Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Mycoplasma pneumoniae Respiratory Illness — Two Rural Counties, West Virginia, 2011
On October 28, 2011, the West Virginia Department of Health and Human Resources notified CDC of an increase in pneumonia cases among school-aged children in two rural counties. Mycoplasma pneumoniae was the suspected cause, based on epidemiology, clinical presentation, and testing of specimens sent to CDC. Three of six nasopharyngeal swabs were positive for M. pneumoniae in testing by quantitative real-time polymerase chain reaction (qPCR). The West Virginia Department of Health and Human Resources and CDC conducted an outbreak investigation to confirm the etiology of the outbreak, establish active case surveillance, and provide recommendations for treatment and containment. The investigation confirmed M. pneumoniae as the cause and identified 125 cases, including two caused by macrolide-resistant isolates. The outbreak was contained with public health interventions that included communicating to the public the importance of respiratory hygiene, providing hand sanitizer in schools, and informing health-care providers about macrolide resistance; antibiotic prophylaxis was not used. Despite the large number of cases and macrolide-resistant strains, no severe extrapulmonary manifestations (e.g., erythema multiforme) were reported.
M. pneumoniae, transmitted through respiratory droplets, is a common cause of acute upper and lower respiratory infections in children and young adults. An estimated 2 million infections are caused by M. pneumoniae each year in the United States; radiologically confirmed pneumonia is noted in 3%–10% of cases. In rare cases, extrapulmonary manifestations occur (1). Pneumonia caused by M. pneumoniae has an incubation period of 3 weeks; outbreaks can be prolonged (1–3). For treatment, macrolides and tetracyclines are first-line antibiotics. In this outbreak, possible cases were defined as Mycoplasma-like illness, with cough lasting ≥3 days and fever ≥100.0°F (≥37.8°C), with symptom onset on or after August 26, 2011 (the start of the school year) in a resident of Gilmer County or Calhoun County. Probable cases were defined as Mycoplasma-like illness with radiologically confirmed pneumonia (a positive chest radiograph reading by a local medical provider). Confirmed cases were defined as Mycoplasma-like illness with M. pneumoniae detected in nasopharyngeal or oropharyngeal swabs by qPCR, with or without radiologically confirmed pneumonia.
Beginning November 16, 2011, active surveillance was conducted in all elementary, middle, and high schools and all primary-care clinics and emergency departments in the two counties. In clinics, providers obtained nasopharyngeal and oropharyngeal swabs from patients with Mycoplasma-like illness and referred them to local health departments for questionnaire administration. In schools, officials reported acutely ill students to local health departments for screening and questionnaire administration and referred them to clinics for swab collection. In addtion, to identify cases with symptom onset before surveillance began, medical records from health-care providers were searched for possible pneumonia cases, which were followed up by telephone.
Swabs were placed in viral or universal transport medium and sent to CDC for culture and M. pneumoniae testing using qPCR. Mycoplasma isolates and specimens with sufficient M. pneumoniae nucleic acid were tested for macrolide resistance by qPCR, followed by high-resolution melt analysis for mutations in the 23S rRNA associated with macrolide resistance (4). Each specimen also was tested for 29 additional respiratory pathogens with qPCR technology used for research (5). Patients with confirmed M. pneumoniae were invited for follow-up oropharyngeal swab collection at least 5 days after completion of antibiotic therapy (or initial specimen collection, if no antibiotics were taken) to assess for persistence of the organism and development of antibiotic resistance. Active surveillance was discontinued December 8 at clinics and December 22 at schools. The last case was identified on December 14, 2011.
During August 29–December 14, a total of 125 cases were identified, including 23 confirmed, 39 probable, and 63 possible cases (Table 1). Of the 125 cases, 43 (34%) had specimens tested for M. pneumoniae by qPCR, and 23 (53%) of those tested were positive. Sixty-nine (55%) of 125 cases had chest imaging performed, and 48 chest radiographs (70%) showed infiltrates consistent with pneumonia. The median age of patients was 10.2 years (range: 0–65.3 years); 68% lived in Gilmer County. The earliest symptom onset date was August 29, although most patients became ill from late October to mid-November (Figure). In addition to fever and cough, common symptoms included sore throat (57%), chills (55%), and muscle aches (54%) (Table 1). No extrapulmonary manifestations or fatalities occurred. Seven (6%) patients were hospitalized; none of the seven required intensive care. Among patients, 92 (79%) were treated with macrolide antibiotics. Eighty-three patients (70%) attended or worked at schools. Among those who did not, 55% had household contacts attending or working at schools (Table 1). All eight schools in the two counties were affected. The mean illness attack rate among students in the four schools in Gilmer County was 5.2% (range: 3.5%–8.0%), and the mean attack rate among students in the three schools in Calhoun County was 3.6% (range: 1.5%–7.7%).
