Progress Toward Poliomyelitis Eradication — Pakistan, January 2014–September 2015
, MD, PhD1; , MBBS2; , MD3; , MPH1; , DMD4; , MD2; , MPH1
Since Nigeria reported its last case of wild poliovirus type 1 (WPV1) in July 2014, Pakistan and Afghanistan remain the only two countries where WPV transmission has never been interrupted (1). This report describes actions taken and progress achieved toward polio eradication in Pakistan during January 2014–September 2015 and updates previous reports (2,3). A total of 38 WPV1 cases were reported in Pakistan during January–September 2015,* compared with 243 during the same period in 2014 (an 84% decline). Among WPV1 cases reported in 2015, 32 (84%) occurred in children aged <36 months, nine (32%) of whom had never received oral poliovirus vaccine (OPV). Twenty-six (68%) of the 38 reported cases occurred in the Federally Administered Tribal Areas (FATA) and Khyber Pakhtunkhwa (KPK) Province. During January–September 2015, WPV1 was detected in 20% (64 of 325) of environmental samples collected, compared with 34% (98 of 294) of samples collected during the same period in 2014. The quality and scope of polio eradication activities improved considerably following the establishment of a national Emergency Operations Center, which coordinated polio eradication partners' activities. All activities are following a National Polio Eradication Emergency Action Plan (4) that includes a rigorous action plan for the polio low transmission season (January−April). The presence of WPV1 in environmental samples in areas where no polio cases are detected highlights the need to improve surveillance for acute flaccid paralysis (AFP). Focused efforts to close remaining immunity gaps by locating, tracking, and vaccinating continually missed children and improving coverage with OPV through the routine vaccination program are needed to stop WPV transmission in Pakistan.
OPV Coverage and Immunization Activities
During 2014, national routine vaccination coverage of infants with 3 doses of oral poliovirus vaccine (OPV3) was estimated by the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) to be 72%,† unchanged from the 2013 estimate (3). Vaccination histories (from parental recall and immunization cards) for children aged 6–23 months with AFP who do not test positive for WPV are used to estimate OPV coverage in the target population. In 2014, national coverage was estimated to be 66% nationally (representing a decline of 7% from 71% in 2013), with considerable regional variation; estimated coverage was 18% in FATA, 35% in Balochistan, 58% in Sindh, 63% in KPK, and 83% in Punjab provinces.
During January 2014–October 2015, house-to-house supplementary immunization activities (SIAs)§ using mostly monovalent oral poliovirus vaccine type 1 (mOPV1) and bivalent type 1 and 3 OPV (bOPV) targeted children aged <5 years. Trivalent OPV (tOPV) (containing OPV types 1, 2, and 3) was used strategically to reduce the risk for circulating vaccine-derived poliovirus type 2 (cVDPV2) emergence. cVDPVs are vaccine viruses that have been excreted by vaccine recipients and have circulated in areas of low vaccine coverage for extended periods of time, eventually reverting to neurovirulence. To boost the population immunity to levels needed for interruption of WPV transmission, injectable inactivated poliovirus vaccine (IPV) has been used in 11 SIAs conducted at fixed immunization posts since November 2014, covering 1.7 million children in security-compromised areas of FATA, in high-risk Union Councils¶ of Karachi, and among internally displaced high-risk populations from FATA who are temporarily residing in areas surrounding FATA. One dose of IPV at age 14 weeks was progressively introduced into routine immunization services in areas of Punjab province during July 2015, and in Sindh province during September 2015. As part of the Global Polio Eradication Initiative End-Game Strategy, 1 dose of IPV is being introduced in all OPV-using countries to boost population immunity and prepare for the withdrawal of type 2 OPV (5).
The percentage of children with nonpolio AFP aged 6–23 months who had never received any routine or supplemental doses of OPV (zero-dose children) declined from 6.3% in 2014 to 2.1% in 2015, and the percentage who had received ≥4 OPV doses increased from 88% in 2014 to 96% in 2015. The highest percentage of zero-dose children was recorded in FATA during 2014 (46%) and in Balochistan during 2015 (12%). During June 2012–October 2014, FATA was mostly inaccessible during SIAs because of a ban on vaccinations by militant groups in North and South Waziristan. As previously inaccessible children left North Waziristan after the launch of military operations there in June 2014, they were vaccinated at strategically placed transit-area vaccination posts. With regained access in areas of FATA, the number of children who were inaccessible for SIAs during January–September 2015 was estimated to be <35,000, decreasing from >250,000 during 2014, and the percentage of zero-dose children among nonpolio AFP cases in FATA declined from 38% in 2014 to 8% in 2015.
