FIGURE. Number, drug use, and arrival times of rave attendees transported to emergency departments (N = 30)* --- Los Angeles County, California, December 31, 2009--January 1, 2010
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Ecstasy Overdoses at a New Year's Eve Rave --- Los Angeles, California, 2010
Ecstasy (3,4-methylenedioxymethamphetamine [MDMA]) is an illegal synthetic amphetamine used as a stimulant and hallucinogen (1--3). On January 4, 2010, the Los Angeles County (LAC) Department of Public Health (DPH) learned of six MDMA-related emergency department (ED) visits and one death, all linked to a New Year's Eve event attended by approximately 45,000 persons. LAC DPH conducted an investigation to search for additional MDMA-related ED visits, characterize the cases, and determine whether drug contamination was involved. This report summarizes the results of the investigation, which determined that 18 patients visited EDs in LAC for MDMA-related illness within 12 hours of the rave. All were aged 16--34 years, and nine were female. In addition to using MDMA, 10 of the 18 had used alcohol, and five had used other drugs. Three patients were admitted to the hospital, including one to intensive care. A tablet obtained from one of the patients contained MDMA and caffeine, without known toxic contaminants. The cluster of apparent ecstasy overdoses occurred in the context of likely increasing MDMA use in the county during 2005--2009, as indicated by increased identification of MDMA-containing forensic specimens and a large increase in LAC residents entering drug treatment programs for MDMA. Collaboration between public health, police, fire, and emergency medical service (EMS) officials on a comprehensive prevention strategy might reduce the number of overdoses at similar events.
A rave is an all-night dance party with electronic music. When raves first emerged in the late 1980s, they were underground parties usually held at abandoned warehouses and outdoor sites. Since then, raves have become organized commercial events staged by promoters at established venues, often with high ticket prices and elaborate laser light effects. The rave in LAC, which has been staged annually since 1998, was held on New Year's Eve, December 31, 2009--January 1, 2010, at a rented public facility jointly owned by the city of Los Angeles, LAC, and the state of California. Admission was restricted to persons with identification indicating they were aged ≥18 years. Approximately 45,000 persons attended the event, which featured music on three stages from 6 p.m. on December 31, 2009, until 4 a.m. on January 1, 2010. Alcohol was for sale to persons aged ≥21 years. Los Angeles Police Department (LAPD) police officers, undercover narcotics officers, roving EMS technicians, and 14 ambulances were stationed on-site. Local EDs had been notified in advance by LAC EMS to possibly expect patients from the rave.
A physician on staff at a hospital located near the event reported a cluster of six apparent ecstasy overdoses to an LAC DPH physician on January 4. That same day, LAC DPH investigators reviewed routine public health surveillance of unusual deaths and noted the death at home on January 1 of a previously healthy man aged 24 years who had attended the same rave. Investigators then conducted interviews with the event facility manager; fire, EMS, and police officials; the on-site incident commander; the coroner; the California Poison Control System medical director; and relatives and friends of the person who died at home after attending the rave. Investigators also reviewed ED records on the six patients initially reported at the ED and interviewed the one patient hospitalized in the intensive-care unit (ICU). They also requested a list of patients transported from the rave to surrounding hospitals and cross-checked this list with records from Los Angeles Fire Department ambulances and private ambulance companies. To identify additional patients who were not transported by ambulance, investigators queried the LAC DPH electronic ED syndromic surveillance system for patients on December 31 and January 1 with a chief complaint that included the keywords "rave," "overdose," "OD," "XTC," or "ecstasy."
An MDMA-associated ED visit was defined as a visit by a person with documented attendance at the rave who was transported to an ED within 12 hours of the end of the event and who had used MDMA. MDMA use was defined as self-reported use, a urine toxicology test positive for amphetamine, or a serum toxicology test positive for MDMA.
The investigation identified ED medical records for 30 patients who had attended the rave. One patient was transported for trauma, and the other 29 for various drug and/or alcohol intoxications. Patients began to arrive at EDs shortly after the rave began (Figure). All but one patient arrived within 2 hours of the end of the rave; the one patient had taken additional ecstasy at home after the event. Eighteen patients had MDMA exposure and met the case definition, 16 by self-reported MDMA use (12 confirmed by toxicology testing) and two by toxicology testing alone. Cases were predominantly in young adults, ranging in age from 16 to 34 years (mean: 21.3 years); 10 cases were in persons aged <21 years, and one was in a person aged <18 years (Table). Thirteen also had used alcohol or other drugs, including marijuana and prescription medications. For the six patients (three of whom were aged <21 years) with available serum alcohol levels, the mean blood alcohol concentration was 0.31 g/dL (range: 0.19 g/dL--0.33 g/dL).
Clinical findings among the 18 patients with MDMA exposure were consistent with MDMA use (1,4), including agitation, hypertension, mydriasis, and tachycardia (Table). Fifteen of the patients were treated and released. Three were admitted. Two were treated for 2 and 4 days, respectively, and discharged in good condition. One patient was admitted to the ICU with seizure, rhabdomyolysis, renal failure requiring hemodialysis, and hepatic failure; he was discharged to home outpatient hemodialysis after a 28-day hospital stay.