Other than M. pneumoniae, no other primary causative pathogens were detected among the 43 persons with qPCR. Eleven (47%) laboratory-confirmed cases yielded sufficient M. pneumoniae nucleic acid for macrolide resistance testing; two (18%) of the cases were resistant (Table 2). Follow-up specimens were collected in 10 laboratory-confirmed cases. Seven tests were negative for M. pneumoniae, two remained positive, and one had an indeterminate result. Among the persistently positive patients, one had never taken antibiotics; the second had a resistant strain according to the first swab, collected more than 2 months after receipt of azithromycin. Six of the seven follow-up negative results were for patients who had taken antibiotics, one of whom had an initially resistant strain; in addition to a macrolide, this patient received doxycycline before the follow-up swab. The follow-up indeterminate case occurred in a patient who had taken azithromycin.
To contain the outbreak, hand sanitizer was made widely available in schools. Letters about hand hygiene, respiratory hygiene (e.g., cough etiquette, social distancing, and staying home when ill), and M. pneumoniae were sent to parents in both counties in November. The Gilmer County Health Department also issued press releases regarding hand and respiratory hygiene on November 3 and 16. Prompt treatment of suspected cases was encouraged, and doxycycline was recommended for patients with persistent symptoms, given circulating resistant strains. Widespread antibiotic prophylaxis was not implemented because convincing evidence of antibiotic effectiveness during outbreaks has not been shown; schools in the two counties were closed November 19–27 for the usual Thanksgiving break. The number of new cases decreased in early December, and active surveillance was discontinued by health-care providers on December 8 and at schools on December 22, before the winter break.
Reported by
Leann Newell, Minnie Hamilton Health System. Patrick Burke, MPH, Jessica Woods, Mid-Ohio Valley Health Dept. Robert Posey, Lewis County Health Dept. Brenda Smith, Gilmer County Health Dept. Sherif M. Ibrahim, MD, Danae Bixler, MD, Loretta Haddy, PhD, Thein Shwe, MPH, Rachel Radcliffe, DVM, West Virginia Bur for Public Health. Al Benitez, Kathy Thurman, MS, Maureen H. Diaz, PhD, Bernard J. Wolff, Agnes Warner, Jonas M. Winchell, PhD, Laura Conklin, MD, Div of Bacterial Diseases, National Center For Immunization and Respiratory Diseases; Kamil Barbour, PhD, Katherine E. Fleming-Dutra, MD, Laura C. Steinhardt, PhD, EIS officers, CDC. Corresponding contributor: Laura C. Steinhardt, lsteinhardt@cdc.gov, 404-718-4794.
Editorial Note
Because M. pneumoniae is not part of normal human pharyngeal flora, its detection in nasopharyngeal or oropharyngeal specimens in persons with compatible clinical illness indicates that M. pneumoniae is the etiologic agent (1). Estimates indicate that up to 40% of community-acquired pneumonia is caused by M. pneumoniae (1). In this investigation, the high percentage of M. pneumoniae–positive specimens among all cases (53%) and among pneumonia cases (70%), and the lack of other causative pathogens detected by qPCR strongly suggest that M. pneumoniae caused the outbreak of acute respiratory illness in Gilmer and Calhoun counties.
Transmission of M. pneumoniae in this outbreak likely occurred in schools, homes, and within the general community. Similar school-based outbreaks of M. pneumoniae have been described previously (3,6), with attack rates of pneumonia ranging from 1.8% to 6.4% (3). Transmission of M. pneumoniae outside schools also has been documented in previous outbreaks (2,3). In this outbreak, although 70% of patients were students or school employees, cases were not centered in one school and occurred among persons both with and without contact with students or school employees.
Two (18%) of 11 specimens tested were resistant to macrolides. Previous outbreaks in Missouri and Rhode Island have reported macrolide resistance in 8% and 27% of isolates, respectively (3,7). More widespread macrolide resistance has been reported in Europe and Asia. Because M. pneumoniae is not routinely isolated in the United States, the prevalence of macrolide resistance and its implications for clinical outcome remain unknown (4,7). Although M. pneumoniae can cause severe disease and extrapulmonary manifestations, the illnesses in this outbreak were relatively mild despite macrolide resistance.
M. pneumoniae outbreaks present challenges because data on effective control measures are lacking. Given transmission via respiratory droplets, control depends on hand and respiratory hygiene and appropriate identification and treatment of cases. Antibiotic prophylaxis has been used as an outbreak control measure in closed settings (8,9) and in settings with severe disease (3). Nonetheless, the role of prophylaxis in M. pneumoniae community outbreaks is not clear because of a lack of data on its effectiveness. The potential benefits of prophylaxis must be balanced with the potential for adverse health effects and induction of macrolide resistance (3,8).
Although this M. pneumoniae outbreak had a relatively mild spectrum of illness, its size and multiple transmission settings warranted aggressive public health interventions targeting homes, schools, and clinics. Awareness of circulating macrolide-sensitive and resistant M. pneumoniae strains made these measures even more crucial because macrolide prophylaxis might not have been effective. Because M. pneumoniae is difficult to culture and resistance testing is not available routinely, antibiotic sensitivity of the circulating strain is usually unknown. This outbreak highlights the importance of considering macrolide resistance in directing treatment protocols during M. pneumoniae outbreaks and demonstrates that prompt implementation of public health measures can mitigate transmission regardless of strain resistance.