Efforts to improve vaccination coverage in high-risk areas in 2015 included the establishing a network of Female Community Volunteers in Karachi and North Sindh, adopting Continuous Community Protected Vaccinations,** conducting health camps that provide a range of public health services in addition to vaccinations in 12 districts where poliovirus continues to circulate (Tier 1 districts), and expanding vaccination by permanent teams placed in key transit points to vaccinate children as they enter and leave reservoir areas (permanent transit points). Approximately 2,000 health camps were conducted in the highest risk areas of FATA, Karachi, and KPK, during which >500,000 children (including 10,000 zero-dose children) received OPV.
Surveillance Activities
AFP surveillance. In 2014, the annual nonpolio AFP rate†† per 100,000 population aged <15 years was 6.2 nationally, ranging from 1.4–13.7 among the eight provinces and regions of Pakistan. The percentage of AFP cases for which adequate stool specimens were collected was 88% (range = 80%–92%) (Table). Despite these overall high AFP surveillance performance indicators in Pakistan, field reviews of AFP surveillance conducted in 67 districts during January−August 2015 detected gaps in surveillance quality (nonpolio AFP rates and adequate stool collection rates below target)§§ at the sub-district level.
Environmental surveillance. Environmental surveillance supplements AFP surveillance through periodic testing of sewage samples for polioviruses. During January 2014–October 2015, a total of 615 sewage samples from 37 sampling sites were tested for polioviruses. During January–September 2015, WPV1 was detected in 20% (64 of 325) of environmental samples from 37 sampling sites, compared with 34% (98 of 294) of samples collected from 30 sites during the same period in 2014. During January–March 2015, cVDPV2 was detected in samples collected in Sindh, and ambiguous VDPV (aVDPV2) (vaccine-derived polioviruses that are either isolated from persons with no known immunodeficiency or isolated from sewage with the ultimate source unknown) was detected in subsequent specimens from Sindh KPK, and Punjab through September 2015.
WPV and cVDPV Epidemiology
During 2014, 306 WPV1 cases were reported in Pakistan, compared with 93 cases in 2013; as of October 23, 2015, a total of 38 WPV1 cases had been reported during January–September 2015, compared with 243 cases reported during the same period in 2014 (Table) (Figures 1 and 2). Among the 306 polio cases reported in 2014, 56% were in zero-dose children. Among the 38 WPV1 cases reported in 2015, 11 (29%) were in zero-dose children; 32 (84%) of the 2015 cases were reported in children aged <23 months.
During January–September, 2015, WPV1 was detected in 17 districts, compared with 32 districts during the same period in 2014. Among the 38 WPV1 cases reported during 2015, 15 (40%) were reported from KPK, 11 (30%) from FATA, six (16%) from Balochistan, five (13%) from Sindh, and one from Punjab. The most recent case was reported from KPK, with an onset date of September 16. Although the number of cases declined compared with 2014, the percentage of orphan viruses (wild-type polioviruses that are >1.5% genetically divergent in the VP1 region from the most closely related isolate, indicating low AFP surveillance sensitivity) isolated during the first half of 2015 increased from 6% to 14%, compared with the first half of 2014. Genetic sequencing data further indicate that, in 2015, WPV1 has persisted in known sanctuaries (Quetta and Karachi) and has been shared across these sanctuaries and across the borders with Afghanistan. Reporting of cVDPV2 decreased considerably during 2014, with 22 cases reported, compared with 48 during 2013. Two cVDPV2 cases were reported during February 2015, and aVDPV2 was isolated from two persons with AFP and from environmental samples. The last WPV3 case in Pakistan was reported from FATA in 2012.
Discussion
During January–September 2015, the number of reported polio cases and WPV1 isolates detected from environmental samples sharply declined compared with the same period in 2014. This might reflect expected low incidence following the high incidence seen in 2014 (1), but the decline also followed the launch and rigorous implementation of a plan to intensify polio eradication activities during January–April 2015, the low transmission season. The increase in cases during 2014 compared with 2013 was caused mainly by the outbreak in North Waziristan, an area that remained inaccessible during SIAs until June 2014, as well as by the population influx from FATA into surrounding areas following military operations in North Waziristan and the subsequent appearance of cases and positive environmental samples in previously unaffected areas; however, to date in 2015, spread in these areas has been limited.
AFP and environmental surveillance data suggest that the intensity of WPV1 transmission during 2015 has been restricted to high-risk areas of KPK (Peshawar), FATA (Khyber), Sindh (Karachi), Balochistan (Quetta and Killa Abdullah), and central Pakistan (Jacobabad). However, continued detection of WPV1 in environmental samples, reporting of a case with date of onset on September 11 in Punjab, and isolation of cVDPV from AFP cases in FATA and KPK and from environmental samples in Karachi and Quetta indicate immunity gaps and circulation of poliovirus in wide geographic areas in Pakistan.