The patient who died at home did not meet the case definition because he was medically unattended and his death occurred ≥12 hours after the rave. The coroner determined that the cause of death was multiple drug intoxication. Friends reported that the decedent had used ecstasy and cocaine at the rave and injected heroin at home afterward. Toxicology testing at autopsy revealed MDMA, cocaine, and heroin. Family members stated that the decedent was previously in good health, and no underlying chronic medical conditions were discovered at autopsy.
Of the eight patients who described the amount of ecstasy used, seven reported ingesting at least two tablets (range: 1--6 tablets). The ingested tablets had no common color or impressed design. The Drug Enforcement Administration's forensic laboratory identified two major components in an ecstasy tablet obtained from the ICU patient, including MDMA and caffeine in nearly equal proportions, and a minor amount of N-methylphthalimide (<5% of total tablet mass). Although no other ecstasy tablets linked to the patients were available for analysis, five ecstasy tablets seized by LAPD narcotics officers during separate arrests at the rave all were confirmed to contain MDMA.
To assess trends in LAC for MDMA use during 2005--2009, investigators reviewed data from the LAC laboratories in the National Forensic Laboratory Information System (NFLIS) and found that MDMA-containing specimens submitted increased annually from 5.2 to 13.4 per 100,000 LAC residents during this period. The Los Angeles County Participant Reporting System of drug abuse treatment statistics reported that the number of LAC residents citing MDMA as their primary drug of choice at the time of entry into drug treatment increased by 650%, from 0.22 to 1.65 per 100,000 LAC residents, during 2005--2009.
Reported by
L Mascola, MD, D Dassey, MD, Acute Communicable Disease Control Program; S Fogleman, MSN, MPH, Toxics Epidemiology Program, Los Angeles County Dept of Public Health, California; L Paulozzi, MD, National Center for Injury Prevention and Control; CG Reed, MD, EIS Officer, CDC.
Editorial Note
Although previous reports (5--7) have documented widespread use of MDMA and other "club drugs" at raves since the early 1990s, this is the first known public health investigation describing the epidemiology of a cluster of MDMA-related ED visits associated with a rave. Notably, according to LAC DPH records, no MDMA-related ED visits are known to have occurred after previous New Year's Eve raves in the county. However, MDMA-related ED visits are not routinely reportable to LAC DPH. This cluster occurred in the setting of a likely overall increase in ecstasy use in LAC during 2005--2009, indicating a possible ongoing and underreported public health problem.
MDMA overdose, rather than drug contamination, likely accounted for the symptoms requiring ED visits among rave attendees. This conclusion is supported, in part, by the lack of a common description of the ecstasy tablets ingested by patients and the finding of MDMA, but no known toxic contaminants, in the ecstasy tablet from one of the patients. In addition, these cases resembled other MDMA-related cases demographically and clinically (1,4,8). One of the patients described in this report was critically ill with multiorgan failure. Severe MDMA-related illness, including hyperthermia, seizure, metabolic disturbances, rhabdomyolysis, renal and hepatic failure, cardiac dysrhythmias, hemorrhagic stroke, and cerebral edema, is well described in the literature and can result in death (1--3).
Less than 6 months after the rave described in this report, news media reported ecstasy overdoses resulting in two deaths and at least five critical illnesses among attendees at a May 29, 2010 rave in the San Francisco Bay area. Nationally, MDMA-related ED visits increased 74.8% during 2004--2008 (8). A recent national survey of teenagers found an increase in use of MDMA in 2009 compared with 2008, and an accompanying decrease in perception of risk for the drug (9). Decreased risk perception might contribute to the observed increases in ecstasy use. Targeting rave attendees with messages that increase risk perception might help to prevent ecstasy overdoses.
The findings in this report are subject to at least three limitations. First, histories of ecstasy use might be inaccurate; illicit drugs might not contain MDMA as purported, or might contain other compounds in addition to MDMA. Second, toxicology testing was not performed in four cases, and urine toxicology testing for amphetamines is not specific for MDMA. This could result in misclassification of the exposure. Finally, among the cases investigated, only one ecstasy tablet was available for analysis.
Drug overdose is a preventable injury that has become an increasing public health concern (10). Effective, culturally appropriate overdose prevention strategies that can be used at raves and other large public gatherings are needed. ED and EMS records might be useful tools for identifying clusters of drug-related emergencies. Health-care professionals should be encouraged to report clusters of suspected drug overdose or contamination. Cooperative efforts among public health, EMS, law enforcement, and substance-abuse treatment services providers are useful in determining current patterns of drug use in a community. Similar collaborations could be used to develop multiagency overdose prevention plans for raves and other mass gatherings. Finally, city and county managers and elected officials should be aware of the potential health risks and costs associated with making publicly owned facilities available for large commercial events such as raves.
