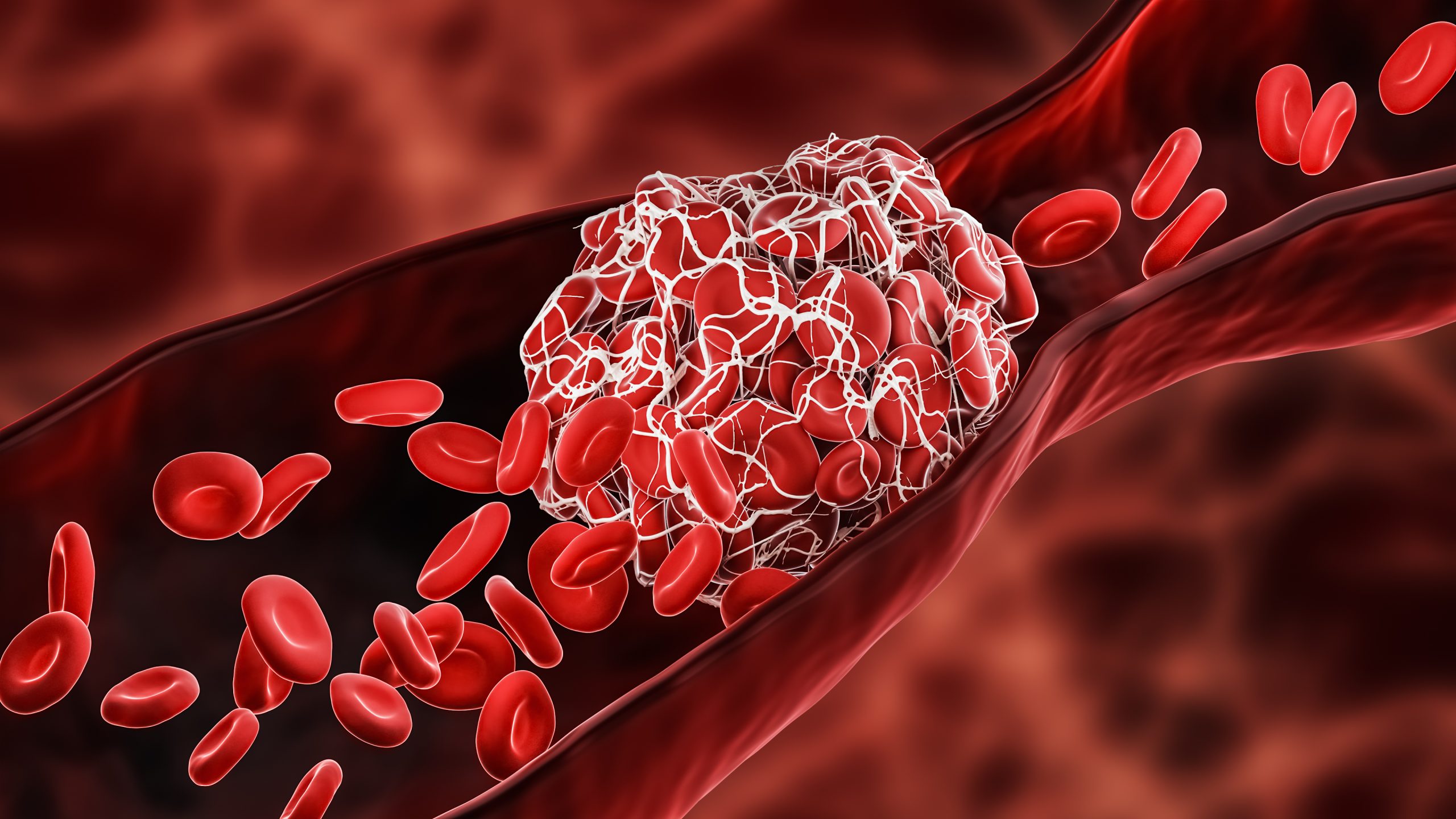
Learn about symptoms, risk factors, and treatment for deep vein thrombosis and pulmonary embolism.
Featured

Learn how blood clots are diagnosed and get information on testing and treatment options.
Learn about the factors that increase your risk for developing a blood clot
Learn about identifying, treating, and managing patients with venous thromboembolism.
View a collection of resources on blood clots.

Access shareable resources from the Stop the Clot, Spread the Word® Campaign.

Read stories from people who have had blood clots.