In 2015, most areas of Pakistan have been accessible during SIAs, apart from small pockets of FATA (in parts of Khyber and North and South Waziristan); however, lack of access because of insecurity is not the main reason that children are missed during SIAs. The majority are missed because of poor-quality SIAs, related to inadequate microplanning, poor supervision and monitoring, and failure to sufficiently train and motivate field supervisors and vaccinators. As part of the low transmission season plan, vaccinators received comprehensive training, and microplans were extensively revised. A strategic shift from tracking "covered children" to tracking "continually missed children" has been implemented. Identifying children at high risk for being missed through improved microplanning and postcampaign assessments needs to continue and be expanded. In addition, because of continued WPV circulation in Afghanistan, attention needs to be focused on border crossings between Afghanistan and Pakistan.
Polio eradication efforts are led by the Prime Minister's Task Force for Polio Eradication. Government ownership and commitment, strategic coordination among partners, and systematic approaches to addressing programmatic challenges are critical factors in achieving polio eradication in Pakistan. Pakistan's Emergency Operations Center has played a vital role in streamlining communications between government officials and Global Polio Eradication Initiative partners by enabling timely data sharing and decision making. Continued government leadership along with innovative methods of tracking and vaccinating missed children are key to the success of polio eradication efforts in Pakistan.
Acknowledgments
Becky Maholland, Office of Public Health Preparedness and Response, CDC; Tahir Malik, World Health Organization (WHO) Country Office, Islamabad, Pakistan; National Stop Transmission of Polio and Field Epidemiology and Laboratory Training Program, Pakistan; WHO Eastern Mediterranean Regional Office, Amman, Jordan; WHO Regional Reference Laboratory for Poliovirus, Islamabad, Pakistan; WHO Global Polio Laboratory Network; Polio Eradication Department, WHO, Geneva, Switzerland.
1Global Immunizations Division, Center for Global Health, CDC; 2World Health Organization, Geneva Switzerland; 3Pakistan Ministry of Health; 4Emory University, Atlanta, Georgia.
Corresponding author: Noha H. Farag, nfarag@cdc.gov, 404-368-8498.
References
- Hagan JE, Wassilak SG, Craig AS, et al. Progress toward polio eradication—worldwide, 2014–2015. MMWR Morb Mortal Wkly Rep 2015;64:527–31.
- Farag NH, Alexander J, Hadler S, et al. Progress toward poliomyelitis eradication—Afghanistan and Pakistan, January 2013–August 2014. MMWR Morb Mortal Wkly Rep 2014;63:973–7.
- Progress toward poliomyelitis eradication—Pakistan, January 2012–September 2013. MMWR Morb Mortal Wkly Rep 2013;62:934–8.
- Government of Islamic Republic of Pakistan. National emergency action plan for polio eradication 2015–2016. Islamabad, Pakistan: Government of Islamic Republic of Pakistan; 2015. Available at http://reliefweb.int/sites/reliefweb.int/files/resources/Final-pakistan-NEAP2015-16.pdf.
- Immunization Systems Management Group of the Global Polio Eradication Initiative. Introduction of inactivated poliovirus vaccine and switch from trivalent to bivalent oral poliovirus vaccine—worldwide, 2013–2016. MMWR Morb Mortal Wkly Rep 2015;64:699–702.
* Cases during January–September 2015 reported as of October 23, 2015.
† Additional information available at http://apps.who.int/immunization_monitoring/globalsummary.
§ Mass campaigns conducted for a brief period (days to weeks) in which 1 dose of OPV is administered to all children aged <5 years, regardless of vaccination history. Campaigns can be conducted nationally or in sections of the country.
¶ Union Councils are administrative units below the district level.
** Continuous Community Protected Vaccinations is a mechanism used to increase vaccination coverage by recruiting and training volunteers from the local community to provide house-to-house vaccinations continually throughout the year.
†† Vaccination histories of children aged 6–23 months with AFP who do not test WPV-positive are used to estimate OPV coverage of the overall target population and to corroborate national reported routine vaccination coverage estimates.
§§ The quality of AFP surveillance is monitored by performance indicators that include 1) the detection rate of nonpolio AFP cases and 2) the percentage of AFP cases with adequate stool specimens. WHO operational targets for countries with endemic poliovirus transmission are an nonpolio AFP detection rate of ≥2 cases per 100,000 population aged <15 years and adequate stool specimen collection from ≥80% of AFP cases (two stool specimens collected ≥24 hours apart, both within 14 days of paralysis onset, and shipped on ice or frozen packs to a WHO-accredited laboratory, arriving in good condition [i.e., without leaking or desiccation]).
Summary
What is already known on this topic?