Acknowledgments
The findings in this report are based, in part, on contributions by C Gastelum, MD, White Memorial Medical Center; B Hwang, MD, D Diamond, MD, B Lee, PhD, C Nagy, MPH, C Rangan, MD, M Santos, Los Angeles County Dept of Public Health; K Douglass, Los Angeles Fire Dept; C Will, MS, Los Angeles Police Dept Scientific Investigation Div, Narcotics Unit; C Chidester, MSN, S Raby, Los Angeles County Emergency Medical Svcs Agency; R Hays, Los Angeles County Dept of Coroner; R Geller, MD, California Poison Control; J Comparin, L Wong, S Oulton, D Kirby, Drug Enforcement Admin; J Peaco, Federal Bur of Investigation; D Bensyl, PhD, Scientific Education and Professional Development Program Office (proposed), and S Vagi, PhD, National Center for Environmental Health, CDC.
References
- Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from 3,4 methylenedioxymethamphetamine ("ecstasy"). Lancet 1992;340:384--7.
- Rogers G. The harmful health effects of recreational ecstasy: a systematic review of observational evidence. Health Technol Assess 2009;13:iii--iv, ix--xii, 1--315.
- Gross SR, Barrett SP, Shestowsky JS, Pihl RO. Ecstasy and drug consumption patterns: a Canadian rave population study. Can J Psychiatry 2002;47:546--51.
- Kalant H. The pharmacology and toxicology of "ecstasy" (MDMA) and related drugs. CMAJ. 2001;165:917--28.
- Bahora M, Sterk CE, Elifson KW. Understanding recreational ecstasy use in the United States: a qualitative inquiry. Int J Drug Policy 2009;20:62--9.
- Degenhardt L, Copeland J, Dillon P. Recent trends in the use of "club drugs": an Australian review. Subst Use Misuse 2005;40:1241--56.
- National Drug Intelligence Center. Raves. Johnstown, PA: US Department of Justice, National Drug Intelligence Center; 2001. Available at http://www.justice.gov/ndic/pubs/656/656p.pdf. Accessed April 15, 2010.
- Drug Abuse Warning Network. Detailed tables: national estimates, drug-related emergency department visits for 2004--2008. Rockville, MD: US Department of Health and Human Services, Office of Applied Studies, Substance Abuse and Mental Health Services Administration; 2009. Available at http://dawninfo.samhsa.gov/data. Accessed June 3, 2010.
- Partnership for a Drug-Free America, Metlife Foundation. 2009 parents and teens attitude tracking study report. New York, NY: Partnership for a Drug-Free America and Metlife Foundation; 2010. Available at http://www.drugfree.org/files/pats_full_report_2009_pdf. Accessed April 15, 2010.
- CDC. CDC's issue brief: unintentional drug poisoning in the United States. Atlanta, GA: US Department of Health and Human Services, CDC; 2010. Available at http://www.cdc.gov/homeandrecreationalsafety/poisoning/brief.htm. Accessed April 14, 2010.
What is already known on this topic?
Ecstasy (3,4-methylenedioxymethamphetamine [MDMA]) is an illegal amphetamine derivative, often used at raves (all-night dance parties with electronic music) as a stimulant and hallucinogen.
What is added by this report?
This report is the first public health investigation of a cluster of MDMA overdoses at a rave. A total of 18 cases of MDMA overdose were identified within 12 hours of the rave. Overall use of the drug in Los Angeles County increased during 2005--2009.
What are the implications for public health practice?
Injury prevention, substance abuse prevention, and emergency preparedness personnel can be involved in advance to develop overdose prevention and response strategies for mass gatherings such as raves, and attendees should be warned about the risks of MDMA and other drugs used at similar events.
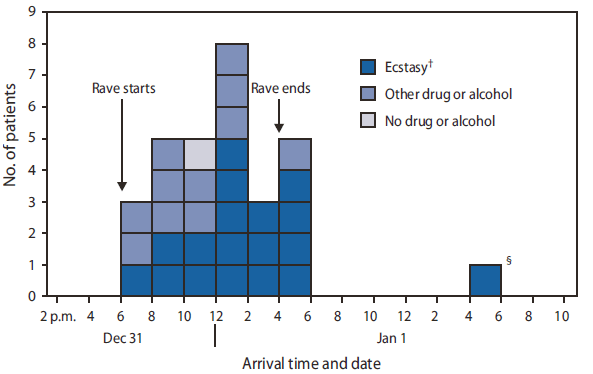
* Chief complaints for 29 patients were characterized as altered mental status, alcohol intoxication, or suspected drug overdose; one patient was transported for trauma.
† 3,4-methylenedioxymethamphetamine (MDMA).
§ Patient consumed additional ecstasy after the rave.
Alternate Text: The figure above shows the number, drug use, and arrival times of rave attendees transported to emergency departments (N = 30) in Los Angeles County, California, December 31, 2009-January 1, 2010 within 12 hours of the end of the event. One patient was transported for trauma, and the other 29 for various drug and/or alcohol intoxications. All but one of the patients arrived at emergency departments within 12 hours of when the rave began.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