References
- Waites KB,Talkington DF. Mycoplasma pneumoniae and its role as a human pathogen. Clin Microbiol Rev 2004;17:697–728.
- Foy HM. Grayston JT, Kenny GE, Alexander ER, McMahan R. Epidemiology of Mycoplasma pneumoniae infection in families. JAMA 1966;197:859–66.
- Walter ND, Grant GB, Bandy U, et al, Community outbreak of Mycoplasma pneumoniae infection: school-based cluster of neurologic disease associated with household transmission of respiratory illness. J Infect Dis 2008;198:1365–74.
- Wolff BJ, Thacker WL, Schwartz SB, Winchell JM. Detection of macrolide resistance in Mycoplasma pneumoniae by real-time PCR and high-resolution melt analysis. Antimicrob Agents Chemother 2008;52:3542–9.
- Kodani M, Yang G, Conklin LM, et al. Application of TaqMan low-density arrays for simultaneous detection of multiple respiratory pathogens. J Clin Microbiol 2011;49:2175–82.
- Dominguez A, Minguell S, Torres J, Serrano A, Vidal J, Salleras L. Community outbreak of acute respiratory infection by Mycoplasma pneumoniae. Eur J Epidemiol 1996;12:131–4.
- Yamada M, Buller R, Bledsoe S, Storch GA. Rising rates of macrolide-resistant Mycoplasma pneumoniae in the central United States. Pediatr Infect Dis J 2012;31:409–11.
- Hyde TB, Gilbert M, Schwartz SB, et al. Azithromycin prophylaxis during a hospital outbreak of Mycoplasma pneumoniae pneumonia. J Infect Dis 2001;183:907–12.
- Klausner JD, Passaro D, Rosenberg J, et al. Enhanced control of an outbreak of Mycoplasma pneumoniae pneumonia with azithromycin prophylaxis. J Infect Dis 1998;177:161–6.
What is already known on this topic?
Mycoplasma pneumoniae is a common cause of acute respiratory infections in children and young adults and might cause up to 40% of community-acquired pneumonia. Macrolide antibiotics are the first-line treatment for M. pneumoniae infections, although resistance to macrolides has been documented.
What is added by this report?
During August 29–December 14, 2011, a total of 125 cases of Mycoplasma respiratory illness were identified in two rural counties of West Virginia. No severe manifestations or deaths occurred. Two (18%) of 11 laboratory-confirmed cases that were tested were resistant to macrolides. Most patients (70%) attended or worked at schools. The outbreak subsided after implementation of standard public health measures, including communicating respiratory hygiene guidance to the public, providing hand sanitizers in schools, and informing health-care providers about macrolide resistance; antibiotic prophylaxis was not implemented.
What are the implications for public health practice?
Although this M. pneumoniae outbreak had a relatively mild spectrum of illness, its size and multiple transmission settings warranted aggressive public health interventions targeting homes, schools, and clinics. This outbreak also highlights the importance of considering macrolide resistance (for which testing is not performed routinely) during M. pneumoniae outbreaks to direct treatment protocols. Despite the presence of resistant strains, Mycoplasma transmission declined with prompt implementation of public health measures.
FIGURE. Confirmed, probable, and possible cases* of Mycoplasma pneumoniae respiratory illness, by date of symptom onset — Gilmer and Calhoun counties, West Virginia, 2011
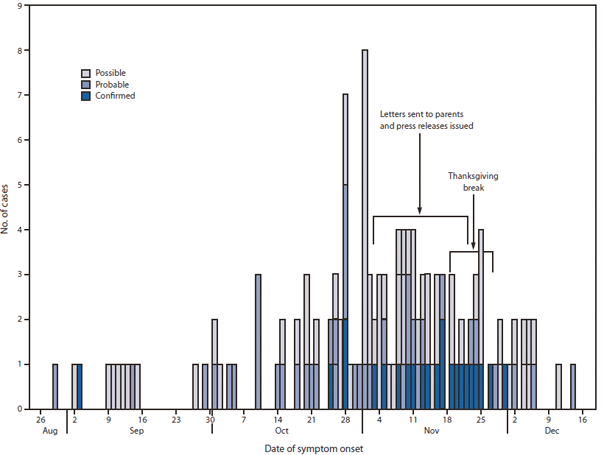
* Possible cases were defined as Mycoplasma-like illness with cough lasting ≥3 days and fever of ≥100.0°F (37.8°C), with symptom onset on or after August 26, 2011. Probable cases were Mycoplasma-like illness with radiologically confirmed pneumonia. Confirmed cases were Mycoplasma-like illness with M. pneumoniae detected by real-time polymerase chain reaction, with or without radiologically confirmed pneumonia.
Alternate Text: The figure above shows confirmed, probable, and possible cases of Mycoplasma pneumoniae respiratory illness, by date of symptom onset in West Virginia's Gilmer and Calhoun counties during an outbreak in 2011. During August 29-December 14, a total of 125 cases were identified, including 23 confirmed, 39 probable, and 63 pos¬sible cases. Most patients became ill from late October to mid-November.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
