential exposures. Real-time syndromic surveillance data were essential not only to monitor injuries, illness, and deaths during and post-hurricane but to provide actionable situational awareness to responders and the public.
Actions taken
The North Carolina Division of Public Health (NC DPH) conducted active, enhanced surveillance before, during, and after Hurricane Florence using the state syndromic surveillance system, NC DETECT, and the National Syndromic Surveillance Program (NSSP). NC DETECT uses emergency department (ED) visits from the state's 126 acute care hospitals, poison center calls, and emergency medical services (EMS) runs. NSSP has the same statewide ED data as NC DETECT. A hurricane dashboard was created in both systems before landfall to make information more easily available to any user.
NC DPH used a diverse set of syndromes to monitor injuries, drownings, motor vehicle accidents, carbon monoxide exposure, medication refills, etc. A hurricane syndrome was also created to try to capture visits specific to the event. Syndrome data were reviewed by staff epidemiologists, and pertinent information was included in a daily situation report that was shared with the State Emergency Operations Center (SEOC) and the Centers for Disease Control and Prevention (CDC).
During the response, CDC's NSSP team asked DPH officials if they wanted to integrate data from Disaster Medical Assistance Teams (DMATs) deployed in North Carolina. Within 24 hours, data from the two deployed DMATs, one in Wake County and one in Mecklenburg County, were available in NSSP.

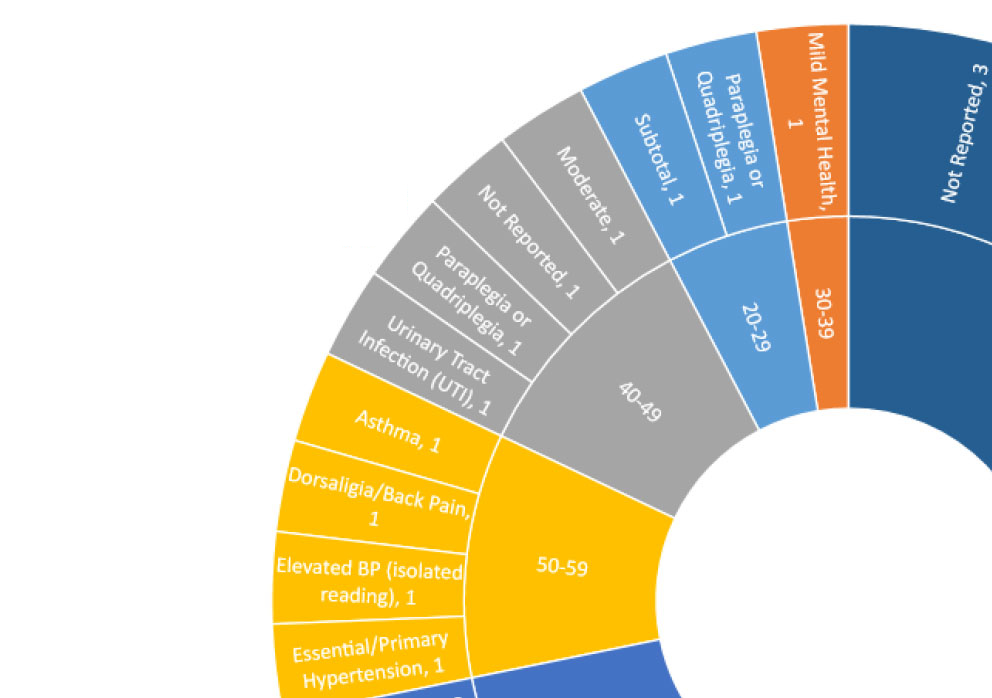
DMAT data were monitored along with ED visits and poison center calls. NSSP staff provided visual summaries of data for DPH review and analysis. Findings from the DMAT data, which were added to daily situation reports, provided insight into the health events experienced by those in shelters receiving DMAT care. Data were monitored for about one week until the DMATs were no longer deployed.
Outcome
A surveillance plan was in place before Hurricane Florence, but that plan did not include field hospital (DMAT) data. Because the DMAT field hospitals serve shelters, the situation report would be incomplete and likely biased without these data. Once NSSP provided DMAT data to the North Carolina DPH, these data were integrated with speed and ease and monitoring began immediately. DMAT data did not reveal major health events among shelter populations—still, DPH officials acquired a more representative picture of affected populations.
Improved situational awareness leads to thorough, better coordinated response efforts that could, potentially, discover vital public health issues. The DMAT data provided by NSSP gave DPH another piece of the surveillance puzzle and helped DPH take an important first step toward improving the state's disaster surveillance plan.
Now, whenever DMATs are deployed, data are available to the state through NSSP.
Lessons learned
Syndromic surveillance systems are inherently flexible and provide valuable situational awareness during natural disasters.
When Disaster Medical Assistance Teams (DMATs) are deployed, data are available in the NSSP to monitor public health issues among populations in shelters that might not be represented in other data streams.
Lessons learned from this experience include the following tips:
- Update emergency response plans to include the potential use of additional data streams, including DMAT data. Where possible, identify these data streams and points of contact.
- Work with the NSSP team before an event to prepare for the deployment and use of additional data streams.
Resources
Zachary Faigen, Enhanced Surveillance Epidemiologist
Division of Public Health, Communicable Disease Branch
North Carolina Department of Health and Human Services
zachary.faigen@dhhs.nc.gov
Centers for Disease Control and Prevention
Office of Public Health Data, Surveillance, and Technology
Detect and Monitor Division
www.cdc.gov/nssp
The findings and outcomes described in this syndromic success story are those of the authors and do not necessarily represent the official position of the National Syndromic Surveillance Program or the Centers for Disease Control and Prevention.