Pakistan remains one of two countries, along with Afghanistan, where indigenous wild poliovirus (WPV) transmission has never been interrupted. Conflict and programmatic issues in both countries have resulted in pockets of missed children during immunization campaigns.
What is added by this report?
The number and geographic spread of WPV type 1 cases have decreased during January–September 2015, compared with the same period during 2013 and 2014. However, gaps in campaign performance and surveillance, evidenced by the persistence of continually missed children and the detection of wild viruses in environmental samples and orphan viruses isolated from cases and environmental samples are indicative of ongoing program challenges.
What are the implications for public health practice?
Continuing poliovirus transmission in Pakistan poses a serious challenge to the achievement of global polio eradication. To achieve the goal of ending poliovirus transmission in Pakistan in 2016, continued government leadership of the polio eradication program and further improvements in campaign quality are needed to reach and vaccinate all children.
FIGURE 1. Number of cases of wild poliovirus types 1 (WPV1) and 3 (WPV3) and circulating vaccine-derived poliovirus type 2 (cVDPV2), by month — Pakistan, 2012–2015
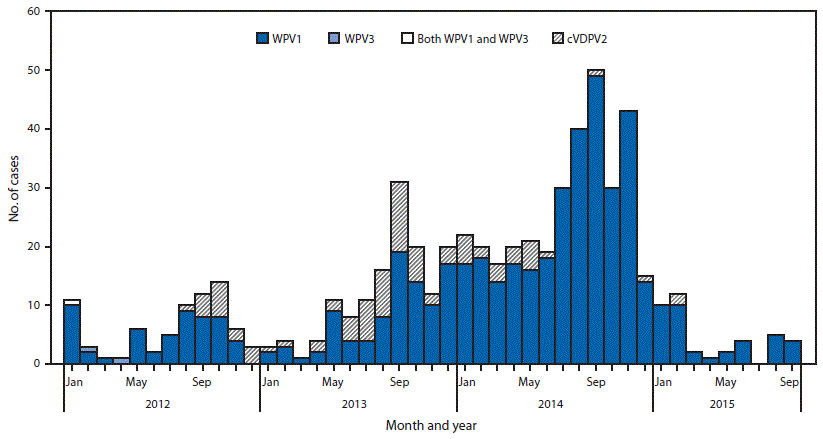
Alternate Text: The figure above is an epidemiologic curve showing the number of cases of wild poliovirus types 1 and 3 and circulating vaccine-derived poliovirus type 2, by month, in Pakistan during 2012–2015.
FIGURE 2. Location of cases of wild poliovirus type 1 (WPV1) and circulating vaccine-derived poliovirus type 2 (cVDPV2), by period — Pakistan, January 2014–September 2015
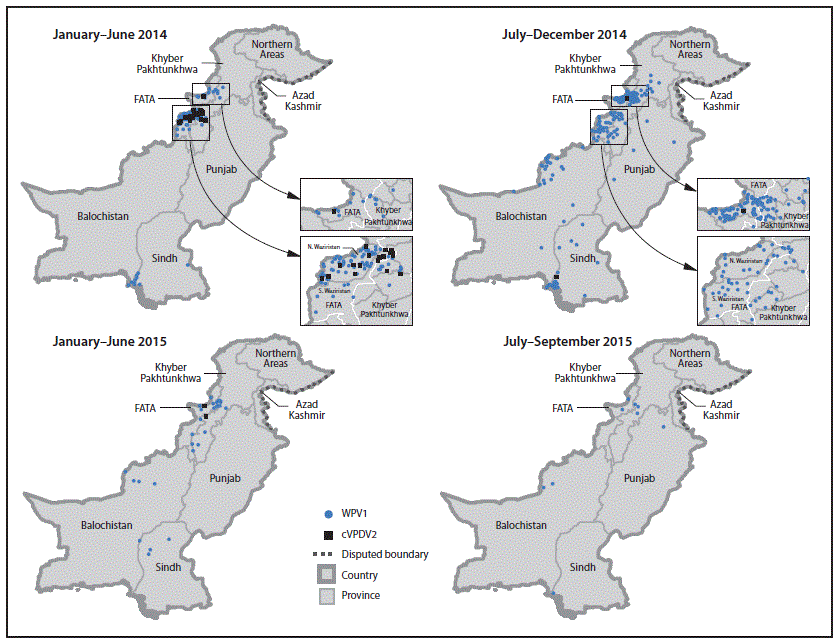
Abbreviation: FATA = Federally Administered Tribal Areas.
Alternate Text: The figure above is a map showing the location of cases of wild poliovirus type 1 and circulating vaccine-derived poliovirus type 2, by period, in Pakistan during January 2014–September 2015.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
